Nutritional Aspects, Pros and Cons of Nutrients-Rich Foods (Fruits and Vegetables) in Response to Stem Cells Transplantation
Fruits and vegetables are among the foods considered as naturally nutrient-rich in addition to common everyday meals. Plant-based diet entailing high intake of these nutrient-rich plant derived foods can provide numerous bioactive constituents. Several of such compounds may modify a multitude of processes that are related to numerous chronic diseases in humans. Human bone marrow can be damaged by disease, chemotherapy or radiation. Therefore, a patient is subjected to stem cell transplantation (SCT) to infuse healthy stem cells that replace damaged ones. Therefore, the purpose of this mini-review is to provide insight of research on the nutritional aspects including pros and cons of nutrient-rich foods (fruits and vegetables) in response to SCT. The review revealed that, multiple myeloma, overweight, sarcopenia and low oxidative stress levels are among the most prevalent conditions/risk factors for complications and increased relapse/non-relapse mortality in patients eligible for SCT. Patients recovering from SCT require more calories and twice as much protein in diets than healthy individuals of similar age and gender. Apple fruit and vegetables such as potatoes, carrots and beetroots were most frequently consumed by patients subjected to allogeneic bone marrow (allo-BMT). While, green vegetables like spinach and broccoli, onion, garlic, beans and peas as well as grapefruits, raspberries, grapes, oranges and strawberries were rarely consumed by patients under allo-BMT. Neutropenic (low-microbial) diets are designed to reduce ingestion of pathogens through the exclusion of foods such as fruits and vegetables that can be vectors of bacteria. In contrast to the neutropenic diet, natural diet plus vegetable-dairy i.e., soy-whey blended protein as well as the modified BMT diet allowed fresh fruits and vegetables without visible damage (e.g., cuts and bruises) and must be well washed under cold running water. Despite the diet restrictions (i.e., towards foods which pose the greatest risk both in hospitals and at home), further research studies with respect to fruit and vegetables are recommended to establish specific prescriptions including optimum quantities and time of consumption by the immunosuppressed patients/those subjected to SCT. Adequate data would be ideal as a tool to aid professionals including nutritionists to safely recommend foods that can be ingested by patients under SCT.
Introduction
In addition to common everyday meals, naturally nutrient-rich or nutrient-dense foods including whole vegetables and fruits provide substantial amounts of vitamins, minerals and other nutrients relative to their calorie content [1]. Other kinds of foods falling into this category include whole, fortified and fiber-rich grain foods, 100% fruit juice, fat-free and low-fat milk, cheese and yogurt, lean meats, skinless poultry, fish, eggs, spices and nuts that are prepared without added solid fats, sugars, and sodium [2]. Fruits and vegetables entail a diverse set of plant-derived foods that differ significantly in content of energy, nutrients, dietary fiber, vitamins, minerals and phytochemicals [3, 4]. Plant-based diet entailing high intake of these nutrient-rich plant derived foods can provide more than 25,000 bioactive constituents [5]. Several of such constituents may adjust a multitude of processes that are related to numerous chronic diseases in humans. Optimal amount of dietary fiber intake is associated to reduce incidence of cardiovascular disease [3]. Antioxidant, anti-inflammatory and several other protective mechanisms in human body are also a function of fruits and vegetables [6, 7, 8, 9, 10, 11, 12]. Human stem cells can be destroyed by disease, chemotherapy (chemo), or radiation. Therefore, a procedure in which a patient receives healthy stem cells to replace damaged stem cells is known as stem cell transplantation (SCT) [13, 14]. The transplant procedure may also be called bone marrow transplant (BMT), peripheral blood stem cell transplant (BCT), cord blood transplant or hematopoietic stem cell transplant (HSCT) depending on the source of stem cells. A therapeutic form for treatment of bone marrow diseases and other neoplasms is known as HSCT. Hematopoietic (blood-forming) are the immature cells that live in the bone marrow (i.e., a spongy tissue inside bones stem cells) and have ability to turn into red blood cells, white blood cells, and platelets.
Autologous, allogeneic, reduced-intensity and syngeneic are the major types of SCT [13, 14]. Autologous SCT uses the patient’s own stem cells (Figure 1a), whereby these cells are removed, treated and returned to the body after a conditioning regimen (a prescribed medical treatment for the promotion or restoration of health). Allogeneic SCT uses stem cells from a donor (i.e., a family member or someone who is not related to the patient) (Figure 1b). Autologous SCT becomes advantageous following the effects of the conditioning treatment, while eradication of the underlying disease by allogeneic SCT is significantly contributed by the donor immune system through development of graft vs leukaemia or tumour effect [15]. In reduced-intensity SCT, like allogeneic SCT, the stem cells are from a healthy person (the donor), but a less intensive chemotherapy is given to the patient. Syngeneic SCT is rare (much less common) because it’s only used on identical twins (donor twin and recipient twin must have identical genetic makeup and tissue type).
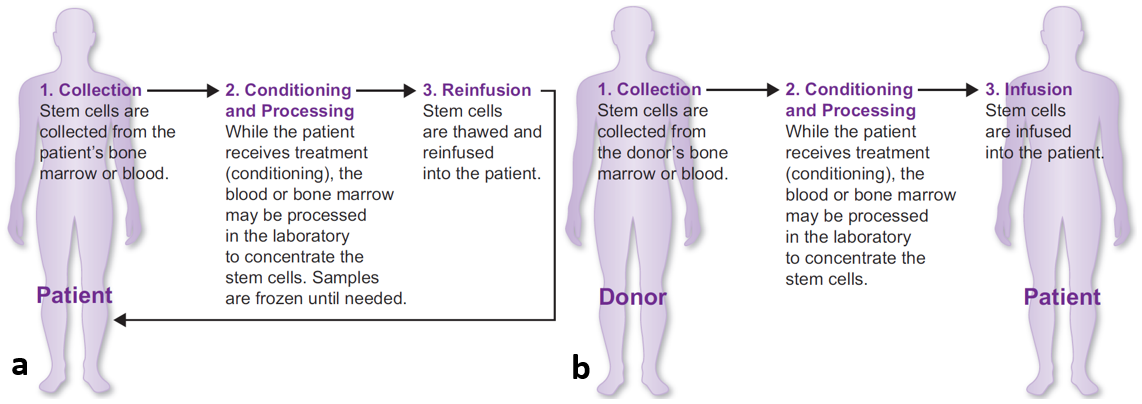
Source: LRF [14]. Figure 1: Demonstration of the major types of SCT (a) Autologous and (b) Allogeneic.
The stem cells replacement is given into a vein, much like a blood transfusion. However, in order to prepare the body for SCT, the patient may undergo “conditioning treatment” which involves receipt of high doses of chemotherapy, and sometimes radiation therapy (Figure 2). In some occasions, the effects of toxicity may decrease oral intake for an extended period of time, thus nutritional status and nutritional intake monitoring is a vital part of supportive care for patients receiving SCT [12]. After conditioning treatment, the stem/blood-forming cells are infused into the patient’s bloodstream through the bone marrow, and begin the process of “engraftment” (Figure 2). This process involves formation of new, healthy red blood cells, white blood cells, and platelets [14]. Stem cells from particular sources can be harvested, processed, and conserved in blood banks for later use or transported for transplant (Figure 2).
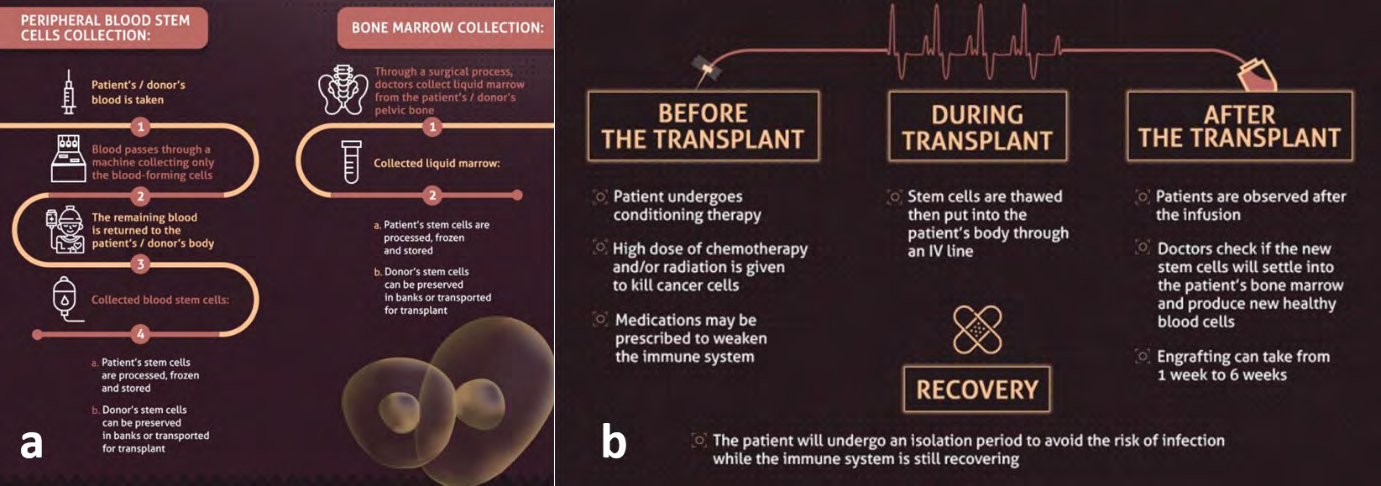
Source: Hildreth C [16]. Figure 2: The stem cells process (a) collection (b) transplantation and recovery phases.
There are numerous diseases that can be treated with a blood SCTs [9, 17, 18]. Autologous SCT can be used to treat a person who is diagnosed with amyloidosis or testicular cancer (germ cell tumors). Allogeneic transplantation can be used to treat a person who is diagnosed with acute leukemia, amegakaryocytosis or congenital thrombocytopenia, aplastic anemia or refractory anemia, chronic lymphocytic leukemia, familial erythrophagocytic, lymphohistiocytosis, myelodysplastic syndrome (MDS), myeloproliferative disorders such as myelofibrosis, and severe aplastic anemia osteopetrosis, paroxysmal nocturnal hemoglobinuria. Patients with an immune deficiency disease (e.g., Wiskott Aldrich Syndrome or SCIDS), genetic or inherited disorders (such as sickle cell disease or thalassemia), and solid tumor (like neuroblastoma, breast carcinoma, childhood sarcomas). Scleroderma (non-malignant diseases), haematological malignancies are also among indications for BMT and BCT. Autoimmune disease (i.e., multiple sclerosis) can also be a treated through BCT option [19]. Depending on the subtype of disease and how advanced it is, people diagnosed with Hodgkin lymphoma, non-Hodgkin lymphoma or multiple myeloma may be used to treat either through autologous or allogeneic SCT [18]. Nevertheless, these does not necessitate SCT to all kind of patients but can be initiated for patients whose quality of life can be improved by the procedure, or patients who have a high risk of such diseases reoccurring (relapsing) after less-intensive treatment, or who have already relapsed. Patients undergoing hematopoietic stem cell transplantation (HSCT) normally present lowered or deteriorated nutritional status, caloric and protein intake adequacy during the hospitalization period [8]. Therefore, more calories and twice as much protein in diets are required by the recovering HSCT patients than healthy individuals of similar age and gender. Moreover, gastro-intestinal side- effects such as nausea, repeated vomiting, mouth complaints and anorexia [8, 9, 10] oropharyngeal mucositis, changes in taste, diarrhoea and esophagitis are common with stem cell transplantations (SCT) [11]. These may lead in low calorie- protein intake, fall in absorption of nutrients, and higher nutritional needs [11], however the intensity and period may vary per conditioning treatment [12]. Despite the elaborated benefits of SCT on disease management and control, nutrition through proper diet is inevitable to the recovering transplant patients. Therefore, the purpose of this mini- review is to provide insights of research on the nutritional aspects including pros and cons of nutrient-rich foods (fruits and vegetables) in response to SCT.
Nutritional Risk Factors in Patients Eligible for SCT
Various aspects are normally investigated to establish the nutritional condition in patients eligible for SCT. The aspects include but not limited to demographic, clinical, patient-generated global subjective assessment findings, anthropometric indicators, nutritional status measurements (food intake) and oxidative stress levels. Multiple myeloma was among the most prevalent condition of the patients eligible for HSCT [20]. Also, based on body mass index, a large proportion of patients eligible for HSCT were overweight, sarcopenic and had low oxidative stress levels. Sarcopenia was associated with risk of cardiovascular disease (based on waist circumference, conicity index and percentage of body fat), hip-to-waist ratio, muscle strength depletion (lean mass deficiency), food intake changes, reduced functional capacity, self-reported good nutritional status, inadequate vitamin B6 and manganese intake but not with oxidative stress [20]. Similarly, Akbulut G [9] associated body weight (i.e., obesity: BMI≥ 30kg/m2 or undernourishment: BMI<18.5kg/m2) as risk factors for complications and increased relapse/ non-relapse mortality in HSCT patients on admission. Also, patients subjected to HSCT are usually at higher risk for malnutrition in the phase before transplantation and afterward [9]. The study by Liu P, et al. [21] also found that the nutritional risk and malnutrition were significantly high in patients subjected to HSCT after being diagnosed with hematological diseases, with some patients already exhibited nutritional deficiencies/risks. The extensive screening and evaluation of nutritional risks and status was based on four nutritional screening tools in combination with body measurements [21]. All the tools namely; nutritional risk screening 2002 (NRS-2002), mini nutritional assessment (MNA), subjective global assessment (SGA) and malnutrition universal screening tools (MUST) indicated that less patients were at nutritional risks (malnourished) post- than pre- HSCT. Weight, hip circumference, waist-hip ratio, calf circumference, mid-upper arm circumference, and suprailiac skinfold thickness were also significantly reduced post- than pre-HSCT.
Nutritional Intake and Diet Quality Relative to SCT
Assessment of nutritional intake and diet quality entails identification of key foods/nutrients, and adequacy of nutrient intake. Moreover, compliance/adherence to the dietary advice and guidelines, particularly information on diet enrichment of recovering patients with energy, protein or micronutrients post-SCT stage. Children and adolescents under allogeneic HSCT got their energy needs met by mouth at the time of hospitalization, while more prevalence of parental nutritional and enteral nutrition from the 7th day after cell infusion, and the increase in caloric intake by mouth was experienced later on from 21st day after cell infusion [22]. A summary of nutrient-rich foods to patients under SCT is presented in (Table 1).
| Condition | Type of SCT | Source | |
|---|---|---|---|
| Vegetables | Allowed well washed raw vegetables & cooked potatoes. Prohibited dried pulses e.g., beans, chickpeas and lentils | HSCT | [9] |
| Vegetables | Prohibited lettuce and carrot tart to 6 months post-SCT; cucumbers, sauerkraut, marinated mushroom, salads/casseroles, potato, pasta, rice entailing raw vegetables and mayonnaise | Allo-BMT | [23] |
| Vegetables | Allowed raw and canned vegetables | HSCT | [24] |
| Vegetables | Allowed canned vegetables; raw vegetables with a peeled skin i.e., cucumber, onion; cooked vegetables; immediately consumed soup and tomato sauce. Prohibited raw vegetables with skin/thin skin i.e., carrot, tomato, mushrooms, industrial packaged salads without salad dressing | HSCT | [25] |
| Vegetables | vegetable-Dairy i.e., Soy-whey blended protein | Allogeneic SCT/ Peripheral blood SCT | [26] |
| Fruits | Allowed canned and frozen fruit, well-washed and peeled fresh fruit (if neutrophil count is <1500 mm3). Prohibited dried fruits; berry fruits i.e., strawberries, raspberries, blackberries, grapes (unless peeled) | HSCT | [9] |
| Fruits | Allowed raspberries and strawberries | HSCT | [10] |
| Fruits | Prohibited raw fruits (that cannot be peeled), chopped, oleaginous fruits, dried fruits, fruits preserved in the house, uncooked fruit soup | Allo-BMT | [24] |
| Fruits | Allowed cooked, canned, raw thick-skinned, raw thin-skinned fruits i.e., grapes, strawberries, mulberries & jaboticabal | HSCT | [27] |
| Fruits | Allowed cooked fruits; cooked dry fruits; raw fruits with a peeled thick-skin i.e., apple, pear, pineapple, avocado; industrial sorbet in industrial packaging. Prohibited raw frozen fruits; raw fruits with skin/thin-skin i.e., red fruits, peach, apricot; all forms of grapefruit | HSCT | |
| Juices | Allowed fruit juices (if neutrophil count is <1500 mm3). Prohibited unpasteurized fruit juice | HSCT | [9] |
| Juices | Allowed pasteurized fruit juice (packed in cartons) | HSCT | [24] |
Table 1: Nutrient-rich foods and their conditions towards patients subjected to SCT.
Ziolko E, et al. [23] found that the commonly consumed foods by patients subjected to allogeneic bone marrow transplantation (allo-BMT) included fruits and vegetables. Apple fruit and vegetables such as potatoes, carrots and beetroots were most frequently consumed by the patients [23]. Green vegetables like spinach and broccoli, onion, garlic, beans and peas as well as grapefruits, raspberries, grapes, oranges and strawberries were rarely consumed by patients under allo-BMT [23]. The effects on change in dietary habits was marginal, despite that all patients obtained the dietary education post-allo-BMT. Consumption of instant foods, insufficient fluid, fruit and vegetable intake, sweets and fried food were the most frequent failures to patients post- allo-BMT. Catabolic processes, comprehensive therapeutic regimen and increasing energy demand were associated to reduction in BMI post-allo-BMT [23].
Nevertheless, there are some diet restrictions (i.e., towards foods which pose the greatest risk both in the hospital and at home) to immunosuppressed patients particularly those subjected to HSCT treatment [9, 24]. Such restrictions include; unwashed and unpeeled raw fruits, damaged fruit, berry fruits (strawberries, raspberries, blackberries), grapes (unless peeled), unpasteurized fruit juice and dried fruits. Moreover, cheeses containing chili peppers, and/or other uncooked vegetables, salad from delicatessens; commercial salsas stored in refrigerated case, dried pulses (e.g., beans, chick peas and lentils), herbs and spices should not be sprinkled on food after cooking. On the other hand, all cooked, frozen, canned, or fresh vegetables and potatoes, well-washed raw vegetables, dried herbs and spices (packaged) (if added before; not after cooking) as well as canned and frozen fruit (except for berry fruits), fruit juices; well-washed and peeled fresh fruit (if neutrophil count is <1500 mm3) are allowed. Such diet was also advised to autologous SCT recipients to follow for about 3 months after chemotherapy, while for allogeneic SCT recipients the diet was to be followed until 1-year post-SCT, or prolonged if still under immunosuppressants for graft-versus-host disease (GVHD) [9].
Infectious complication such as GVHD accounts for a great effect on the quality of life to patients as it is among the major cause of allogeneic HSCT-related morbidity and mortality [27, 28]. GVHD is due to activation of T cells that recognize host antigens as non-self, leading to an autoimmune reaction in patients’ organs i.e., skin, lungs, liver, gastrointestinal tract (GIT), thymus, hematopoietic system, and likely the central nervous system. Patois C, et al. [25] suggested that, the risks of contamination can be lowered by having condiments and canned vegetables or fruits in small containers because the container will not stay open for a long time and will be quickly consumed in its entirety. According to Pereira AZ, et al. [28] several nutritional interventions may be directed towards improving and controlling gastrointestinal symptoms like early satiety.
This includes making the patient aware of the importance of food, performing diet fractionation (from six to eight meals/day), modification of dietary fiber by cooking and/or grinding to reduce satiety (unpeeled fruit, cooked vegetables, soups and liquid juices) and increasing the caloric and protein density of meals. Foods become safe from bacteria as the later can be destroyed through cooking [29]. Therefore, evasion of foods considered to be loaded with bacteria (i.e., raw fresh fruits and vegetables) is believed to lower the risk of infections in patients under SCT. Low-microbial diets designed to reduce ingestion of pathogens through the exclusion of foods that can be vectors of bacteria are known as neutropenic diets (ND) [11]. Nevertheless, HSCT recipients who received ND had higher rate of infections from organisms colonizing the gastrointestinal tract [25]. Thus, confirming that the restrictive diets cannot completely out compete the more liberalized diets in preventing infections. Previously, the NDs comprised of foodstuffs sterilized by autoclaving or irradiation. Thereafter a modified diet of cooked foods prepared through appropriate techniques of hygiene, storage and cooking was adopted following poor intake by patients.
A comparative study by Taggart C, et al. [10] between a neutropenic diet and a food safety-based diet in pediatric patients subjected to HSCT revealed that, there was no difference in the perceived food cravings, nausea, diet limitations, and subjective quality of life between the groups of patients. The study demonstrated a non-inferiority of the modified BMT diet over the traditional neutropenic diet. In contrast to the neutropenic diet which said no to consumption of fresh, canned, and frozen fruits or vegetables, the modified BMT diet was composed of a set of instructions such as
- Allowed fresh fruits and vegetables mainly raspberries and strawberries
- Fresh fruit and vegetables must be well washed under cold running water and
- Families are encouraged to select fruit and vegetables without visible damage (e.g., cuts and bruises).
Patients diagnosed with acute leukemia (a type of cancer of the blood and bone marrow that affects white blood cells) exhibit severe protein loss i.e., protein-energy malnutrition (PEM) and abnormally low concentrations of plasma proteins i.e., albumin and globulin and skeletal muscle wasting [26]. Ren G, et al. [26] investigated the effects soy-whey protein blend ingestion in promoting muscle protein synthesis (MPS), whereby patients were divided into a natural diet plus soy-whey blended protein (BP) group and the natural diet only (ND) group. According to Ren G, et al. [26] protein and energy intake decreased significantly after SCT in both groups. However, BP improved PEM status, muscle mass and increased the levels of serum albumin, globulin and serum total protein to varying levels in leukemia patients. Patients subjected to BP before SCT exhibited vivid increase in arm muscle area and had significantly higher gripping power value than ND group. Patients in the BP group had shorter average time (12.2±2.0 days) to stem cell engraftment than for ND group (15.1±2.9 days).
Muscle-related indicators mainly; anthropometric variables, muscle strength and serum protein were significantly decreased in ND group patients than in BP group. Chen G, et al. [30] found that, patients subjected to SCT were highly motivated to follow food safety recommendations than organ transplant patients who were more reluctant to risky foods consumption. These patients also understood their exposure to foodborne illness, and were equipped with knowledge and behavior changes essential to protect their health. Similarly, receptivity of participants in a dietary intervention was higher for Adult HCT survivors within 2 years post-HSCT than those with over 2 years. Adult HSCT survivors reported less-than-optimal adherence to good quality diet [30], dietary advice/guidelines and had numerous shortfall nutrient intakes, but their willingness to participate in a dietary intervention was relatively high [31]. In addition, lower quality of diet attributed the change in taste for foods, also inadequate intakes of magnesium, calcium, vitamins (A, C, and D) and fiber (at 8.9 g per 1000 kcal/day) dropped far lower than the sufficient recommended intake of 14g per 1000 kcal/day [31].
Conclusion
The review provided highlights on the nutritional aspects of patients as well as potentiality of nutrient-rich foods (fruits and vegetables) in response to SCT. Multiple myeloma, overweight, sarcopenia and low oxidative stress levels are among the most prevalent conditions/risk factors for complications and increased relapse/non-relapse mortality in patients eligible for SCT. More calories and twice as much protein in diets is require by patients recovering from SCT than healthy individuals of similar age and gender. Apple fruit and vegetables such as potatoes, carrots and beetroots were most frequently consumed by patients subjected to allogeneic bone marrow (allo-BMT). While, green vegetables like spinach and broccoli, onion, garlic, beans and peas as well as grapefruits, raspberries, grapes, oranges and strawberries were rarely consumed by patients under allo- BMT. Neutropenic (low-microbial) diets are designed to reduce ingestion of pathogens through the exclusion of foods such as fruits and vegetables that can be vectors of bacteria. In contrast to the neutropenic diet, natural diet plus vegetable-dairy i.e., soy-whey blended protein as well as the modified BMT diet allowed fresh fruits and vegetables without visible damage (e.g., cuts and bruises) and must be well washed under cold running water. Sufficient vitamin, energy, fiber or antioxidants needs could not be achieved with inadequate food intake. Therefore, good nutrition is essential for immune and bone marrow reconstitution following SCT. The food safety-based diet in compliance/adherence to the dietary advice and guidelines, particularly information on diet enrichment of recovering patients with energy, protein or micronutrients post-SCT stage is safe and offers a greater variety of food, which may assist in the transition to a normal diet. Dietary guidance is inevitable, this enhances reduction of microbial exposure, optimize nutrient consumption and energy intake for patients subjected to SCT. Despite the diet restrictions (i.e., towards foods which pose the greatest risk both in hospitals and at home), further research studies with respect to fruit and vegetables is recommended to establish specific prescriptions including optimum quantities and time of consumption by the immunosuppressed patients/ those subjected to SCT. Adequate data would be ideal as a tool to aid professionals including nutritionists to safely recommend foods that can be ingested by patients under SCT.
References
-
Nicklas TA, Drewnowski A, O Neil CE (2014) The nutrient density approach to healthy eating: challenges and opportunities. Public Health Nutr 17(12): 2626-2636.
-
Drewnowski A, Dwyer J, King JC, Weaver CM (2019) A proposed nutrient density score that includes food groups and nutrients to better align with dietary guidance. Nutr Rev 77(6): 404-416.
-
Slavin JL, Lloyd B (2012) Health benefits of fruits and vegetables. Adv Nutr 3(4): 506-516.
-
Rahman MM, Mosaddik A, Alam AK (2021) Traditional foods with their constituent’s antiviral and immune system modulating properties. Heliyon 7(1): e05957.
-
Carlsen MH, Halvorsen BL, Holte K, Bohn SK, Dragland S, et al. (2010) The total antioxidant content of more than 3100 foods, beverages, spices, herbs and supplements used worldwide. Nutr J 9(1): 1-3.
-
Oz AT, Kafkas E (2017) Phytochemicals in fruits and vegetables. Waisundara V Superfood and functional food. Intech Open, London, UK, pp: 175-184.
-
Jideani AI, Silungwe H, Takalani T, Omolola AO, Udeh HO, et al. (2021) Antioxidant-rich natural fruit and vegetable products and human health. Inter J Food Properties 24(1): 41-67.
-
Garios RS, Oliveira PM, Aguiar AS, Luquetti SC (2018) Caloric and protein intake in different periods of hospitalization of patients undergoing hematopoietic stem cell transplantation. Hematol Transfus Cell Ther 40(4): 332-338.
-
Akbulut G (2013) Medical nutritional therapy in hematopoietic stem cell transplantation (HSCT). Intern J Hem Oncol 23(1): 55-65.
-
Taggart C, Neumann N, Alonso PB, Lane A, Pate A, et al. (2019) Comparing a neutropenic diet to a food safety-based diet in pediatric patients undergoing hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 25(7): 1382-1386.
-
Albertini SM (2012) Neutropenic diets in hematopoietic stem cell transplantation. Rev Bras Hematol Hemoter 34(2): 73-79.
-
Iestra JA, Fibbe WE, Zwinderman AH, Van Staveren WA, Kromhout D (2002) Body weight recovery, eating difficulties and compliance with dietary advice in the first year after stem cell transplantation: a prospective study. Bone Marrow Transplant 29(5): 417-424.
-
Norville R, Tomlinson D (2010) Hematopoietic Stem Cell Transplantation. In: Tomlinson D, Kline NE, et al. (Eds.), Pediatric Oncology Nursing. Pediatric Oncology. Springer, Berlin, Heidelberg, pp: 243-267.
-
LRF (2016) Understanding the Stem Cell Transplantation Process: A Guide for Patients, Caregivers, and Loved Ones. Lymphoma Research Foundation (LRF), New York, USA, pp: 1-60.
-
Balassa K, Danby R, Rocha V (2019) Haematopoietic stem cell transplants: principles and indications. Br J Hosp Med 80(1): 33-39.
-
Hildreth C (2020) Stem Cell Transplants: What To Know About This Life-Saving Procedure. BioInformant.
-
Hatzimichael E, Tuthill M (2010) Hematopoietic stem cell transplantation. Stem cells cloning: 3: 105-117.
-
Oliveira MC, Elias JB, Moraes DA, Simões BP, Rodrigues M, et al. (2021) A review of hematopoietic stem cell transplantation for autoimmune diseases: multiple sclerosis, systemic sclerosis and Crohn’s disease. Position paper of the Brazilian Society of Bone Marrow Transplantation. Hematol Transfus Cell Ther 43(1): 65- 86.
-
Ali N, Adil SN, Shaikh MU (2015) Autologous hematopoietic stem cell transplantation-10 years of data from a developing country. Stem Cells Transl Med 4(8): 873-877.
-
Viana AC, Aguiar AP, Rodrigues BC, Mendonça PD, Maia FM (2020) Evaluation of nutritional risk factors in hematopoietic stem cell transplantation-eligible patients. Einstein (São Paulo) 18: eAO5075.
-
Liu P, Wang B, Yan X, Cai J, Wang Y (2016) Comprehensive evaluation of nutritional status before and after hematopoietic stem cell transplantation in 170 patients with hematological diseases. Chin J Cancer Res 28(6): 626-633.
-
Lewandowski CG, Daudt LE, Keller Jochims AM, Paz A, Mello ED (2019) Nutritional aspects in allogeneic hematopoietic stem cell transplantation in children and adolescents in a tertiary hospital. Nutr Hosp 36(1): 20- 24.
-
Ziolko E, Pamula AK, Zlotkowska R, Wyrozumska TB, Lampa M, et al. (2016) The Dietary Habits in Patients after the Allogeneic Bone Marrow Transplantation (Allo- BMT). Health Science Journal 10(3): 1-4.
-
Vicenski PP, Alberti P, Amaral DJ (2012) Dietary recommendations for immunosuppressed patients of 17 hematopoietic stem cell transplantation centers in Brazil. Rev Bras Hematol Hemoter 34(2): 86-93.
-
Patois C, Chen Y, Meiselman HL, Barraco F, Giboreau A (2021) Designing food and meals for bone marrow transplant patients with compromised immunity. International Journal of Food Design 6(1): 27-51.
-
Ren G, Zhang J, Li M, Yi S, Xie J, et al. (2017) Protein blend ingestion before allogeneic stem cell transplantation improves protein-energy malnutrition in patients with leukemia. Nutr Res 46: 68-77.
-
Trifilio S, Helenowski I, Giel M, Gobel B, Pi J, et al. (2012) Questioning the role of a neutropenic diet following hematopoetic stem cell transplantation. Biol Blood Marrow Transplant 18(9): 1385-1390.
-
Pereira AZ, Vigorito AC, Almeida AM, Candolo AA, Silva AC, et al. (2020) Brazilian Nutritional Consensus in Hematopoietic Stem Cell Transplantation: Graft-versus- host disease. Einstein (São Paulo) 18: eAE4799.
-
Wolfe HR, Sadeghi N, Agrawal D, Johnson DH, Gupta A (2018) Things We Do For No Reason: Neutropenic Diet. J Hosp Med 13(8): 573-576.
-
Chen G, Kendall PA, Hillers VN, Medeiros LC (2010) Qualitative studies of the food safety knowledge and perceptions of transplant patients. J Food Prot 73(2): 327-335.
-
Farhadfar N, Kelly DL, Mead L, Nair S, Colee J, et al. (2020) Dietary intake and diet quality of hematopoietic stem cell transplantation survivors. Biol Blood Marrow Transplant 26(6): 1154-1159.
- Research Progress of Induced Pluripotent Stem Cells and Their Clinical Application Prospects
- Nishan Al-Kamal is the Starting Point of A Feminist Scientist
- Current Concepts and Future Perspectives of Stem Cell Therapy in Peripheral Arterial Disease
- Stem Cell and Oxidative Stress-Inflammation Cycle
- Adipose Derived Mesenchymal Stem Cells Origin, Characteristics and Promises
- Mitochondria Targeted Antioxidants can Improve In Vitro Embryo Production in Buffalo