Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
Background: Patient safety is a paramount concern in healthcare systems worldwide, remaining a significant challenge de spite advancements in medical technology and clinical practices. To address these issues, the Joint Commission International (JCI) introduced the International Patient Safety Goals (IPSG) framework, aimed at promoting patient safety and minimizing risks across various healthcare settings. This study seeks to evaluate the knowledge and practices of healthcare providers in a tertiary care teaching hospital in Gujarat. The insights obtained will help identify areas for improvement and enhance patient safety initiatives within the hospital. Aim: To assess the knowledge and practice of healthcare providers on International Patient Safety Goals. Methodology: This observational descriptive study was conducted among 100 healthcare workers at the All India Institute of Medical Sciences, Rajkot. The participants included Senior Residents, Junior Residents, Senior Nursing Officers, and Nurs ing Officers. Prior to commencing the study, approval for an expedited review was obtained from the Institutional Ethical Committee. Data collection involved gathering sociodemographic information and assessing knowledge, while practices were evaluated using a structured checklist. Results: A total of 100 healthcare workers (HCWs) participated in the study. The participants comprised Senior Residents (SRs) (15%), Junior Residents (JRs) (35%), Senior Nursing Officers (SNOs) (10%), and Nursing Officers (NOs) (40%). All HCWs had less than 10 years of experience, with a majority being female (55%). Knowledge assessment results from a 20-question questionnaire indicated that SRs scored 58%, JRs 54.71%, SNOs 62%, and NOs 65.63%. Compliance in practice, observed across 1200 practices, revealed rates of 46.34% for SRs, 39.05% for JRs, 47.20% for SNOs, and 68.75% for NOs. Conclusion: Overall, the knowledge and practice compliance rates among healthcare workers in our institute are moder ate. Nursing Officers (NOs) demonstrate higher compliance rates in both IPSG practices and knowledge compared to Senior Residents (SRs), Junior Residents (JRs), and Senior Nursing Officers (SNOs). Compliance rates are notably lower among JRs, indicating a significant area for improvement. Gap analysis revealed a positive gap of 12%, 15%, and 16% among SRs, JRs, and SNOs, respectively, suggesting barriers that prevent effective translation of knowledge into practice. Conversely, a negative gap of -3% among NOs indicates their practice compliance slightly surpasses their knowledge, likely due to practical experience.
Talwar V¹, Radha V², Bhise M*³ and Agrawal A⁴
¹Department of Microbiology, Nursing Officer, PGDHM, B.Sc. Nursing, AIIMS Rajkot, India ²Department of Microbiology, Senior Nursing Officer, , B.Sc. Nursing, AIIMS Rajkot, India ³Department of Microbiology, Assistant Professor, MD DNB Microbiology, AIIMS Rajkot, India ⁴Department of Microbiology, Professor and Head, MD Microbiology, AIIMS Rajkot, India
Abbreviations
JCI: Joint Commission International; IPSG: International Patient Safety Goals; HCWs: Healthcare Workers; SRs: Senior Residents; JRs: Junior Residents; SNOs: Senior Nursing Officers; Nos: Nursing Officers; WHO: World Health Organization; IPSG: International Patient Safety Goals; LASA: Look-Alike and Sound-Alike; HSOPSC: Hospital Survey on Patient Safety Culture; NABH: National Accreditation Board for Hospitals & Healthcare Providers; NDHM: National Digital Health Mission; HAIs: Healthcare-Associated Infections; DALYs: Disability-Adjusted Life Years.
Introduction
Patient safety, as defined by the Joint Commission International (JCI), involves the proactive prevention of harm to patients. This includes a systematic approach to identifying and mitigating risks, ensuring that healthcare processes are meticulously designed to prevent errors and adverse events [1]. The evolution of patient safety thinking has profoundly reshaped the healthcare landscape. Historically, patient safety was predominantly viewed through a legalistic lens, attributing errors primarily to individual failings. However, the transition to a system engineering approach has marked a pivotal shift in this perspective, focusing on understanding and preventing errors through comprehensive systemic changes. This paradigm shifts highlights the critical need for a cultural transformation within healthcare organizations, emphasizing the development of a safety-oriented mindset to effectively mitigate risks and enhance patient care [2, 3]. The World Health Organization (WHO) defines patient safety as the absence of preventable harm to patients during healthcare and the reduction of unnecessary risk to an acceptable minimum. This principle is critically important, as approximately 1 in 10 patients is harmed in healthcare settings, with over 3 million deaths occurring annually due to unsafe care. WHO identifies several common sources of patient harm, including medication errors, surgical errors, and healthcare-associated infections. Medication errors affect 1 in every 30 patients, with many cases being severe or life-threatening. Surgical errors contribute significantly to preventable harm, accounting for 10% of such incidents. Additionally, healthcare-associated infections not only extend hospital stays but also exacerbate antimicrobial resistance and increase financial burdens [4, 5]. Patient safety is a fundamental dimension of care, intricately linked to the complexity of modern medical advances. Errors often result from a combination of circumstances that converge during the care process. Adverse events thus represent a severe public health issue, causing varying degrees of harm to patients and their families. These incidents also contribute to increased costs in the care process and extended hospital stays, underscoring the need for ongoing efforts to enhance patient safety [6, 7].
Recognizing the importance of addressing patient safety concerns, organizations such as the JC) have developed frameworks like the International Patient Safety Goals (IPSG). These goals provide standardized guidelines and best practices to promote patient safety and minimize risks across various healthcare settings The International Patient Safety Goals were developed in 2006 by JCI which were adapted from the JCAHO’s National Patient Safety Goals. The JCI has also updated the versions of IPSG over a period and currently version 2017-2023 is being practiced globally. Above 50% of harm (1 in every 20 patients) is preventable; half of this harm is attributed to medications. Some estimates suggest that as many as 4 in 10 patients are harmed in primary and ambulatory settings, while up to 80% (23.6–85%) of this harm can be avoided [8].
Errors in patient identification can lead to serious issues such as medication, transfusion, and testing errors, as well as procedures being performed on the wrong person. Verbal and telephone communications, particularly patient care orders and reporting critical test results, are highly prone to errors. High-risk medications, known as Look-Alike and Sound-Alike (LASA) medications, pose significant risks for adverse outcomes. In hospitals, wrong-site, wrong-patient surgeries, and incorrect procedures are alarmingly frequent. Contributing factors include poor communication among surgical team members, insufficient patient involvement in site marking, and inadequate verification procedures. Healthcare-Associated Infections (HAIs) are often severe and can be fatal. The International Patient Safety Goals (IPSG), established by JCI in 2006, provide crucial guidelines to enhance patient safety and ensure high-quality care globally [9, 10].
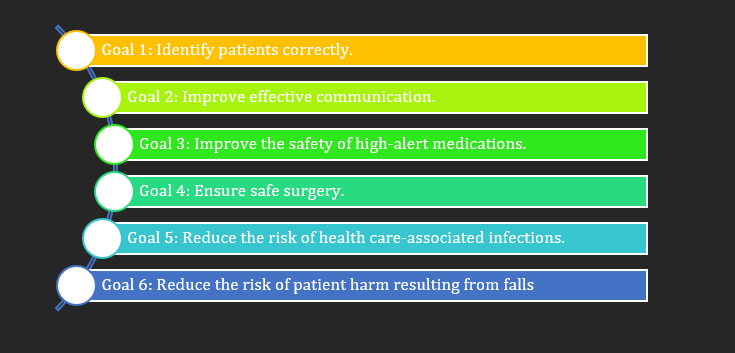
The six IPSGs were established to drive specific improvements in patient safety across healthcare settings. These goals target six critical areas where patient safety is often compromised and provide evidence-based strategies to mitigate risks. The first goal focuses on accurate patient identification, aiming to prevent errors related to medication administration, transfusions, and procedures by ensuring that each patient is correctly identified at every point of care. The second goal addresses effective communication, particularly in the transmission of patient care orders and critical test results, to reduce misunderstandings and errors. The third goal emphasizes the safety of high-alert medications, such as LASA drugs, by implementing strategies to minimize the risk of adverse outcomes. The fourth goal seeks to ensure the correct site, procedure, and patient for surgeries, addressing common issues like wrong-site and wrong-patient surgeries through improved team communication and verification processes. The fifth goal focuses on reducing the risk of HAIs by promoting stringent infection control practices. Finally, the sixth goal aims to reduce the risk of patient harm resulting from falls by implementing preventive measures. Collectively, these goals provide a comprehensive framework for enhancing patient safety and ensuring high-quality care in healthcare institutions worldwide [11].
A study evaluating the Hospital Survey on Patient Safety Culture (HSOPSC) in Indian hospitals found that the average composite positive response rate was 64.8%. High positive responses were seen in areas like teamwork (79%), communication about errors, and hospital management support for patient safety.
However, lower positive responses were noted in staffing and work pace (30%), response to error (50%), communication openness, and reporting patient safety events (both 59%), indicating areas needing improvement [12].
The current status of patient safety in India reflects both significant progress and ongoing challenges. Recently, there has been increased recognition of the importance of patient safety within the Indian healthcare system, leading to the implementation of various initiatives aimed at enhancing safety standards. Notably, India has made substantial strides in establishing regulatory frameworks, such as those set by the National Accreditation Board for Hospitals & Healthcare Providers (NABH), which focus on improving quality and safety in healthcare settings [13]. Additionally, the introduction of the National Digital Health Mission (NDHM) represents a major step towards creating a comprehensive digital health ecosystem that incorporates safety measures. Despite these advancements, considerable issues persist, impacting the overall effectiveness of patient safety efforts and highlighting the need for continued improvement [14].
This study is designed to evaluate the understanding and application of IPSG among healthcare providers at a tertiary care teaching hospital. By assessing both the knowledge and practices related to these goals, the research seeks to identify the strengths and areas requiring improvement within the current safety protocols. The insights gained from this evaluation will be instrumental in guiding the development and implementation of more effective policy measures aimed at enhancing patient safety and improving overall patient outcomes. Through this comprehensive assessment, the study aspires to contribute to the refinement of safety practices and the establishment of robust frameworks that ensure high standards of care within the healthcare facility.
Aim/General Objective
To assess the knowledge and practice of health care providers on International Patient Safety Goals
Specific Objective
- To assess the knowledge of health care providers on International Patient Safety Goals
- To assess the practices of health care providers as per International Patient Safety Goals
- To analyse the gap between knowledge and practice on compliance of International Patient Safety Goals among health care providers
Review Of Literature
The International Patient Safety Goals (IPSG), established by the Joint Commission International (JCI), are crucial for advancing patient safety in healthcare settings worldwide. These goals address key areas essential for preventing harm and enhancing the quality of care. These goals are as elaborated [15, 16, 17]:
Goal 1: Accurate patient identification is a cornerstone of safe and effective healthcare, essential for ensuring that each patient receives the correct treatment and intervention. This process is facilitated by employing at least two distinct patient identifiers, which significantly reduces the likelihood of errors. These identifiers typically include information such as the patient’s full name, date of birth, medical record number, or other unique identifiers like a patient ID wristband.
Goal 2: Effective communication among healthcare providers is a vital objective for enhancing patient safety and ensuring high-quality care. This goal focuses on the systematic and clear exchange of information between all members of the healthcare team, including physicians, nurses, pharmacists, and other healthcare professionals.
Goal 3: The safe handling of high-alert medications is a critical component of patient safety, given the elevated risk of severe harm associated with these drugs. High-alert medications are those that have a higher likelihood of causing significant patient harm when used incorrectly. These medications include, but are not limited to, anticoagulants, insulin, opioids, chemotherapeutic agents, and certain antibiotics. Due to their potency and the narrow therapeutic window, improper use of high-alert medications can lead to serious adverse effects, including overdose, organ damage, or even death.
Goal 4: Preventing surgical errors is a critical component of patient safety, and achieving this involves meticulous verification processes to ensure the correct procedure, patient, and surgical site are identified and confirmed. This multi-step verification process is designed to minimize the risk of wrong- site, wrong-procedure, or wrong-patient surgeries, which can have devastating consequences for patients.
Goal 5: Reducing the incidence of healthcare-associated infections (HAIs) is a top priority in patient safety due to the significant impact these infections can have on patient outcomes. HAIs, which include infections acquired during the course of receiving healthcare treatment, can lead to severe complications, extended hospital stays, increased healthcare costs, and even mortality. Addressing HAIs requires a comprehensive, multi-faceted approach to infection prevention and control.
Goal 6: Reducing fall risks within healthcare environments is a crucial aspect of patient safety, as falls can lead to severe injuries, prolonged hospital stays, and diminished quality of life. The goals related to fall prevention involve a proactive and comprehensive approach to identifying and mitigating factors that contribute to falls.
Together, these objectives are designed to foster a safer healthcare environment and enhance patient safety.
Errors in patient identification pose a serious challenge in healthcare settings. The Joint Commission reported that between 2014 and 2017, approximately 12.3% of sentinel events were attributed to mistakes in patient identification [18]. These errors can lead to severe consequences, including incorrect treatments or misdiagnoses. Furthermore, research has shown that 35% of denied hospital claims stem from issues related to inaccurate patient identification or incomplete information. This not only impacts the quality of patient care but also results in significant financial implications for healthcare providers. Ensuring accurate patient identification is crucial for both patient safety and operational efficiency, highlighting the need for robust systems and protocols to address and mitigate these risks [19].
A study conducted in emergency departments across India revealed that 53% of clinicians encountered at least one critical incident over the past year due to poor communication. This underscores the substantial effect that communication barriers can have on both patient care and safety. The study identified several factors contributing to these communication challenges. One major issue is the diverse range of languages spoken by clinicians and patients, which can lead to misunderstandings and complicate interactions. Furthermore, high patient volumes, low levels of health literacy, and hierarchical dynamics within the workplace further intensify these communication difficulties. Addressing these issues is essential for improving patient safety and the overall effectiveness of emergency care [20].
According to statistics from the WHO, medication- related harm impacts approximately 1 in 30 patients within healthcare settings. Of these incidents, over 25% are classified as severe or life-threatening. Furthermore, medications are implicated in around 50% of all avoidable harm within healthcare systems. This highlights the critical need for stringent medication safety practices and error prevention strategies, as a significant portion of patient safety issues can be traced back to medication-related errors. Addressing these challenges is crucial for enhancing patient outcomes and reducing the incidence of preventable harm in healthcare environments [18, 21]. Surgical errors represent a major global health issue. WHO estimates that complications occur in approximately 3-16% of surgeries performed worldwide. Additionally, the global prevalence of surgical errors and related adverse events is estimated to be between 5-10% of all surgeries. These statistics underscore the critical importance of improving surgical practices and safety measures to reduce the incidence of errors and enhance patient outcomes. Addressing these challenges requires a concerted effort to implement effective safety protocols, improve surgical training, and foster a culture of continuous quality improvement in surgical care [22, 23]. Falls rank as the second leading cause of unintentional injury deaths globally, with approximately 684,000 fatalities each year. They are particularly prevalent among older adults, with 28-35% of individuals aged 65 and older experiencing falls annually; this rate increases to 32-42% for those aged 70 and above. Each year, about 37.3 million falls are severe enough to necessitate medical attention, resulting in over 38 million disability-adjusted life years (DALYs) lost [18]. In India, the prevalence of falls among the elderly is notably high, affecting 53% of individuals over the age of 65. This rate significantly surpasses those observed in other countries, such as the USA, where the prevalence is 30%, and Japan, where it is 13.7%. These figures highlight the urgent need for targeted interventions and preventive measures to address the high incidence of falls and their severe impact on health and quality of life, especially in India [24, 25]. A study conducted at a tertiary care hospital in North India reviewed 394 patient records to evaluate adherence to IPSG. The audit found that 339 records (86%) complied with all six IPSG standards. Among these goals, the highest compliance rate was achieved for ensuring safe surgery (fourth goal), with a perfect 100% compliance rate. In contrast, the lowest compliance was observed in the areas of improving effective communication (second goal), minimizing healthcare- associated infections (fifth goal), and reducing patient harm from falls (sixth goal), with compliance rates of 81%, 80%, and 78%, respectively. Additionally, a survey conducted among 60 doctors, 86 nurses, and 76 technicians assessed awareness of these safety goals. The results showed the highest level of awareness among nurses (84.8%), followed by doctors (81.7%) and technicians (80.2%) [26]. In a separate study conducted at a tertiary care hospital in India, involving a sample of 306 healthcare professionals—comprising doctors, nurses, and paramedics—the findings indicated a significant gap in awareness of the IPSG. Specifically, 51% of the doctors were found to be unaware of the IPSG standards, while 49% had only partial knowledge of these guidelines. Among the nursing staff, the situation was somewhat different: 21% were both knowledgeable about and consistently followed the IPSG goals, 23.5% were completely unaware of them, and the remaining 55% had partial awareness or were aware of some aspects but lacked comprehensive understanding of the complete set of standards. This distribution highlights varying levels of awareness and adherence among different categories of healthcare professionals, underscoring the need for targeted educational interventions to improve compliance with patient safety protocols [27].
In a research study examining the understanding, attitudes, and implementation of international patient safety goals among staff nurses in selected Indian hospitals, data from a sample of 60 nurses revealed the following insights: 58.8% of the participants had insufficient knowledge, 28.33% possessed a moderate level of knowledge, and only 13.33% demonstrated a high level of knowledge regarding IPSG. Concerning their practices, 76.67% of nurses exhibited strong adherence to safety practices, whereas 23.33% had poor practice levels. Attitudes towards patient safety goals varied, with 63.33% holding positive attitudes and 36.67% displaying negative attitudes [28].
Amaal Abousallah’s 2018 study, titled “The Impact of Application of International Safety Goals on Patient Safety Culture: A Field Study in Private Hospitals in the City of Amman,” provides a comprehensive evaluation of how the implementation of IPSG influences patient safety culture in private hospitals located in Amman, Jordan. The study adopts a descriptive and analytical research design to assess the relationship between IPSG adherence and the quality of patient safety culture. The research focused on data collected from a sample of 156 medical staff members working in Joint Commission International-accredited hospitals within the city. The methodological approach enabled a thorough analysis of both the extent of IPSG implementation and its impact on various aspects of patient safety culture. Key findings of the study indicate a high level of consensus among medical staff regarding the application of IPSG in their clinical practice. This strong agreement reflects a significant alignment with the safety goals, which, in turn, is associated with a positive shift in the safety culture within these healthcare settings. Abousallah’s study underscores a robust positive correlation between the rigorous application of IPSG and improvements in patient safety culture, suggesting that adherence to these international safety standards plays a critical role in fostering a safer healthcare environment. The study’s conclusions highlight that each of the IPSG variables—such as improving communication among healthcare providers, ensuring correct patient identification, and maintaining effective infection control practices— contributes positively to enhancing patient safety culture. Abousallah advocates for the continuous reinforcement and integration of these safety goals into hospital protocols and staff training to sustain and further advance patient safety outcomes. By emphasizing the importance of ongoing commitment to IPSG, the study provides valuable insights for healthcare administrators and policymakers, suggesting that sustained adherence to international safety standards is essential for optimizing patient care and fostering a culture of safety within healthcare organizations [29].
Additionally, a cross-sectional observational study on patient safety practice compliance was conducted in a tertiary care hospital in India, focusing on the intensive care unit, operation theatre, and in-patient wards. The research, which involved direct observations and interviews with staff, revealed differing levels of adherence to safety practices. Some areas exhibited only partial compliance or less, while others demonstrated satisfactory adherence to patient safety protocols [30].
Akhu-Zaheya LM, et al. [28] conducted a study to evaluate the effectiveness of training programs aimed at improving the knowledge and practice of IPSGs among nurses in Jordanian hospitals. The study highlighted the critical role of continuous education and training in enhancing patient safety practices. The researchers employed a quasi-experimental design, involving pre- and post-training assessments to measure changes in nurses’ knowledge and practices related to IPSGs. The findings indicated a significant improvement in both knowledge and practice post-training, underscoring the effectiveness of structured training programs in fostering a culture of safety within healthcare settings. The study also emphasized the importance of organizational support and the need for regular updates to training content to keep pace with evolving patient safety standards. By focusing on systemic changes and continuous professional development, the research contributes to the broader understanding of how targeted educational interventions can lead to substantial improvements in patient safety outcomes [28]. Failure to adhere to patient safety standards can stem from several factors, including insufficient awareness and training, limited resources, hierarchical barriers that hinder communication, workload pressures that prioritize efficiency over safety, resistance to change, inadequate monitoring, and the inherent complexity of healthcare systems. These challenges can obstruct healthcare providers’ ability to effectively implement and sustain safety protocols. To tackle these issues, a comprehensive strategy is needed, involving the education and empowerment of healthcare professionals, adequate resource allocation, the promotion of open communication and teamwork, the establishment of robust monitoring systems, and the cultivation of a safety-focused culture within healthcare organizations. By addressing these foundational issues, healthcare institutions can reduce risks and enhance adherence to safety standards, thereby improving the quality of care and patient outcomes [32].
Methodology
Study Location
This study was conducted at the tertiary care teaching institute, Gujarat.
Study Population
The study population included healthcare workers- senior residents, junior residents, and nursing officers of the hospital.
Study Design
This was a descriptive study aiming to assess the knowledge and practice of patient safety standards among healthcare providers.
Study Type
The study was an observational study, where data was collected through direct observation and questionnaire administration.
Data Collection
Data was collected prospectively, starting from June 1 to August 31, 2024.
Data Collection Tools
The data collection for this study involved two primary methods: an observational checklist and a direct questionnaire. The observational checklist was used to assess adherence to patient safety standards, while the questionnaire aimed to evaluate the knowledge and understanding of the IPSG among healthcare providers.
The questionnaire was divided into following parts:
- The first part consisted of demographic data of the samples such as age, sex, cadre, qualification, years of experience.
- The second part of the questionnaire tool had 20 questions assessing the knowledge of healthcare workers on IPSG The observational checklist included specific details such as the department in which the observation took place, the professional cadre of the individual being evaluated, and the criteria used for assessment related to patient safety standards.
Sample Size
The sample size for the study was 100 participants.
Mode of Sample Collection
Participants were selected using random stratified sampling methods to ensure representation across different categories of healthcare providers. Only those participants who provided consent while completing the questionnaire were selected for the observational assessment.
Pre-test and Validation of Questionnaire
Prior to data collection, the questionnaire and observational tool underwent pre-testing and validation by a team of experts at INI Rajkot to ensure its reliability and validity for the study context.
Ethical Considerations
- This study does not cause any harm or manipulation to the samples or patients
- Informed consent was taken from all the samples
- The data collection was started after getting an approval from the IEC of the institute.
Operational Definitions
Knowledge: Knowledge refers to the understanding and awareness of specific information, concepts, and principles related to patient safety goals as assessed by a structured questionnaire. In this study, it encompasses the healthcare provider’s ability to recall, recognize, and apply relevant information regarding the IPSG in clinical practice. It is quantified through responses to a 20-item questionnaire, where correct answers indicate a higher level of knowledge regarding patient safety protocols. Practice: Practice refers to the actual actions taken by healthcare providers in relation to patient safety standards. It is evaluated using an observational checklist that records specific compliance with patient safety standards during the delivery of healthcare services. Observations focus on actions that align with the IPSG.
Inclusion criteria
Healthcare workers including Senior Residents, Junior Residents, Senior Nursing officers and Nursing Officers of All India Institute of Medical Sciences Rajkot.
Exclusion Criteria
Healthcare workers such as faculties, HODs and those who did not fill the questionnaire tool were not included in this study.
Statistical Analysis
The collected data was meticulously organized and entered into a master Excel spreadsheet to facilitate thorough analysis. Each dataset was categorized by specific variables, such as demographic information and responses from the questionnaires and observational checklists. Once the data was compiled, it was transformed into tables and graphs for clearer interpretation.
Results
The present study was conducted at INI Rajkot among 100 healthcare professionals involving SR, JR, SNO, NO.
- The data obtained was tabulated and analysed under following headings:
- Demographic details of the participants
- Knowledge score on IPSG among participants
- Compliance rate on IPSG among participants
- Gap Analysis of knowledge on IPSG and practice among participants
Demographic Data
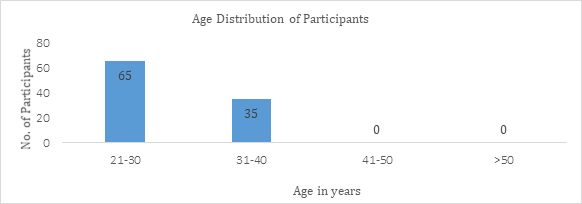
| Age in (years) | Frequency | Percentage |
|---|---|---|
| 21-30 | 65 | 65% |
| 31-40 | 35 | 35% |
| 41-50 | 0 | 0 |
| >50 | 0 | 0 |
Table 1: Distribution of the Study Participants as Per Age Group- N=100.
In this study, the sample consisted of 100 participants, with 65 individuals (65%) aged between 21-30 years, and 35 individuals (35%) aged between 31- 40 years. Notably, there were no participants in the age group of 41 to 50 years or older.
| Sex | Frequency | Percentage |
|---|---|---|
| Male | 45 | 45% |
| Female | 55 | 55% |
Table 2: Distribution of the Study Participants as Per Sex- N=100.
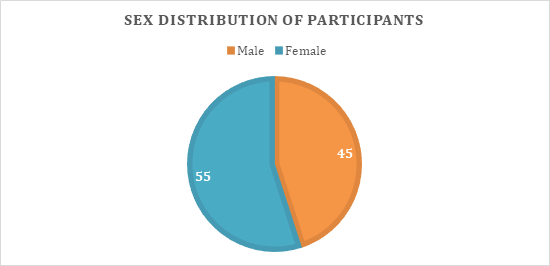
The study included a total of 100 participants, consisting of 55 (55%) females and 45 (45%) males.
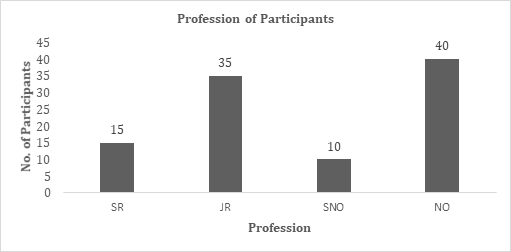
| Profession | Frequency | Percentage |
|---|---|---|
| SR | 15 | 15 |
| JR | 35 | 35 |
| SNO | 10 | 10 |
| NO | 40 | 40 |
Table 3: Distribution of the Study Participants as Per Profession- N=100.
In this study, the sample of 100 participants included 15
individuals (15%) who were Senior Residents, 35 individuals (35%) who were Junior Residents, 10 individuals (10%) who were Senior Nursing Officers, and 40 individuals (40%) who were Nursing Officers.
| Qualification | Frequency | Percentage |
|---|---|---|
| Diploma | 25 | 25 |
| Graduate | 50 | 50 |
| Post Graduate | 25 | 25 |
| PhD | 0 | 0 |
Table 4: Distribution of the Study Participants as Per Qualification- N=100.
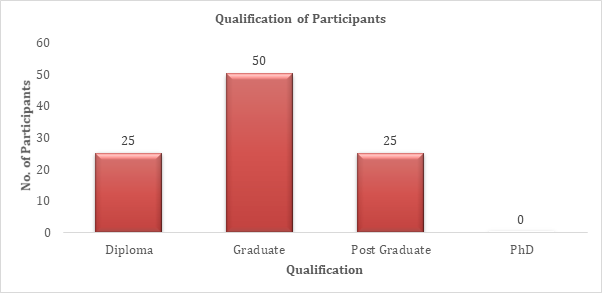
The study included a sample size of 100 participants, with the following qualifications: 25 (25%) held diplomas, 50 (50%) were graduates, 25 (25%) had postgraduate degrees, and none possessed a PhD.
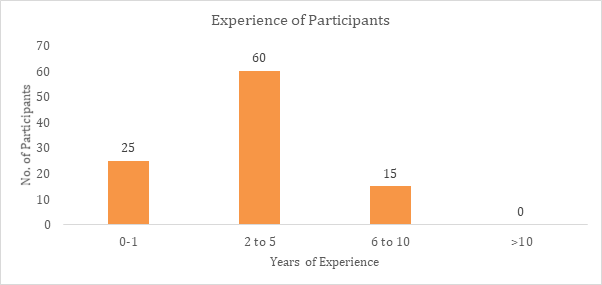
| Years of Experience | Frequency | Percentage | |
|---|---|---|---|
| 0-1 | 25 | 25 | |
| 2 to 5 | 60 | 60 | |
| 6 to 10 | 15 | 15 | |
| >10 | 0 | 0 | |
| Q No. | Question | Correct (%) | incorrect (%) |
| 1 | IPSG stands for | 61 | 39 |
| 2 | Positive patient identification’ under IPSG Goal -1 includes all EXCEPT | 42 | 58 |
| 3 | Which IPSG goal includes the recommendation to ‘Implement Evidence-Based Practices to Prevent Central Line-Associated Bloodstream Infections’? | 53 | 47 |
| 4 | Which IPSG goal pertains to ensuring the accuracy of patient records? | 48 | 52 |
| 5 | Which IPSG goal is directly related to the prevention of wrong-site, wrong- procedure, and wrong-patient surgery? | 45 | 55 |
| 6 | To reduce the risk of patient harm from falls, the healthcare team should | 49 | 51 |
| 7 | The ‘Universal Protocol’ for preventing surgical errors is associated with which IPSG goal? | 41 | 59 |
| 8 | The IPSG goal that involves ‘Medication Reconciliation’ is aimed at preventing | 46 | 54 |
| 9 | A surgical team is preparing for a procedure. According to IPSG Goal 4, what is the final step they must take before making the incision? | 42 | 58 |
| 10 | A nurse receives a verbal order for a high-alert medication. What is the most appropriate IPSG-compliant response? | 41 | 59 |
| 11 | To adhere to IPSG Goal 6, what should be included in a fall prevention program for an elderly patient? | 42 | 58 |
| 12 | To prevent healthcare-associated infections, IPSG recommends specific hand hygiene practices. Which of the following is NOT recommended? | 75 | 25 |
| 13 | A patient is scheduled for surgery, and two patients have the same name. What IPSG-compliant action should the surgical team take to ensure correct patient identification? | 47 | 53 |
| 14 | In the context of IPSG, ‘Medication Reconciliation’ should be performed | 45 | 55 |
| 15 | What is the purpose of using two patient identifiers in IPSG 1? | 53 | 47 |
| 16 | Which of the following is an example of a strategy to improve effective communication to prevent errors and ensure safe care? | 68 | 32 |
| 17 | According to IPSG, what is the best practice to reduce the risk of patient harm from falls in a hospital setting? | 83 | 17 |
| 18 | Which IPSG goal emphasizes the use of ‘read-back’ technique in verbal or telephone communication? | 51 | 49 |
| 19 | Which action best demonstrates adherence to the IPSG goal of reducing healthcare- associated infections? | 95 | 5 |
| 20 | The recommendation to ‘Measure and Reduce the Risk of Patient Harm from Falls’ falls under which IPSG goal? | 57 | 43 |
Table 5: Distribution of the Study Participants as Per Years of Experience- N=100.
The study involved a sample size of 100 participants, with 25% having 0-1 years of experience, 60% having 2-5 years of experience, 15% with 6-10 years of experience, and none exceeding 10 years of experience.
Knowledge Assessment of the Study Participants
The mean score on the questionnaire indicated that 54.2% of the responses were correct, while 45.8% were incorrect, based on 20 questions answered by the 100 participants.
| Knowledge Score | Percentage | Interpretation |
|---|---|---|
| 16-20 | 80-100 % | Good Knowledge |
| 15-Nov | 55-79 % | Moderate knowledge |
| 0-10 | 0-54% | Poor Knowledge |
Table 6: Knowledge Assessment Criteria on IPSG among Participants (N=100).
| Mean Knowledge Score | Percentage |
|---|---|
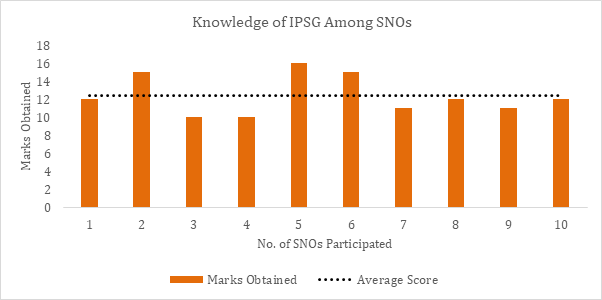
| 11.6 | 58% |
Table 7: Knowledge Score on IPSG Among Senior Residents – N = 15.
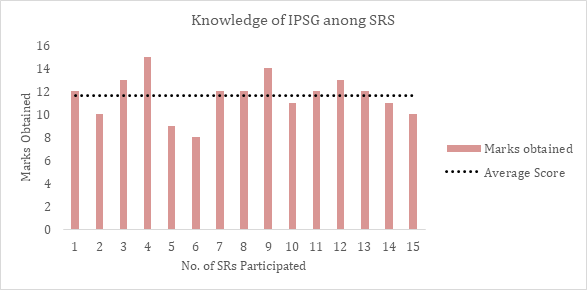
The average score for Senior Residents (SRs) was 11.6, corresponding to 58%, indicating that they possess moderate knowledge of the International Patient Safety Goals (IPSG).
| Mean Knowledge Score | Percentage |
|---|---|
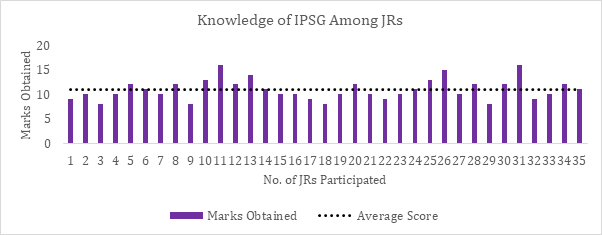
| 10.94 | 54.71% |
Table 8: Knowledge Score on IPSG Among Junior Residents – N = 30.
The average score for Junior Residents (JRs) was 10.94, corresponding to 54.71%, indicating that they possess moderate knowledge of the International Patient Safety Goals (IPSG).
| Mean Knowledge Score | Percentage |
|---|---|
| 12.4 | 62% |
Table 9: Knowledge Score on IPSG Among Senior Nursing Officers – N = 10.
The average score for Senior Nursing Officers (SNOs) was 12.4, corresponding to 62%, indicating that they possess moderate knowledge of the International Patient Safety Goals (IPSG).
| Mean Knowledge Score | Percentage |
|---|---|
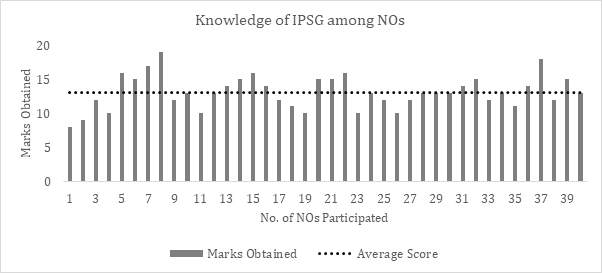
| 13.13 | 65.63% |
Table 11: Knowledge Score on IPSG Among Nursing Officers – N = 40.
The average score for Nursing Officers (NOs) was 13.13, corresponding to 65.63%, indicating that they possess moderate knowledge of the International Patient Safety Goals (IPSG).
| Sl.no. | Profession | Mean Knowledge Score | Percentage |
|---|---|---|---|
| 1. | Senior Residents | 11.6 | 58% |
| 2. | Junior Residents | 10.94 | 54.71% |
| 3. | Senior Nursing Officers | 12.4 | 62% |
| 4. | Nursing Officers | 13.13 | 65.63% |
Table 10: Profession Wise Distribution of Knowledge Score – N= 100.
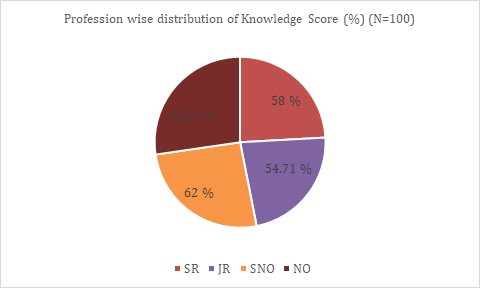
Based on the knowledge assessments on International Patient Safety Goals (IPSG) among healthcare workers, the results indicate varying levels of knowledge across different cadres.
Senior Residents (SRs) demonstrated an average knowledge score of 11.6, corresponding to a knowledge rate of 58%. Junior Residents (JRs) had a slightly lower average knowledge score of 10.94, with a knowledge rate of 54.71%.
Senior Nursing Officers (SNOs) showed a higher level of knowledge, with an average score of 12.4 and a knowledge rate of 62%. Nursing Officers (NOs) achieved the highest scores, with an average of 13.13 and a knowledge rate of 65.63%.
Compliance Rate on IPSG Among Participants
| GOAL | Compliance | Noncompliance |
|---|---|---|
| Goal 1 | 25 | 15 |
| Goal 2 | 25 | 20 |
| Goal 3 | 20 | 25 |
| Goal 4 | 16 | 14 |
| Goal 5 | 15 | 25 |
| Goal 6 | 8 | 27 |
| TOTAL | 109 | 126 |
Table 12: Compliance of IPSG Practices for Senior Residents (SRs).
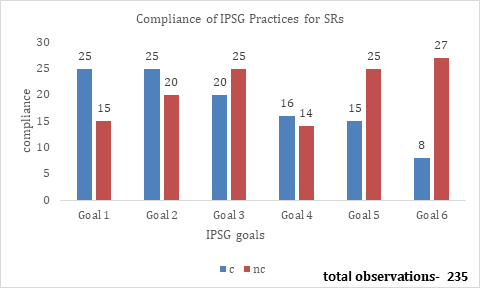
In this study, compliance among SRs was evaluated, encompassing a total of 235 opportunities. The distribution of these opportunities varied to reflect different areas of focus and compliance rates. Specifically, Goal 1 had 40 opportunities, with 25 compliant and 15 non-compliant cases. Goal 2 was allocated 45 opportunities, resulting in 25 compliant and 20 non-compliant cases. Similarly, Goal 3 also received 45 opportunities, with 20 compliant and 25 non- compliant cases.
Goal 4 comprised 30 opportunities, yielding 16 compliant and 14 non-compliant cases. Goal 5 had 40 opportunities, showing 15 compliant and 25 non-compliant cases. Finally, Goal 6 included 35 opportunities, resulting in 8 compliant and 27 non-compliant cases.
| Goal | Compliance | Noncompliance |
|---|---|---|
| Goal 1 | 30 | 40 |
| Goal 2 | 40 | 30 |
| Goal 3 | 35 | 25 |
| Goal 4 | 10 | 20 |
| Goal 5 | 5 | 35 |
| Goal 6 | 3 | 42 |
| TOTAL | 123 | 192 |
Table 13: Compliance of IPSG Practices for Junior Residents.
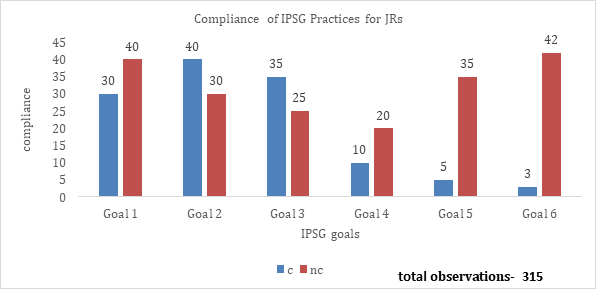
Figure 13: Compliance of IPSG Practices for Junior Residents. In this study, a total of 315 compliance opportunities for Junior Residents (JRs) were evaluated. Specifically, Goal 1 was assigned 70 opportunities, with 30 compliant and 40 non- compliant cases. Similarly, Goal 2 received 70 opportunities, resulting in 40 compliant and 30 non-compliant cases. Goal 3 was allocated 60 opportunities, yielding 35 compliant and 25 non-compliant instances. In contrast, Goal 4 had
30 opportunities, showing 10 compliant and 20 non- compliant cases. Goal 5 was given 40 opportunities, with only 5 compliant and 35 non-compliant cases. Lastly, Goal 6 received 45 opportunities, resulting in 3 compliant and 42 non-compliant cases. The overall compliance for Junior Residents was 123, while non-compliance 192.
| Goal | Compliance | Noncompliance |
|---|---|---|
| Goal 1 | 35 | 25 |
| Goal 2 | 40 | 20 |
| Goal 3 | 15 | 15 |
| Goal 4 | 10 | 20 |
| Goal 5 | 5 | 15 |
| Goal 6 | 13 | 37 |
| TOTAL | 118 | 132 |
Table 14: Compliance of IPSG Practices for Senior Nursing Officers.
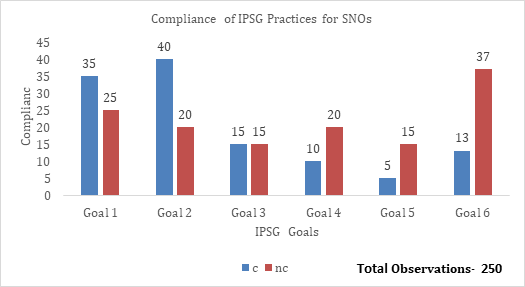
In this study, a total of 250 compliance opportunities for Senior Nursing Officers (SNOs) were evaluated, reflecting a strategic focus on enhancing patient safety in critical areas. Specifically, Goal 1 was assigned 60 opportunities, with 35 compliant and 25 non-compliant cases. Goal 2 also received 60 opportunities, resulting in 40 compliant and 20 non- compliant cases. Goal 3 had 30 opportunities, yielding 15 compliant and 15 non-compliant instances. In contrast, Goal
4 was assigned 30 opportunities, showing 10 compliant and 20 non-compliant cases. Goal 5 had 20 opportunities, with only 5 compliant and 15 non-compliant cases. Lastly, Goal 6 received 50 opportunities, resulting in 13 compliant and 37 non-compliant cases. The overall compliance for Senior Nursing Officers was 118, while non-compliance totalled 132.
| Goal | Compliance | Noncompliance |
|---|---|---|
| Goal 1 | 50 | 20 |
| Goal 2 | 52 | 23 |
| Goal 3 | 50 | 15 |
| Goal 4 | 28 | 22 |
| Goal 5 | 50 | 25 |
| Goal 6 | 45 | 20 |
| TOTAL | 275 | 125 |
Table 15: Compliance of IPSG Practices for Nursing Officers.
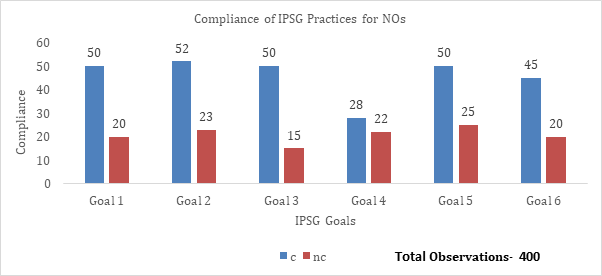
In this study, a total of 400 compliance opportunities for Nursing Officers (NOs) were evaluated. Goal 1 was assigned 70 opportunities, resulting in 20 compliant and 30 non- compliant cases. Goal 2 received 75 opportunities, with 52 compliant and 23 non-compliant instances. Goal 3 had 65 opportunities, yielding 50 compliant and 15 non-compliant cases. In contrast, Goal 4 was allocated 60 opportunities, showing 28 compliant and 22 non-compliant cases. Goal 5 received 75 opportunities, resulting in 50 compliant and 25 non-compliant cases. Lastly, Goal 6 was assigned 65 opportunities, achieving 45 compliant and 20 non-compliant cases. The overall compliance for Nursing Officers was 275, while non-compliance totalled 125.
| Sl. No | Category | Compliance | Compliance (%) | Non- Compliance | Non- Compliance (%) | Total Practices |
|---|---|---|---|---|---|---|
| 1 | SR | 109 | 46.38 | 126 | 53.62 | 235 |
| 2 | JR | 123 | 39.05 | 192 | 60.95 | 315 |
| 3 | SNO | 118 | 47.2 | 132 | 52.8 | 250 |
| 4 | NO | 275 | 68.75 | 125 | 31.25 | 400 |
| Total opportunities= 1200 |
Table 16: Profession Wise Compliance Rate on IPSG Practice.
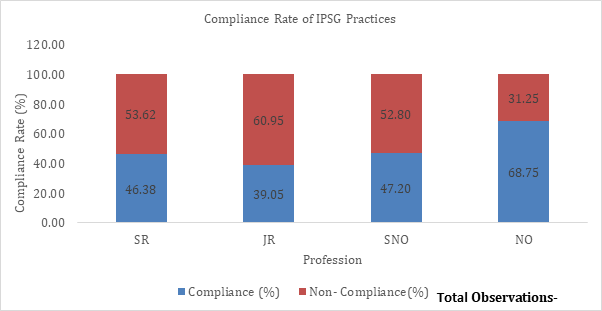
In this study, a total of 1,200 observations of IPSG practices were conducted, distributed as follows: 235 practices for Senior Residents (SRS), 315 for Junior Residents (JR), 250 for Senior Nursing Officers (SNO), and 400 for Nursing Officers (NO). The distribution was tailored to each group’s specific roles, with Nursing Officers receiving the most observations due to their extensive hands-on patient care, Junior Residents focusing on direct patient interaction, Senior Residents being involved in patient care procedures and consultations, and Senior Nursing Officers engaging primarily in managerial activities. The compliance rates observed were 46.38% for SRS, 39.05% for JR, 47.20% for SNO, and 68.75% for NO.
Gap Analysis of Knowledge and Practice on IPSG Among the Study Participants
| SRs | JRs | SNOs | NOs | |
|---|---|---|---|---|
| Knowledge | 58% | 54.71% | 62% | 65.63% |
| Practice | 46.34% | 39.05% | 47.20% | 68.75% |
| Gap Analysis | 12% | 16% | 15% | -3% |
Table 17: Gap Analysis of Knowledge and Practice on IPSG Among the Study Participants.
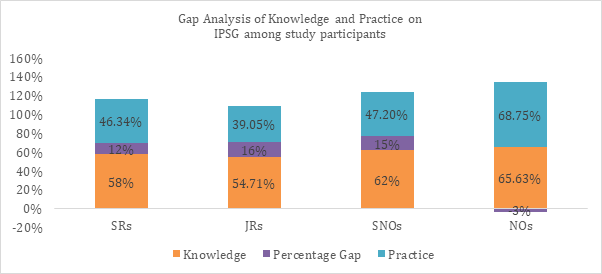
Figure 17: Gap Analysis of Knowledge and Practice on IPSG Among the Study Participants. The gap analysis of knowledge and practice scores among healthcare workers (HCWs) reveals significant disparities across different cadres. Senior Residents (SR) exhibit a 12% positive gap, Junior Residents (JR) show a 16% positive gap, and Senior Nursing Officers (SNO) have a 15% positive gap, indicating that these groups possess greater knowledge than what is demonstrated in their practice. This suggests the presence of barriers to translating knowledge into practice, highlighting the need for targeted interventions. In contrast, Nursing Officers (NO) present a -3% negative gap, indicating that their practice scores slightly surpass their knowledge scores, likely due to the compensatory effect of practical experience. These findings underscore the necessity for tailored strategies to bridge the knowledge-practice gap, particularly aimed at enhancing the practical application of knowledge among SRs, JRs, and SNOs.
Discuission
The study was conducted at a tertiary care teaching hospital involving 100 healthcare workers over the period of June 1 to August 31, 2024. A questionnaire was distributed to participants, allowing them 15 days (June 1–June 15, 2024) to complete the Google form. Following this, observations to evaluate compliance with IPSG practices commenced and continued for 1.5 months (June 17–August 31, 2024). The study aimed to assess the knowledge and practices of healthcare workers concerning IPSG within the institute. To ensure proper evaluation, two nursing officers and two senior residents were appointed and received specialized training to monitor compliance with IPSG practices.
Profile of Study Participants
Table 1 and 2 In this study, out of 100 participants, 55% were females (n=55) and 45% were males (n=45). The age distribution showed that a majority, 65% (n=65), were aged between 21-30 years, while 35% (n=35) were aged between 31-40 years. Notably, there were no participants in the age group of 41-50 years or older. These findings align with a similar study conducted by Joshi DC et al. [23], which analysed the demographic distribution of healthcare workers in the context of the International Patient Safety Goals (IPSG). In their study, the sample consisted of 120 healthcare workers, with 60% females and 40% males. The age distribution was predominantly younger, with 70% of participants aged between 21-30 years, 25% aged between 31-40 years, and only 5% aged 41 years or older [23]. Both studies observed a lack of participants aged 41-50 years or older, which could influence the generalizability of the findings to older age groups.
Table 3 In this study, the sample of 100 participants included 15 individuals (15%) who were Senior Residents (SR), 35 individuals (35%) who were Junior Residents (JR), 10 individuals (10%) who were Senior Nursing Officers (SNO), and 40 individuals (40%) who were Nursing Officers (NO). These findings can be contextualized by comparing them to similar studies on the International Patient Safety Goals (IPSG).
For instance, a study by Joshi DC, et al. [23] analyzed the demographic distribution of 394 healthcare workers in a tertiary care hospital in Northern India. This study provided valuable insights into overall awareness and compliance with IPSG, although it did not specify the similar cadre- wise distribution of participants. The large sample size and comprehensive analysis in Joshi and Saini’s study highlight the general trends in IPSG awareness and compliance among healthcare workers, which can be compared to the specific cadre distributions in our study [23].
Similarly, a study by Ananya R,et al. [24], examined adherence to IPSG among 306 healthcare workers in a tertiary care cardiac center in India. This study focused on overall compliance levels and the factors influencing adherence to IPSG but also did not provide cadre-specific details. The findings from Ananya et al.’s study underscore the importance of understanding the broader compliance trends and the challenges faced by healthcare workers in implementing IPSG [24].
Both studies underscore the importance of understanding demographic patterns and the need for targeted interventions to enhance IPSG implementation across various healthcare settings. The consistency in the representation of healthcare workers in these studies and our study highlights the need for focused strategies to improve patient safety outcomes. By comparing our cadre- specific findings with the broader trends observed in these studies, we can better tailor interventions to address the specific needs and challenges faced by different groups of healthcare workers, ultimately enhancing the effectiveness of IPSG implementation.
Table 4 In this study, the sample of 100 participants included 25 individuals (25%) with diplomas, 50 individuals (50%) who were graduates, and 25 individuals (25%) with postgraduate degrees, with none possessing a PhD. These findings can be contextualized by comparing them to similar studies on the qualifications of healthcare workers. For instance, a study by Joshi DC, et al. [23] titled “Awareness and Compliance to International Patient Safety Goals among Healthcare Personnel of a Tertiary Care Hospital in Northern India” analysed the qualifications of 394 healthcare workers [23].
Although the study did not specify the exact distribution of qualifications, it provided valuable insights into the overall awareness and compliance with IPSG among healthcare personnel. Notably, there are no studies specifying the cadre- wise distribution included in our study [27, 28, 29].
Table 5 In this study, the sample of 100 participants included 25% with 0-1 years of experience, 60% with 2-5 years of experience, and 15% with 6-10 years of experience, with none exceeding 10 years. These findings can be contextualized by comparing them to similar studies on the experience levels of healthcare workers in relation to International Patient Safety Goals (IPSG). For instance, the study by Joshi DC, et al. [23] analysed the awareness and compliance with IPSG among 394 healthcare workers, providing valuable insights into overall compliance and awareness levels, although it did not specify the exact distribution of years of experience [23]. Additionally, a study on the implementation of IPSG in a tertiary care hospital found that compliance with IPSG was higher among those with more years of experience, aligning with our findings that a significant portion of participants had 2-5 years of experience [24].
Furthermore, the study on patient safety culture and the implementation of IPSG highlighted the significant role of experience in achieving better compliance rates [20]. Notably, there are no studies specifying the cadre-wise distribution included in our study, which adds a unique dimension to our research.
- Knowledge and
- Practice among study
- Participants
Table 18: In this study, the sample of 100 participants
Table 8-12: The average score for Senior Residents (SRs) was 11.6, corresponding to 58%, indicating that they possess moderate knowledge of the International Patient Safety Goals (IPSG). The average score for Junior Residents (JRs) was 10.94, corresponding to 54.71%, indicating moderate knowledge of IPSG. The average score for Senior Nursing Officers (SNOs) was 12.4, corresponding to 62%, and for Nursing Officers (NOs) it was 13.13, corresponding to 65.63%, both indicating moderate knowledge of IPSG. These findings can be contextualized by comparing them to similar studies on IPSG compliance among healthcare workers. For instance, the study by Joshi DC, et al. [23] analyzed the awareness and compliance with IPSG among 394 healthcare workers, revealing high levels of awareness and compliance, particularly among nurses, with doctors showing an awareness level of 81.7% [23]. Another study by Ananya R, et al. [24] on adherence to IPSG in a tertiary care cardiac centre found that overall compliance was highest among doctors (72%), followed by nurses (69%) and paramedics (68%) [24]. Additionally, a study on the impact of IPSG implementation in healthcare settings highlighted the importance of targeted training and experience in achieving better compliance rates [30]. These studies highlight the significant role of targeted training in achieving better compliance rates. Notably, there are no studies specifying the cadre-wise distribution included in our study, which adds a unique dimension to our research.
Table 13-17: In our study, a total of 1,200 observations of IPSG practices were conducted, distributed among different healthcare worker groups: 235 practices for Senior Residents (SRS), 315 for Junior Residents (JR), 250 for Senior Nursing Officers (SNO), and 400 for Nursing Officers (NO). This distribution was tailored to each group’s specific roles, with Nursing Officers receiving the most observations due to their extensive hands-on patient care, Junior Residents focusing on direct patient interaction, Senior Residents being involved in patient care procedures and consultations, and Senior Nursing Officers engaging primarily in managerial activities. The compliance rates observed were 46.38% for SRS, 39.05% for JR, 47.20% for SNO, and 68.75% for NO.
Similar studies have shown varying compliance rates among different healthcare professional groups. For instance, a study conducted in a tertiary care hospital in Northern India reported that compliance rates were generally higher among nursing staff compared to medical staff, reflecting the critical role nurses play in direct patient care and adherence to safety protocols [30]. Another study highlighted that junior medical staff often had lower compliance rates, possibly due to their relative inexperience and the high demands of their roles [30]. Combining data from these studies with your findings can provide a comprehensive understanding of IPSG adherence across different healthcare professional groups.
Table 18: Our study revealed significant disparities across different cadres, with Senior Residents (SR) exhibiting a 12% positive gap, Junior Residents (JR) a 16% positive gap, and Senior Nursing Officers (SNO) a 15% positive gap, indicating that these groups possess greater knowledge than what is demonstrated in their practice. In contrast, Nursing Officers (NO) presented a -3% negative gap, suggesting that their practice scores slightly surpass their knowledge scores, likely due to the compensatory effect of practical experience. Joshi DC, et al. [23] study in a tertiary care hospital in Northern India found that while 85% of healthcare workers had good knowledge of IPSG, only 60% adhered to these practices, with barriers such as lack of training and inadequate resources [23]. Similarly, Ananya R, et al. [24] research in a tertiary care cardiac centre in India showed that 78% of healthcare workers were knowledgeable about IPSG, but only 55% consistently adhered to these practices, with high workload and insufficient staffing identified as major barriers [24]. These combined findings underscore the necessity for tailored strategies to bridge the knowledge-practice gap. Addressing these barriers through targeted interventions, such as continuous training, practical workshops, improved resource allocation, and supportive supervision, is crucial. Enhancing the practical application of knowledge among SRs, JRs, and SNOs, while leveraging the practical experience of NOs, could significantly improve adherence to IPSG and overall patient safety.
Conclusion
Overall, the knowledge and practice compliance rates among healthcare workers in the institute are moderate. Nursing Officers (NOs) demonstrate comparatively higher compliance rates in both IPSG practices and knowledge than Senior Residents (SRs), Junior Residents (JRs), and Senior Nursing Officers (SNOs). Specifically, the compliance rates for IPSG practices and knowledge are notably lower among JRs, indicating a significant area for improvement.
The gap analysis revealed a positive gap of 12%, 15%, and 16% among SRs, JRs, and SNOs, respectively. This positive gap indicates that these groups possess greater knowledge than what is demonstrated in their practice, suggesting the presence of barriers that prevent the effective translation of knowledge into practice. On the other hand, the negative gap of -3% among NOs indicates that their practice compliance slightly surpasses their knowledge, likely due to the compensatory effect of practical experience.
These findings underscore the necessity for targeted interventions to bridge the knowledge-practice gap. There is a clear need to enhance both the knowledge and practice compliance rates among healthcare workers, particularly among SRs, JRs, and SNOs. Strategies such as continuous training, practical workshops, improved resource allocation, and supportive supervision could be instrumental in addressing these gaps. By focusing on these areas, we can significantly improve adherence to IPSG and overall patient safety in our institute.
Recommendations
Overall, the knowledge and practice compliance rates among healthcare workers were moderate. To improve these rates, it is recommended to implement induction and continuous training programs focused on adherence to IPSG practices. Such training can enhance both knowledge and practical application among healthcare workers.
Additionally, conducting continuous audits and providing regular feedback can help identify and address gaps in practice.
Implementing accreditation standards such as those from NABH and Kayakalp can further improve adherence to IPSG practices among healthcare workers.
These strategies collectively can lead to significant improvements in patient safety and care quality.
Limitations
- The study participants were limited to specific cadres, which may impact the generalizability of the findings.
- Additionally, there were fewer surgical opportunities, making it challenging to appropriately assess Goal 4. As our institute is in its early stages, the number of opportunities for observation was limited to specific goal practices.
- Furthermore, the study was conducted in a single healthcare facility, which might limit the generalizability of the findings to other settings.
- There may be other factors influencing the knowledge- practice gap that were not measured in this study, such as insufficient training resources, varying levels of individual motivation, and differences in departmental policies.
Future Scope
The limited surgical opportunities, reflective of the institute’s early-stage development, posed challenges in effectively assessing Goal 4 compliance. However, these constraints are characteristic of emerging healthcare settings and underscore the need for tailored approaches. Despite these limitations, the study provides meaningful insights into IPSG practices and highlights areas for improvement. Future research could address these gaps by exploring longer study durations or leveraging collaborations with established institutions to enhance the scope and applicability of findings.
References
-
(2020) The Joint Commission. Patient Safety.
-
Emanuel L, Berwick D, Conway J(2008) What Exactly Is Patient Safety?. In: Henriksen K, Battles JB, et al. (Eds.), Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 1: Assessment). Rockville (MD): Agency for Healthcare Research and Quality.
-
(2020) Focusing on the International Patient Safety Goals.
-
(2024) Patient Safety.
-
(2020) World Health Organization.
-
Panattieri ND, Dackiewicz N, Arpí L, Godio C, Andión E, et al. (2019) Patient safety and the international goals: Consensus document. Arch Argent Pediatr 117(S6): S277-309.
-
(2020) Quality Management and Patient Safety.
-
Geberemariyam BS, Donka GM, Wordofa B (2018) Assessment of knowledge and practices of healthcare workers towards infection prevention and associated factors in healthcare facilities of West Arsi District, Southeast Ethiopia: a facility-based cross-sectional study. Arch Public Health 76: 69.
-
Joint Commission International (2023) International Patient Safety Goals
-
Joint Commission International (2020) International Patient Safety Goals. In: 6th (Edn.).
-
National Accreditation Board for Hospitals & Healthcare Providers (NABH) (2021) NABH Newsletter.
-
National Health Authority (2021) Ayushman Bharat Digital Mission.
-
Abousallah A (2018) The Impact of Application of International Safety Goals on Patient Safety Culture: A Field Study in Private Hospitals in Amman.
-
World Health Organization (2024) Global Patient Safety Report 2024.
-
World Health Organization (2023) Patient safety.
-
The impact of patient identification errors (2021).
-
Douglass K, Narayan L, Allen R, Pandya J, Talib Z (2021) Language diversity and challenges to communication in Indian emergency departments. Int J Emerg Med 14(1): 57.
-
MacDowell P, Cabri A, Davis M (2021) Medication administration errors. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services.
-
Kentucky Trial Lawyers (2023) How often do surgical errors occur?.
-
World Health Organization (2024) Safe surgery.
-
Wang Y, Leng S, Jin Y, Tang X, Zhu X, et al (2024) Successful ageing is associated with falls among older adults in India: a large population-based cross-sectional study based on LASI. BMC Public Health 24: 1682.
-
Salari N, Darvishi N, Ahmadipanah M, Shohaimi S, Mohammadi M (2022) Global prevalence of falls in the older adults: a comprehensive systematic review and meta-analysis. J Orthop Surg Res 17: 334.
-
Chandra Joshi D, Ravinder Singh S (2022) Awareness and Compliance to International Patient Safety Goals among Healthcare Personnel of a Tertiary Care Hospital in Northern India. Journal of Clinical and Diagnostic Research.
-
Ananya R, Kamath S, Pati A, Sharma A, Raj A, et al. (2019) A Study on Adherence to International Patient Safety Goals in a Tertiary Care Cardiac Centre in India. Medicolegal update 19(2): 211.
-
Raghavendran M, Batacharjee T, Revathi R (2020) A Study to Assess the Knowledge, Attitude and Practice Regarding International Patient Safety Goals Among the Staff Nurses at Selected Hospital, Kanpur. International Journal of Pharmacy and Biological Sciences.
-
Abousallah A (2018) The impact of application of international safety goals on patient safety culture: A field study in private hospitals that working in the city of Amman. MEU library Theses: Middle East University.
-
Swaris M, Mamatha HK (2022) A Study on Patient Safety Practice Compliance in a Tertiary Care Teaching Hospital. International Journal of Health Sciences and Research.
-
Akhu-Zaheya LM, Khater WA, Shaban IA (2020) The effectiveness of training programs in improving the knowledge and practice of International Patient Safety Goals (IPSGs) among nurses in Jordanian hospitals. J Nurse Care Qual 35(3): E1-E7.
-
Sameera V, Bindra A, Rath GP (2021) Human errors and their prevention in healthcare. J Anaesthesiol Clin Pharmacol 37(3): 328-335.
-
Shahin MAH, Alshammari RK, Alabed HH (2020) Quality of care and patients’ safety awareness and compliance among critical care nurses at Qassim National Hospital: adopting IPSGs.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report
- A Single-Center, Prospective Study Focused on Quality Indicators, Success Rate, Features, Outcomes, and Indications of Endoscopic Retrograde Cholangiopancreatography (ECRP) Practice at a Tertiary Care Hospital