Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
Artificial intelligence (AI) has rapidly emerged as a powerful tool in the global effort to prevent and control infectious diseases. With the growing burden of pandemics, antimicrobial resistance (AMR), and travel-related outbreaks, traditional public health responses face significant challenges in speed, scale, and coordination. AI technologies—ranging from machine learning (ML) and natural language processing (NLP) to deep learning and generative models—offer new capabilities across surveillance, early outbreak detection, diagnostics, modeling, vaccine development, public communication, and resource allocation. This review synthesizes the expanding applications of AI in infectious disease prevention and control and highlights its transformative potential in improving preparedness and response. AI enables real-time integration of heterogeneous data sources, supports precision diagnostics in low-resource settings, accelerates vaccine target identification, and enhances public health communication during crises. However, its implementation is not without challenges. These include data quality and bias, privacy and security, technical limitations, transparency and trust, ethical concerns, misinformation, regulatory gaps, cost and infrastructure constraints, and system fragmentation. To maximize AI’s benefits, policy frameworks should promote equitable data access, interdisciplinary collaboration, and inclusive governance mechanisms. Technical development should also prioritize transparency, adaptability, and contextual relevance. AI has the potential to reshape global infectious disease prevention and control, but realizing its promise requires deliberate, coordinated efforts to overcome structural, ethical, and technical barriers.
Abbreviations
AI: Artificial Intelligence; AMR: Antimicrobial Resistance; ML: Machine Learning; NPL: Natural Language Processing; IDVI: Infectious Disease Vulnerability Index; VAEs: Variational Autoencoders; MPL: Multi-layered perceptron; GNNs: Graph Neutral Networks; GANs: Generative Adversarial Networks;
CNNs: Convolutional Neural Networks
Introduction
Artificial intelligence (AI), broadly defined as the performance of tasks by computer programs that typically require human intelligence, is increasingly recognized as a transformative force in global health [1]. Its applications span disease surveillance, behavioural risk analysis, resource optimization, tailored health communication, and combating misinformation [2].
These capacities are urgently needed, as infectious diseases remain a major global health threat. Diseases such as HIV/AIDS, tuberculosis, and malaria, along with pandemics like COVID-19, continue to cause widespread mortality and socioeconomic disruption [3]. In addition, the rise of antimicrobial resistance (AMR) represents a silent yet escalating global crisis, [4] while international travel accelerates the spread of emerging pathogens [5]. These challenges highlight the need for faster, smarter, and more coordinated public health responses. AI is uniquely positioned to address these gaps by identifying high-risk patients, predicting outbreak dynamics, and informing tailored prevention and control strategies [6]. However, there are still a series of urgent problems and challenges to be solved in order to better apply AI to the prevention and control of infectious diseases, including data quality and bias issues, technical limitations, ethical dilemmas, regulatory gaps, and systemic barriers such as inadequate infrastructure, high costs, and workforce shortages. This review examines the expanding role of AI in infectious disease prevention and control, focusing on its opportunities and transformative potential, implementation challenges, and policy implications.
Opportunities and Transformative Potential
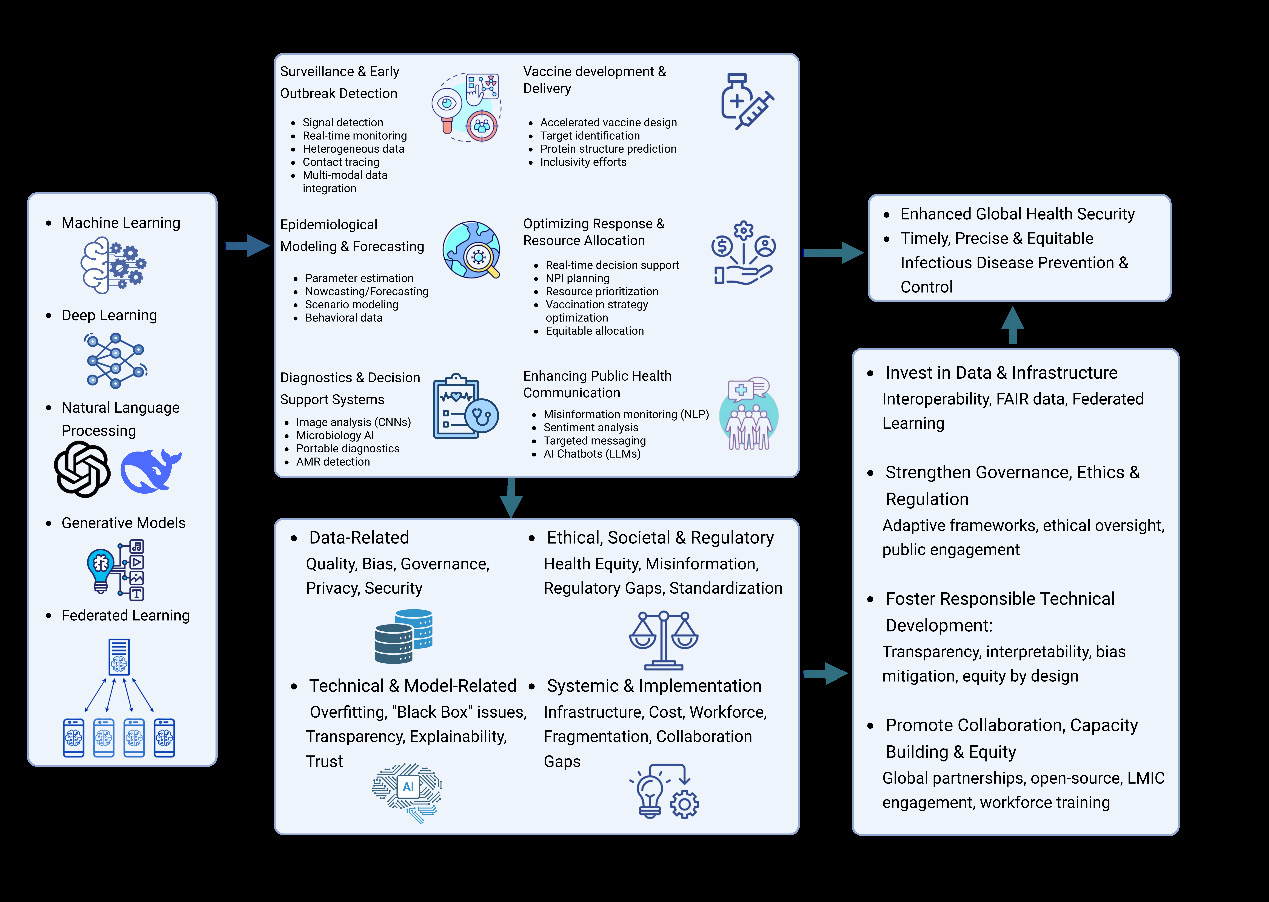
AI holds significant potential across multiple domains of infectious disease prevention and control, including enhancing surveillance and early outbreak detection, advancing epidemiological modeling and forecasting, supporting diagnostics and decision-making systems, accelerating vaccine development and distribution, optimizing response strategies and resource allocation, and strengthening public health communication.
Surveillance and Early Outbreak Detection
AI has revolutionized real-time infectious disease surveillance by enabling the timely detection of outbreak signals from complex and heterogeneous data sources. Traditional surveillance systems are often limited by reporting delays and fragmented data streams, while AI algorithms—particularly those using natural language processing (NLP) and machine learning (ML)—can rapidly identify abnormal patterns across digital platforms, news sources, and social media [7].
AI-powered platforms such as HealthMap and BlueDot exemplify the capabilities of NLP-based surveillance systems.
HealthMap processes large volumes of global web-based data to identify early signs of outbreaks, successfully flagging events like H1N1 and COVID-19 ahead of conventional systems [7]. BlueDot integrates global air travel patterns, climate change indicators, and zoonotic spillover data using ML and NLP to track more than 100 diseases [8] It was among the first platforms to identify the emergence of SARS-CoV-2 in December 2019 [6].
AI also facilitates the real-time monitoring of syndromic and behavioural data. Wearables and biosensors—such as smartwatches and microphones—can detect early physiological changes, including elevated resting heart rates or unusual coughing patterns, that serve as proxies for illness before clinical diagnosis [9]. The population aggregate of this signal can warn public health officials of an impending outbreak [7]. Similarly, public health researchers have used AI to analyse data from social media and search engine queries to monitor symptom surges and community-level concern [10].
Integrated modeling approaches further enhance anticipatory surveillance. AI-based systems can combine travel data, phone-based tracking, and epidemiological signals to detect and characterize outbreak risks at both local and global scales [3] One example is the Infectious Disease Vulnerability Index (IDVI), which synthesizes national data on governance, healthcare capacity, and demographics to estimate country-level preparedness, with higher scores reflecting a better ability to respond to a disease outbreak [11, 12] In parallel, mobile phone–based cyber surveys have been used to identify people with mild symptoms and track disease spread in real time [13].
AI has also advanced digital surveillance and early outbreak detection through mobile sensor-based systems and contact tracing technologies. ML-driven platforms such as the Epidemic Watch System (EWS) utilize smartphone sensor data and algorithms to monitor contacts and classify infection risks in real time [14]. These systems enhance early detection capabilities and support public health decision- making. To improve accuracy, researchers developed multi- sensor fusion models that reduce false positives by 95% and increase detection accuracy by 62% [15]. Furthermore, privacy-preserving ML frameworks have been proposed to enable scalable and ethical digital surveillance during future outbreaks [16].
Epidemiological Modeling and Forecasting
Beyond real-time surveillance, AI also plays a vital role in the modeling and forecasting of infectious disease outbreaks, supporting forward-looking public health strategies. Traditional models such as SIR and agent-based simulations have been foundational in infectious disease epidemiology but often struggle with computational burden, data sparsity, and parameter estimation [17] AI techniques—including ML, deep generative models, and Bayesian inference techniques—have been increasingly adopted to address these limitations [18, 19].
AI models enhance the estimation of key epidemiological parameters such as transmissibility, infection fatality ratios, and generation intervals, even when input data are incomplete or noisy [20] This improvement is made possible by leveraging a range of advanced analytical methodologies.
One foundational statistical framework, increasingly intertwined with AI-driven epidemiological analysis, is Bayesian modeling. While rooted in classical statistics, Bayesian approaches offer a powerful lens for understanding disease dynamics by systematically integrating prior knowledge with observed data, handling uncertainty explicitly, and modeling complex spatial and temporal dependencies. This methodology considers unknown parameters as random variables characterized by probability distributions, incorporating prior information with current data to derive a posterior distribution [21]. Bayesian principles are increasingly integrated directly into AI models, such as generative models [22] and neural networks, [23] to enhance interpretability and provide robust uncertainty quantification for predictions. This approach is instrumental in addressing common challenges in spatial epidemiology, including non-normality, limited sample sizes, missing data, and clustered data structures. In epidemiological modeling and forecasting, these models are applied for tasks such as estimating disease transmission risk, identifying high- incidence areas, assessing influencing factors, enabling real- time disease surveillance, and forecasting outbreaks to guide public health planning and resource allocation [21].
Beyond these established statistical frameworks, specialized deep learning architectures offer new paradigms for understanding disease dynamics. Graph Neural Networks (GNNs), for example, are specifically designed to process and learn from graph-structured data, capturing complex relational information crucial for epidemiological insights. The methodology of GNNs in epidemic modeling involves representing complex relationships and interactions within epidemiological data as graphs, where nodes might represent individuals, locations, or demographic groups, and edges signify connections or interactions relevant to disease spread. GNNs are designed to learn from the structure of these graphs, aggregating information from neighbouring nodes to update the representation of each node, thereby capturing both local and global dependencies within the network. These models can be purely data-driven (Neural Models) or integrate mechanistic epidemiological models (Hybrid Models). In epidemiological modeling and forecasting, GNNs are applied to overcome limitations of traditional models by effectively incorporating relational data, such as human mobility and contact networks. Their applications include disease forecasting, outbreak detection, understanding transmission pathways, and public health surveillance, facilitating the modeling of complex spatio- temporal dependencies that are often challenging for conventional approaches [24].
Complementing models that analyse existing data structures, another class of AI, generative models, offers powerful techniques for creating synthetic data and simulating complex systems, thereby addressing critical gaps in epidemiological modeling and forecasting. Generative models learn the underlying patterns and distributions of input data to produce new, realistic samples that share characteristics with the original data. Key methodologies include Generative Adversarial Networks (GANs), which use a competitive generator-discriminator framework, and Variational Autoencoders (VAEs), which learn probabilistic data representations for decoding new samples. The methodology involves meticulous data collection, model development and training, and critically, integration with classical epidemiological models like SIR and SEIR for a novel, synergistic framework. Rigorous validation is essential to ensure accuracy. In epidemiological modeling and forecasting, generative models revolutionize the field by generating synthetic epidemiological data, addressing issues of data scarcity and privacy. This synthetic data enhances the accuracy and efficiency of predicting disease outbreaks and understanding their complex dynamics, ultimately improving the predictive capabilities of existing epidemiological models and providing more nuanced insights for public health decision-making [25].
Practical applications of AI-based modeling are extensive. BlueDot not only detects outbreaks but also forecasts potential spread by incorporating global travel, weather patterns, and zoonotic spillover data [8]. Similarly, novel algorithms such as Extremal Optimization–tuned Neural Networks (EO-NN), combined with GPS tracking, have been used to identify disease hotspots for Kyasanur Forest Disease (KFD) [3]. AI-based Random Forest models proved effective in forecasting H5N1 outbreaks in Egypt, [26] while SARIMA and SARIMANNAR models have been developed to predict seasonal TB outbreaks and assess TB seasonality in South Africa [27]. Others have predicted novel fungal infection risk factors through ML-based classification [28].
AI’s predictive capabilities extend to scenario modeling and resource planning. Multi-layered perceptron (MLP) and adaptive network–based fuzzy inference systems (ANFIS)
have demonstrated promising results in forecasting infection trends and mortality [29]. These models support healthcare system preparedness by simulating disease burden under varying intervention strategies. In one study, deep reinforcement learning (DRL) was used in Hong Kong to dynamically adjust non-pharmaceutical interventions (NPIs) based on travel, climate, and behavioural data. The system- controlled outbreaks while minimizing health system strain and accelerating herd immunity [30].
As more diverse data streams—including climate, genomic, and behavioural indicators—are integrated, AI has the potential to further improve forecasting accuracy and policy responsiveness.
Diagnostics and Decision Support Systems
AI has revolutionized diagnostics and clinical decision- making in infectious diseases, particularly in resource- limited settings where skilled personnel and laboratory infrastructure are scarce. By integrating medical imaging, electronic health records (EHRs), and clinical data, AI tools improve diagnostic accuracy, reduce diagnostic delays, and enhance infection control at both individual and population levels [3, 31, 32].
Diagnostics and decision support systems significantly leverage AI models that excel at pattern recognition, classification, and multimodal data processing for infectious disease prevention and control.
Among these foundational AI approaches, ML provides a robust, data-driven toolkit to enhance diagnostics and decision support in infectious disease control. These methodologies identify complex patterns from diverse patient data, including symptoms, medical history, imaging results, and demographic information, to improve diagnostic speed, accuracy, and reliability. A variety of ML algorithms are employed, such as Logistic Regression, Support Vector Machines, Naive Bayes, Decision Tree, K-Nearest Neighbour, various forms of Artificial Neural Networks, and powerful ensemble techniques that combine multiple models. These approaches have proven effective in diagnosing infectious conditions, as well as in patient risk assessment and overall health management planning [33].
Within the broader spectrum of ML techniques, Convolutional Neural Networks (CNNs) have demonstrated a transformative impact, particularly within medical image analysis for infectious disease diagnosis. CNNs represent a powerful deep learning methodology adept at image classification by automatically extracting and selecting features, providing an end-to-end solution where features are learned directly from the data through their inherent architecture. This capability makes CNNs highly valuable for medical image classification for disease diagnosis, where their application can accelerate diagnosis and patient referral, leading to earlier treatment and increased cure rates. This robust approach supports clinical decision- making by providing timely and accurate diagnostic insights from medical imaging, thereby contributing to infectious disease prevention and control efforts [34, 35].
For processing textual information, NLP and Large Language Models (LLMs) represent a crucial and evolving subset of AI methodologies designed to understand, interpret, and generate human language text, which is particularly valuable for analysing intricate clinical data. The core methodology involves training models for contextual understanding and human-like text generation, enabling machines to process unstructured textual information. This capability is applied in infectious disease diagnosis and decision support by extracting vital information from diverse textual sources such as medical reports and clinical notes. Applications include enhancing diagnostic accuracy by identifying disease-related patterns from free-text reports, improving public health surveillance through the analysis of large volumes of textual data for early outbreak detection, and supporting risk assessment by extracting crucial clinical data for predictive analytics [36, 37, 38]. These models offer significant potential for streamlining medical tasks and augmenting human expertise in managing infectious diseases.
Complementing these diagnostic models, Federated learning is a decentralized ML methodology that enables the training of algorithms across multiple local data samples without the need for exchanging raw data between servers or edge devices. Unlike conventional centralized methods where all local datasets are transferred to a single server, federated learning allows models to be trained locally using data samples collected at each node. These locally trained models are then synchronized with a master model, often an Artificial Neural Network (ANN), which further globally trains the peer nodes, allowing for continuous refinement of a shared linear model. This approach effectively addresses critical challenges such as data access rights, data privacy, heterogeneous data access, and security, making it particularly beneficial in sensitive domains like healthcare. In the context of infectious disease diagnosis and decision support, federated learning is applied to develop more accurate and reliable distributed ML models for disease detection systems. Training algorithms on diverse, localized datasets without compromising privacy can improve the quality and reliability of disease detection technology, thereby safeguarding human health through more precise and timely predictions derived from improved medical records [39].
Building on these capabilities, AI-powered diagnostics stand out as a prominent application area, spanning medical imaging interpretation, microbial analysis, portable testing, and drug resistance detection—ultimately enhancing timely diagnosis and infection control. One of the most widely applied use cases is AI-powered medical imaging. Deep learning algorithms have been used to interpret chest radiographs for tuberculosis (TB), particularly in regions lacking access to radiologists. These models can triage normal cases efficiently, allowing clinicians to focus on ambiguous or critical findings. Similarly, AI-enhanced microscopy, such as CNNs for Gram stain interpretation, offers high diagnostic precision for bacterial infections and antimicrobial-resistant pathogens [6]. In malaria diagnosis, AI systems analyse blood samples to identify red blood cells infected with Plasmodium species, providing faster and more cost-effective diagnosis in high-burden areas [40]. During the early stages of the COVID-19 pandemic, neural networks were used to analyse chest X-rays, achieving high diagnostic accuracy [41].
In microbiology, population genomics combined with ML models enables the identification of high-risk genotypes, improving the targeting of prevention programs [6]. Tools have also been used to differentiate between bacterial and viral causes of meningitis with high precision [42].
Portable diagnostic tools powered by AI are expanding access to rapid, decentralized testing [43]. Mobile apps and handheld devices can interpret images, symptoms, and even cough audio to diagnose conditions like TB, malaria, or respiratory infections in remote settings [44] These advances reduce dependency on centralized labs and allow for faster case isolation and treatment initiation.
AI has also accelerated drug susceptibility testing and the detection of AMR. Algorithms trained on genomic and phenotypic data can predict resistance patterns and recommend effective therapies, contributing to efforts to combat the global rise of AMR [43]. Integration of these tools into surveillance and hospital systems enhances both individual care and broader infection prevention strategies.
Overall, AI-based diagnostics and decision-support tools contribute to timely disease detection, efficient resource use, and improved infection control, especially in under- resourced settings where traditional diagnostic methods are not always feasible.
Vaccine Development and Delivery
The COVID-19 pandemic underscored the need for rapid vaccine development and global delivery infrastructure. AI has contributed significantly to this effort by accelerating vaccine design, optimizing immunogenic target selection, and improving public health implementation strategies [45]. Using AI, researchers have been able to identify candidate antigens and predict immune responses with greater speed and precision than traditional laboratory methods.
In the early stages of COVID-19 vaccine development, AI-powered reverse vaccinology tools such as Vaxign-ML and MARIA were used to model peptide binding to human leukocyte antigen (HLA) molecules—an essential step in eliciting adaptive immune responses. These tools enabled the rapid identification of viral components like the Spike (S), Nucleocapsid (N), and Membrane (M) proteins, which formed the basis for authorized vaccines including Pfizer/BioNTech’s Comirnaty and Moderna’s mRNA-1273 [46]. Complementing these efforts, DeepMind’s AlphaFold algorithm enabled accurate protein structure prediction, accelerating the design of vaccine candidates by replacing time-consuming traditional methods like X-ray crystallography [8].
AI also supported efforts to improve vaccine inclusivity across populations. Programs like EvalMax and OptiMax, developed at MIT, incorporated genetic diversity in HLA haplotypes to predict how various racial and ethnic groups would respond to specific antigenic peptides. This approach demonstrated that the Spike protein alone might not be immunologically sufficient for all populations, encouraging the inclusion of additional epitopes to strengthen immune responses [46, 47].
Optimizing Response and Resource Allocation
AI plays a pivotal role in optimizing infectious disease response strategies by enabling real-time, systems-level decision support. During public health emergencies, timely decisions about resource allocation, intervention timing, and risk prioritization are critical. AI helps public health authorities synthesize dynamic and high-volume data into actionable strategies, enhancing the speed and precision of outbreak response.
Rather than replacing traditional outbreak tools, AI augments them by integrating multiple data sources— such as mobility patterns, healthcare system capacity, and behavioural indicators—into coordinated frameworks for action.48 These models enable governments to anticipate surges in hospital demand, allocate medical resources efficiently, and adapt interventions in response to rapidly evolving epidemic conditions [49, 50].
For example, AI has supported adaptive NPI planning by continuously analysing real-time data to adjust control measures without exceeding healthcare system capacity [30] Similarly, AI-based models significantly enhance vaccination strategies by enabling precise targeting, adaptive planning, and efficient resource use [45].
As public health systems face increasingly complex and globalized threats, AI’s capacity to support proactive, scalable, and adaptive response strategies will be essential to improving the resilience and equity of infectious disease control efforts.
Enhancing Public Health Communication
Accurate public communication is vital in infectious disease control, particularly during pandemics when fear and misinformation can undermine health interventions. AI has proven effective in mitigating these risks by monitoring digital platforms and enabling real-time, targeted communication.
AI tools using NLP have been deployed to analyse online content from platforms such as Twitter and Reddit. These systems can detect misinformation trends, analyse sentiment shifts, and help authorities intervene with accurate messaging [8]. For example, NLP-based sentiment analysis has been used to analyse vaccine hesitancy during COVID-19 [51, 52]. Another application was the WHO’s AI-powered chatbot, which provided timely, verified information to global users during the pandemic. It served as a trusted communication channel, reducing anxiety and countering misinformation at scale [53]. Beyond information dissemination, these tools reinforce behavioural epidemiology by informing risk communication strategies. Monitoring digital concerns allows for responsive public health messaging, increasing compliance with control measures, and strengthening epidemic response [54].
Future Prospects of AI in Infectious Disease Prevention and Control
AI is poised to revolutionize global infectious disease prevention and control, offering unprecedented capabilities to enhance public health responses by improving their scalability, timeliness, and precision [43].
One of the most significant advancements lies in the multi- modal data integration into global real-time surveillance networks. Future AI systems are projected to seamlessly integrate diverse data sources, including genomic sequences, behavioural trends, mobility patterns, and environmental indicators [55]. For example, Boston University’s BEACON platform is an open-source AI-powered surveillance system that integrates data from multiple disease-tracking sources, uses AI to analyse and translate information, and produces human-verified reports—supporting real-time, multi-modal global disease monitoring and information sharing [56]. The US Centres for Disease Control and Prevention is already leveraging AI and ML within its Data Modernization Initiative to incorporate non-traditional data sources such as images, audio, social media, and EHRs to improve surveillance speed and accuracy, accelerate outbreak response, and enhance vaccine safety monitoring [57]. Research projects, like the NIH-funded VentNet, demonstrate ongoing efforts in multi- modal data integration for clinical decision support, using ML on EHR data and planning to incorporate imaging to predict outcomes like respiratory failure in COVID-19 patients [58].
Generative AI is emerging as a critical tool, particularly in accelerating therapeutic discovery, vaccine development, and drug design. These models, alongside sequence-to- structure prediction and GNNs, are expanding the landscape of innovation [59]. Companies like Evaxion are actively using AI to simulate the immune system and create predictive models to identify novel targets for vaccines [60]. These AI innovations enable rapid and efficient screening of vast numbers of molecules, significantly reducing the time and cost associated with developing new pharmaceutical compounds and vaccine candidates [61].
Furthermore, AI-driven behavioural modeling is anticipated to become more sophisticated, allowing public health officials to better anticipate public responses to containment measures and understand factors influencing vaccine uptake [54]. Cutting-edge research utilizes generative multi-agent systems, powered by LLMs, to simulate complex human behaviours, including vaccine hesitancy dynamics and adherence to non-pharmaceutical interventions during public health emergencies [62]. These simulations can provide valuable insights for informing public health policy.AI-powered tools are also expected to advance health equity, particularly in low- and middle-income countries (LMICs). Cloud-based diagnostics, mobile health apps, and remote monitoring platforms will allow for early detection, risk assessment, and disease management even in settings with limited infrastructure. The expansion of wearables and telemedicine will further improve health outcomes and service delivery in remote settings [43]. These tools can be used for diagnosis, morbidity or mortality risk assessment, disease outbreaks and surveillance, and health policy and planning [63].
The collective application of these AI innovations promises to usher in an era of more proactive, precise, and equitable public health responses, capable of tackling the evolving challenges posed by infectious diseases globally.
Challenges
Data Quality, Representativeness, and Algorithmic Bias
The utility of AI in infectious disease prevention and control is fundamentally dependent on the quality, diversity, and representativeness of the data used to train its models. In many LMICs, the scarcity of high-quality, standardized, and interoperable datasets presents a critical barrier. Incomplete, inconsistent, or outdated data can result in unreliable AI predictions, thereby compromising timely and effective responses to disease outbreaks [3, 43].
A central concern is algorithmic bias arising from unrepresentative training data. Many AI systems are developed using datasets predominantly from high-income countries (HICs), limiting their generalizability to LMICs and underrepresented populations [43]. Such bias can lead to distorted epidemiologic predictions and exacerbate existing health disparities. For instance, U.S. COVID-19 mortality data have been shown to underreport deaths among Black and Hispanic populations by up to 60% due to missing race information—an issue both moral and methodological [64]. Moreover, structural bias in data collection can cause AI models to reach accurate-seeming but misleading conclusions. One striking example involved image-classification models trained to detect COVID-19 using chest radiographs. When children’s chest X-rays were used as a control group, the models effectively distinguished adults from children, rather than identifying infection status. In fact, prediction remained possible even after lung areas were removed from images, simply based on the dataset source. This suggests that the standard testing protocols used in many studies on automated COVID-19 diagnosis may be biased, leading models to learn dataset-specific features rather than medically relevant information [65].
In vaccine development, biases in healthcare access and reporting further contribute to unequal performance and safety across populations. When AI models are trained on data primarily from HICs, resulting vaccines may be less effective or safe in LMICs, exacerbating global inequities and hindering broad-based immunization success [8].
Data Governance, Privacy, and Security
Beyond the quality and representativeness of data, how this information is governed, protected, and who has access to it poses another significant set of challenges. The integration of AI into infectious disease surveillance has amplified long-standing concerns around data governance, individual privacy, and security. AI systems frequently rely on sensitive health information—including personal medical records and genomic data—to model disease risks and inform interventions [8]. As surveillance networks expand, so do the risks associate with breaches and unauthorized access to personal data [3].
These concerns are compounded by the use of increasingly granular and unconventional data sources. AI models now incorporate digital traces from wearable devices, connected health apps, and “digital exhaust” generated by users interacting with online platforms [66]. While these inputs enhance model accuracy, they also raise the risk of re-identification, especially when datasets are combined across systems or inadequately anonymized. The scale and intrusiveness of such data collection challenge existing norms of consent and confidentiality in public health [67].
New computational approaches, such as federated learning, have been explored to mitigate privacy risks in AI- powered surveillance. In this framework, analytical models are deployed to individual devices where data remains locally stored. Aggregated insights are then returned to a central system without transferring the underlying personal data. A recent study used federated learning in smartphone- based infectious disease surveillance, illustrating a method that reduces central data storage risks while maintaining analytical capability [7].
Despite such technical developments, public unease about the potential misuse of health data remains high. The challenge of balancing public health objectives with personal data protection is further complicated by the need for large, open datasets to advance epidemiologic modeling and prediction. In the absence of clear regulatory boundaries, privacy risks can undermine trust and hinder participation in AI-driven disease surveillance.
Technical Barriers and Model Limitations
Even with well-governed and high-quality data, the inherent characteristics and current limitations of AI models themselves present distinct technical hurdles. One of AI’s most persistent technical limitations in infectious disease prevention and control is the risk of overfitting. Overfitting occurs when a model learns not only the underlying patterns in the training data but also the noise, resulting in high apparent accuracy during training but poor generalization to new, unseen data [3, 55].
This problem is especially acute when models are trained on small or biased datasets—common in early-stage outbreaks or low-resource settings—leading to predictions that cannot adapt to evolving epidemiological conditions [7].
This challenge is compounded by the “black box” nature of many deep learning models. These systems often lack transparency in their internal decision-making, making it difficult for users to interpret or validate predictions [68] In public health contexts where decisions must be accountable and evidence-based, this lack of explainability undermines trust and may limit adoption by clinicians, epidemiologists, or policymakers.
Another concern is the potential for deep learning algorithms to amplify existing biases. When models are trained on datasets that reflect historical or structural inequities, such as underrepresentation of certain populations or regional disparities, they may reproduce or even intensify these patterns in their predictions [69]. In infectious disease contexts, such skewed outputs could affect disease burden estimates, resource allocation, or even diagnosis rates across different communities.
Finally, most general-purpose AI models, such as those designed for open-ended text or speech tasks, are not currently equipped to handle specialized epidemiological questions or concepts. Integrating single-task models into more general frameworks remains a future goal rather than a present reality. Furthermore, these foundation models are typically developed by large technology firms at high cost, making downstream fine-tuning for public health applications both unsustainable and inequitable [20].
Transparency, Explainability, and Public Trust
The opacity of many AI models presents a major barrier to their integration into infectious disease prevention and control systems. Often referred to as “black-box” algorithms, these models—especially deep learning systems—lack transparency in how they process inputs and generate outputs. This can erode clinical trust and make it difficult for public health professionals to interpret, validate, or act on AI-generated predictions [43, 55]. Without sufficient clarity on decision-making pathways, AI systems may fail to gain traction in real-world public health workflows.
This challenge is particularly acute in clinical settings, where practitioners are trained to rely on empirical evidence and observable reasoning. AI outputs that lack interpretability may be dismissed or underutilized, even if technically accurate. In epidemic modeling, the problem extends further: many current AI-based models struggle to offer mechanistic insights into transmission dynamics or disease behaviour. As a result, their generalizability across populations, pathogens, or geographies remains limited [20].
To address these issues, researchers have developed approaches known as explainable AI (XAI), which aim to clarify the rationale behind AI decisions [70]. However, XAI is not a complete solution. One persistent risk is “false confirmation,” when both humans and AI agree on an incorrect decision [2].
Beyond clinical and scientific use, AI’s opacity also complicates its acceptance in the public domain. Traditionally, public health decisions have been communicated by trusted figures such as epidemiologists or health officials, relying on a blend of data, expertise, and human judgment. The introduction of AI as a decision-making agent introduces an unfamiliar, abstract actor into this space-one that the public may not intuitively trust [71].
Public skepticism can be exacerbated when AI-driven guidance conflicts with traditional expert consensus or produces recommendations that appear counterintuitive. Moreover, inconsistent media narratives—ranging from exaggerated optimism to alarmist warnings-further distort perceptions of AI’s capabilities and limitations. In the context of infectious disease forecasting, either a hyped success or a publicized failure may have lasting impacts on public confidence. These dynamics present an enduring challenge to the legitimate integration of AI into population-level health decision-making processes [55].
Ethical Dilemmas and Health Equity
The application of AI in infectious disease prevention and control raises substantial ethical challenges. Chief among these are concerns regarding patient privacy, algorithmic bias, data integrity, equity in healthcare access, and the autonomy of both patients and healthcare providers. These challenges are especially pronounced when AI is used in diagnosis or prognosis, where automated outputs may directly influence clinical decisions and population-level interventions [43].
AI systems trained on non-representative datasets may perpetuate or exacerbate existing health disparities, resulting in unequal availability of care or reduced model accuracy for underrepresented populations [72]. For example, AI models trained on historical data may perpetuate health care disparities by reinforcing biases against protected populations, highlighting the need for AI systems to be designed and evaluated with principles of distributive justice to ensure equitable outcomes [73]. These challenges highlight the importance of transparency and accountability in the ethical deployment of AI in healthcare.
Various ethical frameworks have been proposed to guide the responsible development and deployment of AI in public health. For instance, the WHO’s 2021 guidance outlines six consensus principles: protecting autonomy; promoting human well-being, human safety, and the public interest; ensuring transparency, explainability, and intelligibility; fostering responsibility and accountability; ensuring inclusiveness and equity; and promoting AI that is responsive and sustainable [1]. Ethical codes have also been proposed by regional and global actors such as the Council of Europe and Gavi, reflecting a growing awareness of the moral complexity involved in deploying AI at scale [2].
Misinformation and Disinformation
The societal impact of AI also extends to the information ecosystem, where its capabilities can unfortunately be harnessed to spread harmful narratives. The rapid spread of misinformation facilitated by AI has posed another critical challenge during health emergencies. AI-powered content recommendation systems and social media algorithms have accelerated the circulation of false or misleading information, especially during the COVID-19 pandemic. One large-scale study analysed 80 million posts from nearly 77,000 Twitter (now X) users over 18 months and found that those who spread COVID-19 misinformation exhibited nearly twice the level of anxiety compared to other users [74]. This dynamic not only distorted public understanding of the outbreak but also imposed measurable psychological harm, underscoring the broader societal costs of AI-amplified misinformation [8].
Regulatory Gaps and lack of standardization
Navigating these complex ethical and societal challenges, from ensuring data integrity to combating misinformation, necessitates robust governance frameworks; however, the rapid pace of AI development has far outstripped the capacity of most regulatory frameworks to ensure safe and responsible implementation. In the domain of infectious disease prevention and control, this regulatory lag presents major obstacles to the safe deployment of AI systems. AI algorithms used for diagnosis or surveillance may lack clearly defined pathways for clinical validation, post- market surveillance, or liability assignment, particularly in countries with an underdeveloped legal infrastructure [75, 76]. Ambiguities in accountability for AI-generated recommendations further complicate efforts to ensure transparency and legal compliance in public health settings [77].
Recognizing these limitations, global bodies such as the WHO have begun issuing high-level guidance. The WHO “Regulatory considerations on artificial intelligence for health” emphasizes the importance of pre-market validation, continuous documentation, risk monitoring, and stakeholder engagement to ensure transparency and traceability [78]. However, national-level regulatory structures remain fragmented, leading to inconsistent compliance standards and gaps in oversight.
Regulatory challenges are compounded by the inherently cross-border nature of disease outbreaks. AI systems used for global health surveillance require coordination across jurisdictions with differing laws, capabilities, and ethical norms. The COVID-19 pandemic demonstrated that, despite rapid technical advances, a lack of harmonized regulatory cooperation can undermine the utility of AI-powered surveillance tools. Without mechanisms for international coordination, the deployment of AI in epidemic response may be hindered, regardless of technical readiness [7].
Infrastructure, Cost, and Workforce Limitations
Beyond the need for clear rules and ethical guidelines, infrastructure gaps present one of the most significant barriers to the integration of AI in infectious disease prevention and control, particularly in LMICs. In many of these settings, healthcare facilities lack the foundational digital infrastructure, such as EHRs, diagnostic equipment, and functional internet connectivity, required to implement AI systems [79]. These limitations are compounded by unreliable electricity supply, which directly affects the continuous operation of AI-powered tools [43].
Even in HICs, the integration of AI tools into healthcare environments is challenged by the incompatibility of legacy systems. Many hospital management platforms, public health databases, and electronic medical records were built decades ago and were not designed to accommodate the high-volume, dynamic, and real-time nature of AI algorithms. Contemporary AI models often rely on specialized computational environments, deep learning libraries, and data formats that are difficult to align with existing software and infrastructure. This incompatibility can pose a substantial risk of operational disruption and data loss during attempted integration [55].
The cost of adopting AI technologies also poses a formidable obstacle. Beyond the initial investment in hardware and software, AI deployment requires ongoing expenditures for maintenance, system upgrades, and secure data storage [80]. The collection and curation of high-quality, large- scale datasets—essential for AI performance—also incur considerable costs, as do the implementation of data privacy safeguards [81]. These financial burdens can be prohibitive, especially in resource-constrained health systems.
Equally critical is the issue of workforce preparedness. Successful AI implementation depends on a health workforce that is literate in data science and AI systems. However, there is a notable shortage of healthcare professionals with such expertise, particularly in low-resource settings. This gap is further widened by the migration of skilled workers to more developed health systems, which reduces local capacity for AI-enabled healthcare delivery. In addition, existing staff may resist the adoption of AI technologies due to unfamiliarity or perceived threats to professional autonomy [43, 82].
Together, these infrastructure and workforce limitations highlight the practical barriers that must be addressed before AI can be reliably and equitably integrated into infectious disease surveillance and control.
System Fragmentation and Interdisciplinary Collaboration Gaps
Finally, even when resources and expertise are available, the effective integration of AI into infectious disease prevention and control is often hindered by the structure of health systems, the organization of data, and the interplay between different disciplines. One of the major challenges is the fragmented nature of health data infrastructure. Health- related data are dispersed across hospitals, community clinics, and individual devices such as smartphones and wearables. Even within single institutions, departments often rely on custom-built systems provided by different vendors, resulting in incompatible data formats and restricted interoperability [83]. As a result, AI models may be limited to operating within narrow data domains, undermining their ability to provide comprehensive and generalizable insights across diverse patient populations.
The problem of data silos not only limits model scope but also affects training quality and representativeness. A lack of integrated datasets prevents AI systems from capturing the full range of patient variability, particularly among populations underrepresented in discrete data systems. This fragmentation impedes the development of contextually relevant AI models that can consistently perform across varied clinical and demographic cohorts [84].
Despite the promise of AI in healthcare, many research publications remain focused on isolated technical innovations rather than interdisciplinary applications. Most AI development does not span the continuum of clinical care, infection prevention and control, or broader public health systems, this highlights the need for interdisciplinary integration and collaboration [85].
Effective integration of AI into public health also requires closer collaboration between data scientists and domain experts. When AI predictions are presented in isolation, they may lack the contextual grounding needed for interpretation. In contrast, when AI-generated outputs are jointly evaluated with input from epidemiologists and public health professionals, they gain both interpretability and relevance [55].
Policy and Practice Recommendations
Realizing the transformative potential of AI in infectious disease prevention and control will require coordinated policy efforts, ethical safeguards, and global collaboration. Stakeholders—including governments, healthcare providers, technologists, and public health agencies—need to work together to create a policy environment that ensures equitable, transparent, and responsible AI deployment across diverse epidemiological contexts [43].
A priority area involves investing in high-quality, representative, and interoperable digital infrastructure. Governments and institutions are encouraged to support open data systems for infectious disease surveillance that enable secure, ethical, and privacy-preserving data sharing [86]. Approaches such as federated learning and adherence to the FAIR data principles (Findability, Accessibility, Interoperability, Reusability)[87] may provide viable pathways to cross-border collaboration while protecting individual privacy.
To build public trust and ensure accountability, regulatory frameworks ought to evolve in step with technological advancements. These frameworks could incorporate lifecycle monitoring, risk mitigation strategies, and documentation processes, as emphasized by the WHO and other regulatory bodies [78]. Ethical oversight mechanisms—such as diverse, interdisciplinary ethics committees—can help ensure that AI systems are reviewed across the development pipeline, upholding principles like privacy by design, data minimization, and meaningful consent. Furthermore, public engagement and consultation may enrich the governance of AI by aligning implementation with societal values and expectations [55].
From a technical perspective, model development should balance innovation with interpretability and performance in real-world settings. Hybrid approaches that integrate deep learning with more traditional statistical methods can offer advantages in terms of both accuracy and explainability [55]. It is advisable to evaluate AI models not only on predictive performance but also on calibration, causal interpretability, and implementation feasibility [20]. Transparency in model architecture, training data, and assumptions—facilitated through open-source tools and public review—can further support responsible use.
Equity considerations are paramount. Many LMICs face challenges in accessing the infrastructure, expertise, and financial resources needed for AI development and deployment. Promoting open-source AI tools, equitable data- sharing arrangements, and inclusive global collaborations could help address these disparities [43]. AI tools in LMICs often underperform when trained on data from HICs and not adapted to local contexts. To improve equity, AI development should incorporate local data, engage LMIC stakeholders, and evaluate effectiveness in real-world settings [88, 89].
Ultimately, maximizing the public health benefits of AI in infectious disease control requires an integrated strategy that promotes innovation while upholding ethical standards and global equity. By embracing inclusive, adaptive, and collaborative approaches, stakeholders can better harness AI’s potential to improve outbreak preparedness, strengthen diagnostics, and advance global health security Figure 1.
Conclusion
AI is poised to become a cornerstone of infectious disease prevention and control. From enhancing surveillance systems and accelerating outbreak detection to supporting diagnostics and optimizing vaccine delivery, AI has demonstrated significant promise in transforming global public health strategies. The COVID-19 pandemic has underscored both the urgency and the potential of AI-driven tools to address infectious disease threats more rapidly and equitably than ever before.
Yet, the path forward is complex. The effective application of AI requires overcoming substantial challenges—particularly in ensuring data quality, managing algorithmic bias, addressing ethical concerns, and closing the digital infrastructure gap in low-resource settings. Fragmented data systems, limited interoperability, and a lack of interdisciplinary collaboration continue to hinder the full integration of AI into public health ecosystems.
Crucially, AI must not reinforce existing inequities or function as a “black box” devoid of accountability. Building trust through transparency, ensuring explainability, and promoting public engagement are essential for AI adoption in both clinical and community settings. Likewise, regulatory frameworks must evolve to ensure safety, effectiveness, and fairness while enabling innovation.
Going forward, inclusive global collaboration and deliberate policy action will be key to ensuring that AI technologies are not only technically sound but also socially and ethically aligned with the goals of public health. When developed and implemented responsibly, AI can empower health systems worldwide to detect, respond to, and prevent infectious diseases with unprecedented speed, precision, and equity.
Contributors
JL conceptualized and supervised the study. SW conducted the literature search, designed the review structure, synthesized the evidence, and drafted the manuscript. SW and JL did critical reading and revised the manuscript. All authors approved the final version and take responsibility for the decision to submit for publication.
Declaration of interests
The authors declare no conflict of interest.
Data sharing statement
No datasets were generated or analysed during the
current study.
Acknowledgements
This research was supported by the National Natural Science Foundation of China (72122001).
References
-
WHO (2021) Ethics and Governance of Artificial Intelligence for Health: WHO Guidance. World Health Organization, Switzerland.
-
Panteli D, Adib K, Buttigieg S (2025) Artificial intelligence in public health: Promises, challenges, and an agenda for policy makers and public health institutions. Lancet Public Health 10(5): e428-e432.
-
Srivastava V, Kumar R, Wani MY, Robinson K, Ahmad A (2025) Role of artificial intelligence in early diagnosis and treatment of infectious diseases. Infect Dis Lond Engl 57(1): 1-26.
-
Salam MA, Al-Amin MY, Salam MT (2023) Antimicrobial resistance: A growing serious threat for global public health. Healthcare 11(13): 1946.
-
Findlater A, Bogoch II (2018) Human mobility and the global spread of infectious diseases: A focus on air travel. Trends Parasitol 34(9): 772-783.
-
Fitzpatrick F, Doherty A, Lacey G (2020) Using artificial intelligence in infection prevention. Current Treatment Options Infectious Diseases 12: 135-144.
-
Brownstein JS, Rader B, Astley CM, Tian H (2023) Advances in artificial intelligence for infectious-disease surveillance. N Engl J Med 388(17): 1597-1607.
-
Yang L, Lu S, Zhou L (2024) The implications of artificial intelligence on infection prevention and control: Current progress and future perspectives. China CDC Wkly 6(35): 901.
-
Gadaleta M, Radin JM, Baca-Motes K (2021) Passive detection of COVID-19 with wearable sensors and explainable machine learning algorithms. Npj Digit Med 4(1): 166.
-
Aiello AE, Renson A, Zivich P (2020) Social media- and internet-based disease surveillance for public health. Annu Rev Public Health 41: 101.
-
Cartaxo ANS, Barbosa FIC, Bermejo PH de S, Moreira MF, Prata DN (2021) The exposure risk to COVID-19 in most affected countries: A vulnerability assessment model. PLoS ONE 16(3): e0248075.
-
Malik YS, Sircar S, Bhat S, Ansari MI, Pande T, et al. (2021) How artificial intelligence may help the COVID-19 pandemic: Pitfalls and lessons for the future. Rev Med Virol 31(5): 1-11.
-
Rao ASRS, Vazquez JA (2020) Identification of COVID-19 can be quicker through artificial intelligence framework using a mobile phone–based survey when cities and towns are under quarantine. Infect Control Hosp Epidemiol 41(7): 826-830.
-
Sardar AW, Ullah F, Bacha J, Khan J, Ali F, et al. (2022) Mobile sensors-based platform of Human Physical Activities Recognition for COVID-19 spread minimization. Comput Biol Med 146: 105662.
-
Nguyen KA, Luo Z, Watkins C (2020) Epidemic contact tracing with smartphone sensors. J Locat Based Serv 14(2): 92-128.
-
Hang CN, Tsai YZ, Yu PD, Chen J, Tan CW (2023) Privacy- enhancing digital contact tracing with machine learning for pandemic response: A comprehensive review. Big Data Cogn Comput 7(2): 108.
-
Hunter E, Mac Namee B, Kelleher JD (2017) A taxonomy for agent-based models in human infectious disease epidemiology. J Artif Soc Simul 20(3).
-
Tran T, Pham T, Carneiro G, Palmer L, Reid I (2017) A Bayesian data augmentation approach for learning deep models. In: Advances in Neural Information Processing Systems 30.
-
Mishra S, Flaxman S, Berah T, Zhu H, Pakkanen M, et al. (2022) πVAE: A stochastic process prior for Bayesian deep learning with MCMC. Stat Comput 32(6): 96.
-
Kraemer MUG, Tsui JLH, Chang SY, Lytras S, Khurana MP, et al. (2025) Artificial intelligence for modelling infectious disease epidemics. Nature 638(8051): 623-635.
-
Wang Y, Chen X, Xue F (2024) A review of bayesian spatiotemporal models in spatial epidemiology. ISPRS Int J Geo-Inf1 3(3): 97
-
Biazzo I, Braunstein A, DallAsta L, Mazza F (2022) A bayesian generative neural network framework for epidemic inference problems. Sci Rep 12(1): 19673.
-
Radev ST, Graw F, Chen S, Mutters NT, Eichel VM, et al. (2021) OutbreakFlow: Model-based bayesian inference of disease outbreak dynamics with invertible neural networks and its application to the COVID-19 pandemics in germany. PLoS Comput Biol 17(10): e1009472.
-
Liu Z, Wan G, Prakash BA, Lau MSY, Jin W (2024) A review of graph neural networks in epidemic modeling. In: Proceedings of the 30th ACM SIGKDD Conference on Knowledge Discovery and Data Mining. KDD ’24 Association for Computing Machinery 6577-6587.
-
Balaram VVSSS, Salman M (2024) Generative AI and its potential to revolutionize epidemiological modeling and disease prediction. Int J Sci Innov Eng 1(2): 29-36.
-
Kane MJ, Price N, Scotch M, Rabinowitz P (2014) Comparison of ARIMA and random forest time series models for prediction of avian influenza H5N1 outbreaks. BMC Bioinformatics 15(1): 276.
-
Azeez A, Obaromi D, Odeyemi A, Ndege J, Muntabayi R (2016) Seasonality and trend forecasting of tuberculosis prevalence data in Eastern Cape, South Africa, using a hybrid model. Int J Environ Res Public Health 13(8): 757.
-
Mayer LM, Strich JR, Kadri SS, Lionakis MS, Evans NG, et al. (2022) Machine learning in infectious disease for risk factor identification and hypothesis generation: Proof of concept using invasive candidiasis. Open Forum Infect Dis 9(8): ofac401.
-
Pinter G, Felde I, Mosavi A, Ghamisi P, Gloaguen R (2020) COVID-19 pandemic prediction for Hungary; A hybrid machine learning approach. Mathematics 8(6): 890.
-
Yao Y, Zhou H, Cao Z, Zeng DD, Zhang Q (2023) Optimal adaptive nonpharmaceutical interventions to mitigate the outbreak of respiratory infections following the COVID-19 pandemic: A deep reinforcement learning study in Hong Kong, China. J Am Med Inform Assoc JAMIA 30(9): 1543-1551.
-
Ye J, Woods D, Jordan N, Starren J (2024) The role of artificial intelligence for the application of integrating electronic health records and patient-generated data in clinical decision support. AMIA Summits Transl Sci Proc 2024: 459-467.
-
Lee S, Kim HS (2021) Prospect of artificial intelligence based on electronic medical record. J Lipid Atheroscler 10(3): 282-290.
-
Mishra S, Kumar R, Tiwari SK, Ranjan P (2022) Machine learning approaches in the diagnosis of infectious diseases: A review. Bull Electr Eng Inform 11(6): 3509- 3520.
-
Yadav SS, Jadhav SM (2019) Deep convolutional neural network based medical image classification for disease diagnosis. J Big Data 6(1): 113.
-
Wicaksono DF, Basuki RS, Setiawan D (2024) Peningkatan performa model machine learning XGBoost classifier melalui teknik oversampling dalam prediksi penyakit AIDS. J MEDIA Inform BUDIDARMA 8(2): 736-747.
-
Omar M, Brin D, Glicksberg B, Klang E (2024) Utilizing natural language processing and large language models in the diagnosis and prediction of infectious diseases: A systematic review. Am J Infect Control 52(9): 992-1001.
-
Boligarla S, Laison EKE, Li J, Mahadevan R, Austen Ng, et al. (2023) Leveraging machine learning approaches for predicting potential lyme disease cases and incidence rates in the united states using twitter. BMC Med Inform Decis Mak 23(1): 217.
-
Cury RC, Megyeri I, Lindsey T, Macedo R, Batlle J, et al. (2021) Natural language processing and machine learning for detection of respiratory illness by chest CT imaging and tracking of COVID-19 pandemic in the US. Radiol Cardiothorac Imaging 3(1): e200596.
-
Javed I, Iqbal U, Bilal M, Shahzad B, Chung TS, et al. (2023) Next generation infectious diseases monitoring gages via incremental federated learning: Current trends and future possibilities. Comput Intell Neurosci 2023(1): 1102715.
-
Manning K, Zhai X, Yu W (2022) Image analysis and machine learning-based malaria assessment system. Digit Commun Netw 8(2): 132-142.
-
Akter S, Shamrat FM, Chakraborty S, Karim A, Azam S (2021) COVID-19 detection using deep learning algorithm on chest X-ray images. Biology 10(11): 1174.
-
Angelo G, Pilla R, Tascini C, Rampone S (2019) A proposal for distinguishing between bacterial and viral meningitis using genetic programming and decision trees. Soft Comput 23(22): 11775-11791.
-
Hudu SA, Alshrari AS, Shoura EJI, Osman A, Jimoh AO (2025) A critical review of the prospect of integrating artificial intelligence in infectious disease diagnosis and prognosis. Interdiscip Perspect Infect Dis 2025(1): 6816002.
-
Vitazkova D, Foltan E, Kosnacova H, M Micjan, M Donoval, et al. (2024) Advances in respiratory monitoring: A comprehensive review of wearable and remote technologies. Biosensors 14(2): 90.
-
Asediya VS, Anjaria PA, Mathakiya RA, Koringa PG, Nayak JB, et al. (2024) Vaccine development using artificial intelligence and machine learning: A review. Int J Biol Macromol 282: 136643.
-
Arora G, Joshi J, Mandal RS, Shrivastava N, Virmani R, et al. (2021) Artificial intelligence in surveillance, diagnosis, drug discovery and vaccine development against COVID-19. Pathogens 10(8): 1048.
-
Liu G, Carter B, Bricken T, S Jain, M Viard, et al. (2020) Computationally optimized SARS-CoV-2 MHC class I and II vaccine formulations predicted to target human haplotype distributions. Cell Syst 11(2): 131-144.
-
Syrowatka A, Kuznetsova M, Alsubai A, AL Beckman, PA Bain, et al. (2021) Leveraging artificial intelligence for pandemic preparedness and response: A scoping review to identify key use cases. Npj Digit Med 4(1):1-14.
-
McKee M, Rosenbacke R, Stuckler D (2025) The power of artificial intelligence for managing pandemics: A primer for public health professionals. Int J Health Plann Manage 40(1): 257-270.
-
Isiaka AB, Anakwenze VN, Ilodinso CR, Ezeokoli MV, Noi SM, et al. (2024) Harnessing artificial intelligence for early detection and management of infectious disease outbreaks. Int J Innov Res Dev.
-
Xu H, Liu R, Luo Z, Xu M (2022) COVID-19 vaccine sensing: Sentiment analysis and subject distillation from Twitter data. Telemat Inform Rep 8: 100016.
-
Qorib M, Oladunni T, Denis M, Ososanya E, Cotae P (2023) COVID-19 vaccine hesitancy: Text mining, sentiment analysis and machine learning on COVID-19 vaccination Twitter dataset. Expert Syst Appl. 212: 118715.
-
(2025) WHO and Rakuten Viber fight COVID-19 misinformation with interactive chatbot.
-
Ali H (2024) AI for pandemic preparedness and infectious disease surveillance: Predicting outbreaks, modeling transmission, and optimizing public health interventions. Int J Res Publ Rev 05: 4605-4619.
-
Zhao AP, Li S, Cao Z, Hu PJ, Wang J, et al. (2024) AI for science: Predicting infectious diseases. J Saf Sci Resil. 5(2): 130-146.
-
(2025) BU launches an open-source infectious diseases monitoring tool powered by AI and human experts. Boston University.
-
(2025) Centres for Disease Control and Prevention. Artificial Intelligence and Machine Learning: Applying Advanced Tools for Public Health U.S.
-
(2025) VentNet: A Real-Time Multimodal Data Integration Model for Prediction of Respiratory Failure in Patients with COVID-19.
-
Wong F, de la Fuente-Nunez C, Collins JJ (2023) Leveraging artificial intelligence in the fight against infectious diseases. Science 381(6654): 164-170.
-
(2025) Using AI to create a vaccine revolution.
-
Kandhare P, Kurlekar M, Deshpande T, Pawar A (2025) A review on revolutionizing healthcare technologies with AI and ML applications in pharmaceutical sciences. Drugs Drug Candidates 4(1): 9.
-
Hou AB, Du H, Wang Y, Jingyu Z, Zixiao W, et al. (2025) Can a society of generative agents simulate human behaviour and inform public health policy? A case study on vaccine hesitancy. Published online arXiv: 2503.09639.
-
Schwalbe N, Wahl B (2020) Artificial intelligence and the future of global health. Lancet Lond Engl 395(10236): 1579-1586.
-
Labgold K, Hamid S, Shah S, Gandhi NR, Chamberlain A, et al. (2021) Estimating the unknown: Greater racial and ethnic disparities in COVID-19 burden after accounting for missing race/ethnicity data. Epidemiol Camb Mass 32(2):157-161.
-
Maguolo G, Nanni L (2021) A critic evaluation of methods for COVID-19 automatic detection from X-ray images. Int J Inf Fusion 76: 1-7.
-
Shajari S, Kuruvinashetti K, Komeili A, Sundararaj U (2023) The emergence of AI-based wearable sensors for digital health technology: A review. Sensors 23(2023): 9498.
-
Emam KE, Jonker E, Arbuckle L, Malin B (2011) A systematic review of re-identification attacks on health data. PLoS ONE 10(4): e0126772.
-
von Eschenbach WJ (2021) Transparency and the black box problem: Why we do not trust AI. Philos Technol 34(4): 1607-1622.
-
Du M, Yang F, Zou N, Hu X (2021) Fairness in deep learning: A computational perspective. IEEE Intell Syst 36(4):25-34.
-
Shin D (2021) The effects of explainability and causability on perception, trust, and acceptance: Implications for explainable. Int J Hum-Comput Stud 146: 102551.
-
Gao S, He L, Chen Y, Li D, Lai K (2020) Public perception of artificial intelligence in medical care: Content analysis of social media. J Med Internet Res 22(7): e16649.
-
Gao Y, Sharma T, Cui Y (2023) Addressing the challenge of biomedical data inequality: An artificial intelligence perspective. Annu Rev Biomed Data Sci. Published online 6(1): 153-171.
-
Rajkomar A, Hardt M, Howell M, Corrado GS, Chin M (2018) Ensuring fairness in machine learning to advance health equity. Ann Intern Med 169: 866-872.
-
Verma G, Bhardwaj A, Aledavood T, De Choudhury M, Kumar S (2022) Examining the impact of sharing COVID-19 misinformation online on mental health. Sci Rep 12(1): 8045.
-
Barbati C, Viviani L, Vecchio R, Arzilli G, Angelis lD, et al. (2024) Impact of artificial intelligence on healthcare- associated infection control: A systematic review. Eur J Public Health 34: 144-507.
-
Cestonaro C, Delicati A, Marcante B, Caenazzo L, Tozzo P (2023) Defining medical liability when artificial intelligence is applied on diagnostic algorithms: A systematic review. Front Med 10: 1305756.
-
Branda F, Stella M, Ceccarelli C, Cabitza F, Ceccarelli Get, al. (2025)The role of AI-based chatbots in public health emergencies: A narrative review. Future Internet 17(4): 145.
-
World Health Organization (2023) Regulatory considerations on artificial intelligence for health. World Health Organization.
-
Khan MS, Umer H, Faruqe F (2024) Artificial intelligence for low income countries. Humanit Soc Sci Commun 11(1):1-13.
-
Fortuna C, Yetgin H, Mohorcic M (2023) Smart infrastructures: Artificial intelligence-enabled lifecycle automation. IEEE Ind Electron Mag 17(2): 37-47.
-
Herath HM, Herath K, Madhusanka A, Guruge L (2024) Data protection challenges in the processing of sensitive data. Data Protection 155-179.
-
Malerbi F, Nakayama L, Dychiao RG, Lucas ZR; Cleva V, et al. (2023) Digital education for the deployment of artificial intelligence in health care. J Med Internet Res 25.
-
Panch T, Mattie H, Celi LA (2019) The “inconvenient truth” about AI in healthcare. Npj Digit Med 2(1): 1-3.
-
Finlayson SG, Subbaswamy A, Singh K, John B, Annabel K, et al. (2021) The clinician and dataset shift in artificial intelligence. N Engl J Med 385(3): 283-286.
-
Arzilli G, Vita ED, Pasquale M, Luca MC, Marzia P, et al. (2024) Innovative techniques for infection control and surveillance in hospital settings and long-term care facilities: A scoping review. Antibiotics 13(1): 77.
-
Silva DS, Smith MJ (2023) Data sharing during pandemics: Reciprocity, solidarity, and limits to obligations. J Bioethical Inq 20(4): 667-672.
-
Wilkinson MD, Dumontier M, Aalbersberg IjJ (2016) The FAIR guiding principles for scientific data management and stewardship. Sci Data 3(1): 160018.
-
Ciecierski-Holmes T, Singh R, Axt M, Brenner S, Barteit S (2022) Artificial intelligence for strengthening healthcare systems in low- and middle-income countries: A systematic scoping review. NPJ Digit Med 5(1): 162.
-
Yang J, Dung N, Thạch P, Nguyen TP, Vu DP, et al. (2023) Generalizability assessment of AI models across hospitals in a low-middle- and high-income country. Nat Commun 15(1): 8270.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia
- Atraumatic Splenic Rupture Secondary to the Use of Anticonvulsants: A Case Report from Libya