Prognostic Factors of Cervical Cord Injury
Aim: Identify prognostic factors of management of cervical spinal cord injury in a low income country. Patients and method: This was a retrospective descriptive study which took place over 4 years and half, from 1st January 2010 to 30 June 2014. A correlation with statistical test has been searched between different variables: sex and clinical evolution, age and clinical evolution, injury circumstances and neurological achievement, admission delay and clinical evolution, operative delay and clinical evolution, tetraplegia and clinical evolution, sphincter disorders and clinical evolution. Epi-info version 3. 5. 1. has been used for statistical tests. Results: Women had clinical improvement in 72.7% and men in 56.5% with a statistically not significant difference (p=0.6053). Patients under 49 years old had a clinical improvement in more than 50% while patients of 50-59 years old have all presented an improvement with a statistically not significant difference (p=0.3665). 4 patients among 7 (57.1%) with a neurological improvement were victims of a public highway accident and 3 patients (42.9%) of work accident with a statistically not significant difference (p=0.4567). A clinical improvement was obtained in more than 50% of patients whatever is the admission delay with a statistically not significant difference (p= 0.4321). Clinical improvement concerned 15 patients (75%) among 20 patients with surgical management after 48 hours with a statistically significant difference (0.0029). 53.8% of patients with incomplete tetraplegia had a clinically improvement with a statistically significant difference (p=0.0378). Clinical improvement was achieved in 68.8% of patients without sphincter disorders against 48% in patients with sphincter disorders. Difference was statistically significant (p=0.0083) Conclusion: At the end of this study, there is a significant clinical improvement in patients with surgical management after 48 years, in patients with incomplete tetraplegia and patients without sphincter disorders.
Introduction
Cervical cord injuries are osseous disc and ligamentous injuries located on cervical cord segment. They represent 2 to 3% of all injuries [1, 2]. Prognostic is linked to initial medullar achievement and time of management [3]. The aim of this study was to identify prognostic factors of management of cervical cord injuries in a low income country.
Patients and Method
Patients
Fifty-seven medical files of patients have been registered. Average age of patients was 38.7 years with extremes of 19 years and 71 years. It was about 46 men and 11 women with a sex-ratio of 4.2. Etiology was dominated by public highway accident in 41 cases (72%). Average admission delay was 27.5 days with extremes of 3 hours and 175 days. Among 25 patients evaluated with ASIA score, 20 patients (80%) were ASIA A or B. forty- eight patients (84.2%) had a motor deficit. Thirty-two patients (56.1%) had tetraplegia, 7 patients (12.3%) with neurovegetatives disorders. Twenty-five patients (43.9%) had sphincter disorders. Among 50 cord injuries, inferior cervical cord was involved in 41 cases (82%), superior cervical cord in 4 cases (8%) and twice achievement in 5 cases (10%). Among 24 vertebral injuries, C4-C5 level was injured in 9 cases (37.5%) followed by C5-C6 level injury in 8 cases (33.3%). According to injuries, there was 16 fractures cases, 15 dislocations cases, 1 fractures- dislocations case, 5 sprains cases, 2 post traumatic disc hernia cases, 1 fracture-compression case.
Management was orthopedic in 54.4% and surgical in 42.1%. Average surgical delay was 25 days with extremes of 24 hours and 101 days. Anterior surgical way was used in 95.83%. Arthrodesis with autologous graft associated to osteosynthesis with screwed plate was most used in 54.16%. Infection occurred in 2 cases (4.08%). Complications of decubitus occurred in Twenty-five patients (51.02%): eschars in 21 cases (42.85%) and pneumonia in 4 cases (8.16%). Mortality occurred in 28.57%. Average hospitalization delay was 39.4 days.
Method
It was about a retrospective descriptive study which took place on 4 years and half, from 1st January 2010 to 30th June 2014. The injuries needed surgical procedure was achieved by a team of three surgeons. A correlation with statistical test has been searched between different variables: sex and clinical evolution, age and clinical evolution, injury circumstances and neurological achievement, admission delay and clinical evolution, operative delay and clinical evolution, tetraplegia and clinical evolution, sphincter disorders and clinical evolution. Epi-info version 3.5.1. Has been used for statistical tests. Chi-squared test was significant for a p value inferior to 0.05.
Results
Clinical improvement was obtained in women in 72.7% against 56.5% in men. A clinical worsening was obtained in men in 26.1% against 18.2% in women with a statistically not significant difference (p=0,6053). This is shown by figure 1.
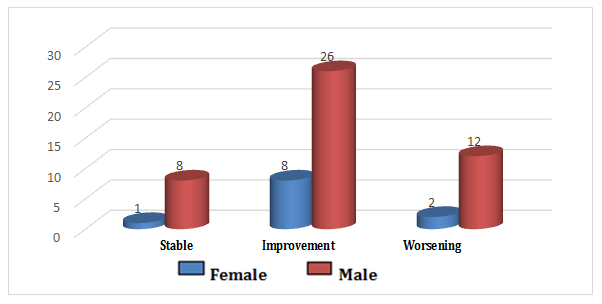
X2 =1,0041 p= 0,6053 Figure 1: Distribution according to clinical outcome and sex.
| Stable | Improvement | Worsening | Total | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number | % | Number | % | Number | % | Number | % | |||||||||
| <30years | 4 | 7, 01 | 10 | 17,54 | 4 | 7,01 | 18 | 31,6 | ||||||||
| 30-39 years | 2 | 3,50 | 10 | 17,54 | 7 | 12,28 | 19 | 33,3 | ||||||||
| 40- 49 years | 1 | 1,75 | 6 | 10,52 | 2 | 3,50 | 9 | 15,8 | ||||||||
| 50-59 years | 0 | 0 | 6 | 10,52 | 0 | 0 | 6 | 10,5 | ||||||||
| > 60 years | 2 | 3,50 | 2 | 3,50 | 1 | 1,75 | 5 | 8,8 | ||||||||
| Total | 9 | 15,76 | 34 | 59,62 | 14 | 24,54 | 57 | 100 |
Table 1: Distribution of clinical outcome according to tetraplegia. Clinical worsening concerned 83.3% of patient’s complete tetr
Clinical worsening was seen in patients between 30-39 years old in 36.8%. Patients under 49 years olds had clinical improvement in more than 50% while patients
| Neurological | WA | TRA | Others | Total | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Disorders | Number | % | Number | % | Number | % | Number | % | |||||||
| NO | 10 | 20 | 37 | 74 | 3 | 6 | 50 | 100,0 | |||||||
| YES | 3 | 42,9 | 4 | 57,1 | 0 | 0 | 7 | 100,0 | |||||||
| Total |
Table 2: Distribution of clinical outcome according to tetraplegia. Clinical worsening concerned 83.3% of patient’s complete tetr
Fifty patients didn’t present neurological achievement. Thirty-seven patients (74%) among them were victim of traffic road accident. Four patients among 7 (57.1%) with neurological achievement were victim of traffic road accident and 3 patients (42.9%) victim of work accident. Difference was statistically not significant (p=0.4567).
Table 2 shows this distribution. Clinical outcome was favorable with improvement in more than 50% whatever the admission delay. Difference was statistically not significant (p= 0.4321).
| Stable | Improvement | Worsening | Total | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number | % | Number | % | Number | % | Number | % | |||||||||
| < 24h | 5 | 17,9 | 15 | 53,6 | 8 | 28,6 | 28 | 100,0 | ||||||||
| 24 - 48 H | 3 | 23,1 | 9 | 69,2 | 1 | 7,7 | 13 | 100,0 | ||||||||
| > 48 H | 1 | 6,3 | 10 | 62,5 | 5 | 31,3 | 16 | 100,0 |
Table 3: Distribution of clinical outcome according to tetraplegia. Clinical worsening concerned 83.3% of patient’s complete tetr
| Stable | Improvement | Worsening | Total | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number | % | Number | % | Number | % | Number | % | |||||||
| 24H - 48H | 0 | 0 | 0 | 0 | 4 | 100 | 4 | 100,0 | ||||||
| > 48 H | 2 | 10 | 15 | 75 | 3 | 15 | 20 | 100,0 |
Table 4: Distribution of clinical outcome according to tetraplegia. Clinical worsening concerned 83.3% of patient’s complete tetr
after 48 hours. Difference was statistically significant (p=0.0029).
| Stable | Improvement | Worsening | TOTAL | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tetraplegia | Number | % | Number | % | Number | % | Number | % | ||||||||
| Complete | 1 | 16,7 | 0 | 0 | 5 | 83,3 | 6 | |||||||||
| Incomplet | 4 | 15,4 | 14 | 53,8 | 8 | 30,8 | 26 |
Table 5: Distribution of clinical outcome according to tetraplegia. Clinical worsening concerned 83.3% of patient’s complete tetr
X2=-,5515 p= 0,0378 Table 5: Distribution of clinical outcome according to tetraplegia. Clinical worsening concerned 83.3% of patient’s complete tetraplegia at admission. Clinical improvement occurred in 53.8% of patients with incomplete $$ \text{tetraplegia. Difference was statistically significant} (p=0.0378). $$
| Worsening | Improvement | Stable | TOTAL | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number | % | Number | % | Number | % | ||||||||||
| Sphincter disorders | 57 | ||||||||||||||
| NO | 3 | 9,4 | 22 | 68,8 | 7 | 21,9 | 32 | ||||||||
| YES | 11 | 44 | 12 | 48 | 2 | 8 | 25 |
Discussion
Cervical cord trauma is a public health problem in low income country because its concerns a young and active population [3, 4]. We have included in this study all cervical cord traumatism with or without neurological injuries with aim to study prognostic factors for clinical outcome. According to sex, clinical improvement was better in women (72.7%) than men (56.5%) and clinical worsening was more frequent in men (26.1%) than in women (18.2%). Women in general, more cautious and less exposed to risk situations as men have certainly less severe attacks. However, difference was not statistically significant (p=0.6053). This result must be qualified. Indeed, under the term cervical cord traumatism is grouped different injuries as well benign as of various gravity without same prognostic.
We have noted absence of statistically significant difference for clinical improvement according to age (p=0.3665). However, more detailed analysis has permit to evoke that a certain clinical improvement with age with 100% in patients between 50 to 59 years. How could we explain this result? Could we advance hypothesis that most severe Injuries with high energy traumatism occur in more young population with clinical improvement according to age? Would the fall in the improvement of Clinical condition at 40% in patients over 60 years not be related to medical history? There are also different injuries in our study which not needed all surgical management. There is no statistically significant difference between circumstances and neurological disorders (p=0.4567). All kind of circumstance can lead to occurrence or not of neurological disorders. It didn’t exist statistically significant difference between admission delay and clinical outcome (p=0.4321). However, clinical improvement was better in patients with admission in the first 24 to 48 hours (69.2%) and clinical worsening was the least in these patients (7.7%). Fehlings et al. [5] have shown that a better neurological recovery at 6 months was linked to surgical management within the first 24 hours after the traumatism. For
Edouard [6], ideal operative time would be 6 hours to 8 hours. In our study, preoperative delay was 25 days. It is 5.37 days in Senegal [3]. This delay is linked to admission delay which is approximatively 10 hours in South Africa [7] and 2.5 days in Nigeria [8]. Several factors can explain this result. We have distance of public health center from population, low financial ressources, patient transport not done by qualified men (firefighters and ambulance) and emergency management system failure with late admission to referral centers [8, 9].
Conclusion
At the end of this study, even our study size is very small; there is a significant clinical improvement in patients with surgical management after 48 years olds. Also, we can conclude in general for this result. Another study with a big sample size will be necessary to conclude. We have also found clinical improvement in patients with incomplet tetraplegia and patients without sphincter disorders.
References
-
Gerbeaux P, Portier F (2003) Stratégies d’imageries des traumatismes du rachis cervical. Presse Med 32: 1853-1856.
-
Berne JD, Velmahos GC, El Tawil Q, Demetriades D, Asensio JA, et al. (1999) Value of complete cervical helical computed tomographic scanning in identifying cervical spine injury in the unevaluable blunt trauma patient with multiple injuries: a prospective study. J Trauma 47(5): 896-903.
-
Kpelao E, Diop A, Beketi K, Tine I, Thioub M, et al. (2013) Problématique de la prise en charge des traumatismes graves du rachis cervical en pays sous- développé. Neurochirurgie 59(3): 111-114.
-
Kawu K, Adebule GT, Gbadegesin AA, Alimi MF, Salami AO (2010) Outcome of conservative treatment of spinal cord injuries in Lagos, Nigeria. Niger J Orthop Trauma 9(1): 21-23.
-
Fehlings MG, Vaccaro A, Wilson JR, Singh A, Cadotte DW, et al. (2012) Early versus delayed decompression for traumatic cervical spinal cord injury: results of the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS). PLoS One 7(2): e32037
-
Edouard A (2003) Prise en charge d’un blessé adulte présentant un traumatisme vertébro-médullaire.
-
Dunn RN, van der Spuy D (2010) Rugby and cervical spine injuries - has anything changed? A 5-year review in the Western Cape. S Afr Med J 100(4): 235- 238.
-
Babatunde AS (2002) Spinal cord injuries in Ilorin, Nigeria. West Afr J Med 21(3): 230-232.
-
Ahidjo KA, Olayinka SA, Ayokunle O, Mustapha AF, Sulaiman GAA et al. (2011) Prehospital transport of patients with spinal cord injury in Nigeria. J Spinal Cord Med 34(3): 308-311.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results