Outcomes and Complications of Intertrochanteric Fractures Treated with Trochanteric Fixation Nail: A Study of 138 Patients
Background: The aim of this prospective study was to evaluate outcomes and complications of patients with intertrochanteric fractures treated with trochanteric fixation nail. Materials and Methods: 138 patients with intertrochanteric fractures were treated with trochanteric fixation nail from June 2011 to May 2014. There were 80 male patients and 58 females. There were 70 cases of AO type 31-A1 fractures, 32 fractures were type 31-A2 and 36 cases were type 31-A3. Union time, union rate, time to weight bearing, complications was recorded. The overall patient outcomes were summarized based on the Harris Hip Scoring system. Results: Average time needed to do TFN fixation was 48.2 ± 10.2 minutes (range 39-74 minutes). Per-operative blood loss was 150 ± 74 ml (range 80-300 ml). Of the 138 patients, 125 patients achieved union uneventfully. The mean union time was 4.4 ± 1.3 months (range 3-7months). Nonunion occurred in 13 cases. Conclusions: For intertrochanteric fractures fixation, trochanteric fixation nail is an effective implant in providing early mobilisation and weight bearing with comparable complication rate.
Introduction
Intertrochanteric fractures occur predominantly as low-energy injuries in elderly patients and as high-energy injuries in younger patients [1, 2]. The prevalence of these fractures is increasing with increase in the life expectancy [3]. Various internal fixation devices have been used for surgical fixation of intertrochanteric femur fractures, and they can be categorized into extramedullary fixation devices and intramedullary fixation devices [4]. Excessive sliding of the lag screw within the plate barrel results in limb shortening and medialization of the distal fragment, which is main cause behind failure of extramedullary devices like Dynamic Hip Screw (DHS) [5, 6]. The various intramedullary devices available are enders nail (condylocephalic nail) and cephalomedullay nails like, proximal femoral nail (PFN), trochanteric fixation nail (TFN), gamma nail, intramedullary hip screw, trochanteric antigrade nail [7, 8].
These nails offer several potential advantages. Because of its central location and the shorter lever arm, intramedullary nail can be expected to decrease tensile strain on the implant decreasing the risk of implant failure and providing more efficient load transfer with maintaining the advantage of controlled fracture impaction as in DHS [9, 10]. The trochanteric femoral nail (TFN) was developed to improve the rotational stability of the proximal fracture fragment, combining the features of an undreamed intramedullary femoral nail with a sliding, load-bearing, femoral neck screw and to avoid curves of femur diaphysis posing difficulty in nail insertion. This prospective study was performed to evaluate outcomes and complications of IT fractures treated with TFN.
Materials and Methods
This prospective study was approved by institutional review board and authorized by the local ethical committee. It was performed in accordance with the Ethical standards of the 1964 Declaration of Helsinki as revised in 2000. During three years, from June 2011 to May 2014, 150 patients with unilateral closed IT fractures were treated with internal fixation with TFN in our hospital. Of the 150 patients, 12 patients were lost to follow-up. Inclusion criteria:
• Unilateral, closed IT fractures.
• Age > 18 years
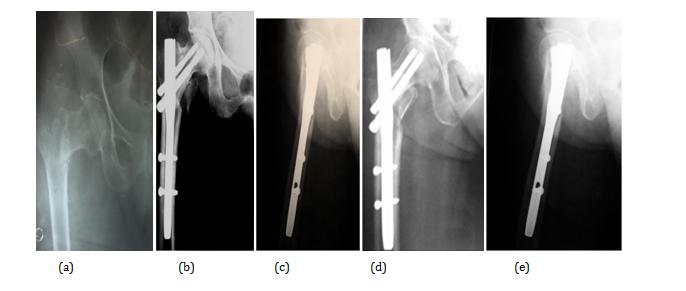
IT fractures with extension below lesser trochanter, patients with previous surgery of the proximal femur, ongoing chemotherapy or irradiation treatment, pathological fractures and open fractures were not included in this study. Other than the demographic details, information concerning the operative time, duration, amount of blood loss, time to full-weight- bearing were recorded. The average age in this study was 68.6 ± 5.6 years (range, 19-82 years). The fractures were classified according to AO/OTA classification. All patients were evaluated preoperatively with use of two standard plain radiographs, an anterioroposterior (AP), and a lateral views. Patients were operated upon as soon as their general medical condition allowed. Surgery was performed with the patient in supine position on a fracture table in traction using lateral approach. TFN with two femoral neck screws was used in these cases Standard postoperative protocol was followed. Knee and ankle exercises were started on postoperative day one. Non weight-bearing walking with help of walker or crutces was started after surgery usually on the third to fifth postoperative day as tolerated by patients. Follow up was done at monthly interval for first 3 months then at 3- months interval for next 15 months (total 18 months). At each follow up, patients were assessed clinicoradiologically. Local wound site, pain, functional outcome scores and complications were assessed and reported. AP and lateral X-ray views were taken at each follow- up and looked for implant position along with signs of fracture union. All patients were advised partial weight bearing with a walker for a period of six to eight weeks then walking with gradually increasing weight bearing was allowed to the patients provided that reduced and stabilized fracture position stayed unchanged and clinicoradiological signs of bone healing (no pain, swelling, tenderness at fracture site clinically and invisible fracture lines in x-rays) allowed. The overall patient outcomes were summarized based on the Harris Hip Scoring system [11] with excellent defined as 90–100 points, good as 80–89 points, fair as 70–79 points, and poor as <70 points. The complications were evaluated in terms of infections (superficial or deep), non-union, implant failure (implant breakage, screw cut-out, Z-effect), secondary loss of reduction, complications unrelated to implant (DVT, bed sores, chest infections etc). Fractures were said to be healed radio graphically if bridging callus was evident on three of four cortices as seen on two views Figure 1.
Results
There were 80 male patients and 58 females. There were 70 cases of AO type 31-A1 fractures, 32 fractures were type 31-A2 and 36 cases were type 31-A3. Average time needed to do TFN fixation was 48.2 ± 10.2 minutes (range 39-74 minutes). Per-operative blood loss was 150 ± 74 ml (range 80-300). Of the 138 patients, 125 patients achieved union uneventfully. The mean union time was 4.4 ± 1.3 months (range 3-7months). 8 cases developed superficial infection but infection was controlled by oral antibiotics in all this case. There was no incidence of deep infection. Nonunion occurred in 13 cases. Four cases with nonunion also had broken neck screws, without any history of fresh trauma and 9 cases of nonunion had Z- effect (back out of one lag screw). All 13 cases of nonunion had undergone revision surgery. The prevalence of postoperative complications unrelated to fracture, such as chest infections, bed sore, urinary tract infection , deep venous thrombosis was comparable with other studies.
To measure functional outcomes, HHS was assessed at each follow-up visit and final follow-up visit showed higher HHS in our study (82.8 ± 12.4; range 66-92).
Discussions
The aim of management of proximal femoral fractures is to achieve near anatomical reduction with a stable fracture fixation. Outcomes of treatment of intertrochanteric fractures depend on bone quality, age of patient, general health, comorbidities and stability of fixation along with choice of implant [12]. Over the years, both intramedullary and extramedullary devices has been used in management of intertrochanteric fractures but each has its own merits and demerits [13, 14]. IT fractures treated with extramedullary devices such as dynamic hip screw or dynamic condylar screw has been shown to develop complications like limb shortening and medialization of the distal fragment [15, 16]. Varus collapse and implant failure such as cut-out of the femoral head screw have also been reported frequently [13, 17]. This has led to the development of intramedullary hip screw devices such as PFN and TFN, which has several potential advantages like shorter lever arm decreasing tensile strain on the implant and efficient load transfer capacity. Some studies have shown cases treated with PFN developing intra-operative complications such as splintering and Fractures at tip of nail due to increased bowing of the anterior cortex of the femur [18]. In our study, there was no incidence of intraoperative shaft fracture. Average operative time, union time, union rate was also comparable to other studies in literature [19, 20]. The main drawback of TFN was unsuitability of this implant to be used in IT fracture extended below the lesser trochanter. In these cases, PFN provides more stability. Regarding functional outcomes, Harris hip scores were good in our study and comparable with other studies at final follow-up [20]. To further evaluate outcome of TFN in IT fractures large multicentre trials are needed and comparative studies to be done with fracture fixation with other implants. For intertrochanteric fractures fixation intramedullary nailing has shown to be effective in providing early mobilization and weight bearing. When the fracture does not extend below the lesser trochanter, TFN is as effective as PFN avoiding impingement on femoral cortex and impending fractures.
References
-
Cummings Steven R, Rubin Susan M, Black Dennis (1990) Costs and potential effects of postmenopausal estrogen. Clincal Orthopedics 252: 163-166.
-
Kyle RF (1994) Instructional course lectures, the academy of orthopedic surgeons: Fractures of the proximal part of the femur. J Bone Joint Surg 76(A): 924-950.
-
Zain Elabdien B, Olerud S, Karlstrom G, Smedby B (1984) Rising incidence of hip fracture in Uppsala, 1965-1980. Acta Orthop Scand 55(3): 284-289.
-
Kokoroghiannis, Aktselis I, Deligeorgis A, Fragkomichalos E, Papadimas D, et al. (2012) Evolving concepts of stability and intramedullary fixation of intertrochanteric fractures-A review. Injury 43(6): 686-693.
-
Rha JD, Kim YH, Yoon SI, Park TS, Lee MH (1993) Factors affecting sliding of the lag screw in intertrochanteric fractures. Int Orthop 17(5): 320- 324.
-
Baixauli F, Vincent V, Baixauli E, Serra V, Sánchez- Alepuz E, et al. (1999) A reinforced rigid fixation device for unstable intertrochanteric fractures. Clin Orthop Relat Res (361): 205-215.
-
Harrington P, Nihal A, Singhania AK, Howell FR (2002) Intramedullary hip screw versus sliding hip screw for unstable intertrochanteric femoral fractures in the elderly. Injury 33(1): 23-28.
-
Parker M, Handoll HH (2008) Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures in adults. . Cochrane Database Syst Rev 16(3): CD93.
-
Pryce Lewis JR, Ashcroft GP (2007) Reverse LISS plating for proximal segmental femoral fractures in the polytrauma patient: a case report. Injury 38(2): 235-239.
-
Zha GC, Chen ZL, Qi XB, Sun JY (2011) Treatment of pertrochanteric fractures with a proximal femur locking compression plate. Injury 42(11): 1294-1299.
-
Harris WH (1969) Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. Journal of Bone and Joint Surgery 51(4): 737-755.
-
Dahl E (1980) Mortality and life expectancy after hip fractures. Acta Orthop Scand 51(1): 163-170.
-
Sadowski C, Lübbeke A, Saudan M, Riand N, Stern R, et al. (2002) Treatment of reverse oblique and transverse intertrochanteric fractures with use of an intramedullary nail or a 95 degrees screw-plate: a prospective, randomized study. J Bone Joint Surg Am 84: 372-381.
-
Suckel AA, Dietz K, Wuelker N, Helwig P (2006) Evaluation of complications of three different types of proximal extra-articular femur fractures: Differences in complications, age, sex and surviving rates. Int Orthop 31(5): 689-695.
-
Nuber S, Schonweiss T, Ruter A (2003) Stabilisation of unstable trochanteric femoral fractures. Dynamic hip screw (DHS) with trochanteric stabilisation plate vs proximal femur nail (PFN). Unfallchirurg 106(1): 39-47.
-
Klinger HM, Baums MH, Eckert M, Neugebauer R (2005) A comparative study of unstable per- and intertrochanteric femoral fractures treated with dynamic hip screw (DHS) and trochanteric butt-press plate vs. proximal femoral nail (PFN). Zentralbl Chir 130(4): 301-306.
-
Bridle SH, Patel AD, Bircher M, Calvert PT (1991) Fixation of intertrochanteric fractures of the femur. A randomised prospective comparison of the gamma nail and the dynamic hip screw. J Bone Joint Surg Br 73(2): 330-334.
-
Egol KA, Chang EY, Cvitkovic J, Kummer FJ, Koval KJ (2004) Mismatch of current intramedullary nails with the anterior bow of the femur. J OrthopTrauma 18(7): 410-415.
-
Utrilla AL, Reig JS, Muñoz FM, Tufanisco CB (2005) Trochanteric gamma nail and compression hip screw for trochanteric fractures: a randomized, prospective, comparative study in 210 elderly patients with a new design of the gamma nail. J Orthop Trauma 19(4): 229-233.
-
Lenich A, Mayr E, Ruter A, Mockl C, Fuchtmeier B (2006) First results with the Trochanter Fixation Nail (TFN): a report on 120 cases. Arch Orthop Trauma Surg 126(10): 706-712.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results