Compressive Mass of the Thearloop Revealing an Intramuscular Lipoma of the Short Abductor of the Thumb (A Case Report)
The lipoma of the thear louse is a rare lesion, which is often expressed by a tumor syndrome and signs of compression of the branches of the median nerve. Magnetic resonance imaging is the exam of choice to study the local extension of the tumor. The main differential diagnoses are median nerve lipofibroma and low grade liposarcoma.
Introduction
The benign tumor pathologies of the hand are frequent and mainly represented by arthro-synovial and paratendinous cysts. Other etiologies are more rare: among these, lipomas constitute only 1 to 3.8% [1, 2] of benign tumors of the hand. The location at the Thear Lodge is exceptional. We present here the case of a patient who presented a compressive lipoma of the lateral branches of the median nerve at the level of the thear lodge.
Observation
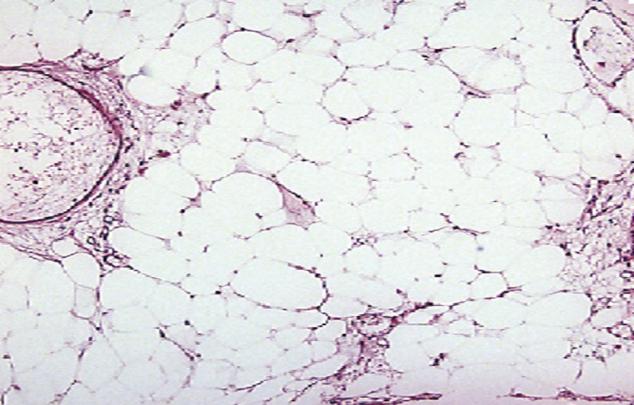
Mr E.L., aged 37, a right-handed man with no particular pathological history, consulted for paresthesias in the thumb right, present for a year and a half increasing for two months. The clinical examination found a very limited swelling, soft, non-inflammatory and painless in the thear lodge, with paresthésies at the outer edge of the thumb. The Allen test was normal, indicating good permeability of the radial artery. The standard radio graph did not reveal a pathological image. The electro myogram (EMG) and the measurement of nerve conduction noted in the right thumb a sustained sensory latency in the distribution area of the lateral branches of the median nerve. Magnetic resonance imaging monitored a hypersignal image in T2 after injection of gadolenium (Figure 1). A biopsy resection was performed under locoregional anesthesia and pneumatic tourniquet at the root of the limb, a tumor-centered approach allowed us to demonstrate an intra muscular mass of lipomatous appearance occupying the short abductor muscle of the thumb with close contact with the lateral rami of the median nerve. The encapsulated tumor was cautiously dissected. The size of the Tumor after resection was 4.5 cm in diameter (Figure 2). The histological study of the surgical specimen confirmed the diagnosis of lipoma (Figure 3).
The evolution was marked by the resolution of the sensory disturbances. At 10 months of follow-up, there was no recurrence of the tumor or nervous disorder.





Discussion
Lipomais a benign tumor, with a clean wall, sometimes polylobed, well encapsulated, developed from mature adipocyte cells. It is often painless and usually results in the palpation of a soft, regular and mobile tumor. In the hand, it is above all the appearance of signs of vasculo- cereal compression which leads the patient to consult. According to its localization, the lipoma can induce nerve compressions, ductal syndrome [3, 4, 5, 6, 7, 8, 9, 10], compression of the digital nerves [5], or even a finger with a jump [7]. The localization at the thear lodge remains unusual and exceptional, such as the case of our patient. Signs of nerve compression are not correlated with the size of the tumor in intranasally developed forms, as opposed to extranor forms for which volume definitely has a role. In the series consulted, compression of the branches of the median nerve was sometimes observed for small tumors. Nerve compression in these cases was explained by the intraoperative discovery of a tumor adherent to the nerve or, A tumor traversed by the nerve branches [6]. In the present case, the tumor was intra muscular and adherent to the lateral rami of the median nerve.
Among the complementary means of exploration of modern imaging ; Ultra sound always retains its place in some authors [6, 7, 10] because it first allows us to differentiate a lipoma from a liposarcoma according to its location and its echogenicity: lipomas are mostly limited without a vascularized zone, their echo structure is similar to that of subcutaneous fat, with an aspect of lobules separated by hyperechoiclinear interfaces, whereas liposarcoma, which is a hard mass, is often deep and poorly limited [3]. But the magnetic resonance imaging remains the most reliable examination, because of its high sensitivity, is an interesting addition to the diagnostic orientation [11], it would show a lobulated mass appearance, including Septas with a hyper signal aspect in T1 and iso signal in T2-weighted sequence, it also allows to make a preoperative planning by studying the dimensions, the ratios, the limits of the tumor and would then orient the route of the surgical approach, with less risk of iatrogenic vascular or nerve damage. At the level of the hand, marginal excision is the treatment of choice of benign lipomas. Dissection and identification of vasculonuclear elements should be carefully considered to avoid iatrogenic lesions. Local recurrences are exceptional. Liposarcoma is the main differential diagnosis.
Conclusion
The lipoma of the thear lodge remains an exceptional localization of the tumor. The presence of signs of nerve compression imposes a well-established etiological balance. The histology after complete removal of the tumor remains imperative to confirm the diagnosis and eliminate a malignant tumor, in particular a liposarcoma.
References
-
Bogumill GP, Sullivan DJ, Baker GL (1975) Tumors of the hand. Clin Orthop 108: 214-222.
-
Leung PC (1981) Tumors of hand. The Hand 13: 169-
-
De Smet L, Bande S, Fabry G (1994) Giant lipoma of the deep palmar space, mimicking persistent carpal tunnel syndrome Acta Orthop Belg 60(3): 334-335.
-
Hoehn JG, Farber HF (1983) Massive lipoma of the palm. Ann Plast Surg 11(5):431-433.
-
Boussouga M, Bousselmame N, Lazrak KH (2006) Lipome compressif de la loge thénar. À propos d’une observation. Chir Main 25: 156-158.
-
Cribb GL, Cool WP, Ford DJ, Mangham DC (2005) Giant lipomateus of the hand and forearm. Br J Hand Surg 30(5): 509-512.
-
Brand MG, Gelberman RH (1988) Lipoma of the flexor digitorum superficialis causing triggering at the carpal canal and median nerve compression.13(3): 342-344.
-
Hironori S, Mitsuhiro T, Hirofumi T, Tsutomu H, Hiroshi T (2002) Carpal tunnel syndrome and trigger wrist caused by a lipoma arising from flexor tenosynovium: a case report. J Hand Surg 27A(6): 1056-1058.
-
Fnini S, Hassoune J, Garche A, Rahmi M, Largab A (2010) Lipome géant de la main : présentation d’un cas clinique et revue de la littérature. Chir Main 29: 44-47.
-
Zahrawi F (1984) Acute compression ulnar neuropathy at Guyon’s canal resulting from lipoma. J Hand Surg 9(2): 238-239.
-
Peh WC, Truong NP, Totty WG, Gilula L (1995) Magnetic resonance imaging of benign soft tissue masses of the hand and wrist. Clin Radiol 50(8): 519- 525.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results