Internal Fixation of Sacroiliac Joint via Posterior Approach in Management of Posterior Pelvic Injuries
Object: Sacroiliac dislocation frequently poses a complex problem for the surgical management and stabilization because of the anatomical and biomechanical factors of this transition zone between the spine and pelvis. The authors had used a modification of the Galveston technique, originally described by Allen and Ferguson in the treatment of scoliosis, to achieve rigid spinal-pelvic fixation in patient’s sacroiliac dislocation with vertical and rotational shear. Methods: Twelve patients who had required spinal-pelvic fixation secondary to sacroiliac dislocation and instability fixation was achieved by intraoperative placement of S1 pedicle screws and contoured titanium rods bilaterally into the ilium. Results: During the follow-up period of18 to 36 months (average 26 months), Postoperative posterior fracture reduction was excellent in 9 patients (75%), good in 2 (17%) and fair in 1 patient (8%) (7). Conclusion: The combined use of S1 pedicle screws and the Galveston technique provided immediate stability and sufficient reduction of sacroiliac dislocation.
Introduction
Sacroiliac dislocation which usually accompanies disruption of the symphysis pubis or fracture of the pelvic rami is the most unstable type of pelvic ring injuries. In such injuries, both the anterior and the posterior columns of the pelvic ring are disrupted and the affected hemi pelvis rotates internally with vertical displacement [1]. Deformities of the pelvic ring with marked instability remain with high frequency after non operative treatment of sacroiliac dislocation [2]. According to the published literature, the long term functional prognosis of sacroiliac dislocation may be poor if reduction were not perfect [3]. The optimum reduction of sacroiliac joint dislocation with large vertical displacement sometimes becomes difficult even with external fixator or any conventional internal fixtures as screws, plates and rods. Among the anchors for lumbosacral fixation, a rod inserted between the inner and outer cortices of the ilium has been used for the most caudal anchor in reconstruction of the lumbar spine (Galveston technique) [4].
Van Savage et al used the Galveston technique for fixation of fracture dislocation of the lumbosacral junction [5]. Alternatively, pedicle screw fixation has been developed as the procedure for posterior internal fixation of the thoracic, lumbar and lumbosacral spine. Several reports have shown reduction and fixation of traumatic lumbosacral dislocation by lumbosacral pedicle screw fixation, whereas there have been few reports discussing the treatment of sacroiliac dislocation by the combined use of pedicle screw fixation of the sacrum and the Galveston technique. The objective of this study was to report the results of reduction and fixation of sacroiliac dislocation in 12 patients by the combined use of pedicle screws of the sacrum and Galveston technique.
Material and Methods
Twelve patients with dislocation of sacroiliac joint underwent reduction and fixation by the combined use of pedicle screws of the sacrum and the Galveston technique. They were seven men and five women, with mean age 36.8 years (range, 21 to 47years). The cause of injury was motor cycle accidents in all patients. Seven patients had associated injuries in extremities. Two patients sustained bladder injury and one had head injury. Before surgery, antero-posterior and inlet plain radiographs of the pelvis and computed tomographic (CT) scans were taken in all patients to evaluate the stability and deformities in pelvic ring (Figure 1).

According to Tile's classification for pelvic ring disruption, four patients were type Band 8 patients were type C pelvic injury with unilateral complete disruption of the sacroiliac joint, which comprised vertical displacement and rotational deformity [6]. Five of eight patients with type C had subtype C1 injury with unilateral sacroiliac dislocation, and the remaining three patients had subtype C2 injuries associated with type C on one side and type B external rotation instability on the other side. Two patients with type C injury had sciatic nerve palsy on the ipsilateral side. With regard to injury patterns of the anterior column, five of seven patients had disruption of the symphysis pubis, and the remaining three patients had fractures of the anterior rami. In the four patients with type C2 disruption, only the unilateral side with type C injury which was more unstable and associated with more marked deformity, was surgically stabilized. Surgical technique: the patient was placed in the prone position. A straight longitudinal incision of the skin was made over the S1 pedicle (Figure 2). Both sides of paravertebral muscles were divided transversely at the same level and were retracted cranially and caudally to expose the posterior cranial portion of the sacrum and the affected posterior iliac crest and to observe the disrupted sacroiliac joint during reduction. The superior portion of the origin of the gluteus maximus muscle was detached sub periosteally from the iliac crest, and the posterior portion of the iliac wing was exposed to control the direction of the iliac probe and the rod. The cartilaginous surface of the sacroiliac joint disrupted by fracture dislocation was treated by debridement and extraction of the bony fragment, which may have disturb the reduction. Pedicle screws were inserted into S1 pedicles bilaterally according to the ordinary pedicle screw insertion technique with the help of image intensifier. TheS1 pedicle screws should be converged medially in a triangular fashion and penetrated the anterior cortex of the sacral vertebral body to increase the stability. The rod bent gently to be medially adapted to the prominence of the sacral lamina and was bent sharply at the screw insertion point of the ilium at an anatomic angle of 45ͦ between the iliac wing and the frontal plane of the sacrum. A block of bone measuring about 2× 2 cm was excised from the rod insertion point of the iliac crest to avoid skin irritation by the rod. The rod was inserted into probed hole between the inner and outer tables of the iliac wing (Figure 3).

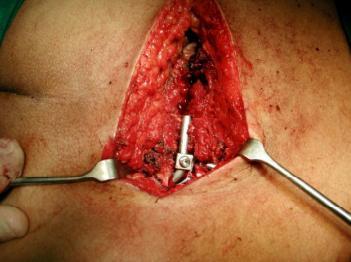
Figure 3: Photo showing application of the rod. The direction of the rod in the frontal plane was downward in all patients according to Galveston method. Two rod-screw connectors were attached to the inserted rod caudally placed in the rod connection to avoid irritation of the L5-S1 facet joint by the connector. For reduction of vertical displacement and angular deformity of the sacroiliac joint, compression force was applied between the inserted rod and each S1pedicle screw using a rod holder and compressor. After introduction of the rod –screw connectors to the pedicle screw, nuts attached to the two screws were alternatively tightened for further reduction (Figure 4). If the space of sacroiliac joint is still widened, compression force was applied between each S1 pedicle screw and the rod to close the opening. After completion of the internal fixation, divided paravertebral muscles were resutured and skin closure was performed. Three out of five patients with symphysis pubis major disruption underwent additional fixation of the symphysis pubis with using dynamic compression plate. The remaining patients were treated by the posterior procedure only.

Results
Median time between trauma and surgery was 2 - 12 days. Mean follow-up was 26±4 months. All patients completed the follow up period. Mean time to full weight bearing was 9 ± 3 weeks, although seven patients had severe injuries of the lower extremities that affected recovery of walking. No motor weakness due to pelvic ring fixation was observed. The vertical displacement was completely reduced in nine patients, and the rotational deformity was completely corrected in seven patients. The reduction was maintained at the time of the final follow-up evaluation (Figures 5 & 6). There were no perioperative complications with the exception of superficial infection in two patients. Postoperative posterior fracture reduction was excellent in 9 patients (75%), good in 2(17%) and fair in 1 patient (8%) [7]. Secondary rotational displacement of the posterior pelvic ring at follow-up X-rays was <5 mm in one patients (8%). Delayed or non-union of the pubic rami occurred in one of the patients that required secondary anterior fixation and in a second one (total 8%) who was able to walk pain free after 6weeks. Delayed-union of the posterior arch was not seen.


Discussion
Mechanically strong constructs of the pelvis, which must be constantly exposed to heavy loads in daily living activities, is produced by the ring-shaped structure. In sacroiliac dislocation, disruption of the posterior column of the pelvis in the sacroiliac joint usually is accompanied by a disruption of the anterior column of the pelvis at the symphysis pubis or as a fracture of the anterior rami. Accordingly, sacroiliac dislocation is considered the most unstable among the various types of traumatic pelvic ring disruption. In this type of injury, the vertically and rotationally unstable pelvis is associated with the loss of bilaterally symmetrical ring structure. In a review article, Tile [8] described patients with vertically unstable disruption of the pelvis who had many problems, 60% of which were persistently painful. The pain usually was present in the posterior sacroiliac area or in the lower lumbar spine and was most frequently associated with unreduced sacroiliac dislocation. Dujardin et al [9], showed in their report on sacroiliac dislocation that pure sacroiliac lesions were associated with poor functional results, especially if reduction was not exact. Therefore, internal stabilization should be performed after confirmation of the stability of the patient's general condition. If the general condition is unstable for injuries of the intra-abdominal organs including the major vessels, life saving management should take procedure over internal fixation of sacroiliac dislocation. In such cases, external fixation may be useful alternative treatment, followed by rigid internal fixation after recovery of the patient's general condition and adequate assessment of the stability of the pelvic ring. However, anterior stabilization using an external fixator alone does not provide sufficient stability for type C injury with severe disruption of the pelvic ring. Some reports have shown that optimum reduction of the sacroiliac dislocation with large pelvic deformity comprises vertical displacement and that rotational deformity is sometimes difficult to treat with an external fixation alone [10, 11, 12, 13, 14]. Conversely, open reduction and internal fixation procedures have been advocated by many investigators to manage sacroiliac dislocation, and have been generally accepted [15, 16, 17, 18, 19]. Some surgeons have reported the results of the management of sacroiliac dislocation by using iliosacral screws fixation [20, 21, 22, 23, 24, 25, 26, 27]. This simple internal fixation is useful for stabilization of sacroiliac dislocation, whereas the complicated anatomy of the sacral foramen causes a risk of nerve injury because of screw placement, and the acquired stability may be not sufficient in the absence of the support from external fixation. Pedicle screw fixation has been developed as a procedure for posterior internal fixation of the thoracic, lumbar, and lumbosacral spines. In the present study, the S1pedicle screws were converged medially in a triangular fashion as the anchor of the sacrum. In addition, the sacral pedicle screws penetrated the anterior cortex of the sacrum to increase the pullout resistance. For another fixation anchor for iliosacral fixation, a rod inserted between the inner and outer cortices of the ilium (Galveston technique) was used. This fixation technique anchor has been demonstrated in biomechanical studies to be the most stable for lumbo sacral fixation among the various fixation procedures [28, 29, 30]. The combined use of S1 pedicle screws and the Galveston technique provide sufficient reduction and high stabilization in the treatment of sacroiliac dislocation. With other posterior sacroiliac fixation techniques using sacroiliac bars and iliosacral screws, reduction must be performed before internal fixation. Conversely, the hybrid anchoring technique in the present study, which used S1 pedicle screws and iliac rod, provided sufficient reduction before fixation . Regarding the direction of iliac rod in the frontal plane , the rod was bent to90ͦ and inserted into the iliac wing in a horizontal direction [31, 32, 33, 34]. The upward or horizontal direction that allowed introduction of the rod into the thinner portion of the iliac wing may enhance the stability of the rod. But insertion of the rod into the thinner portion of the ilium brings difficulty in rod sitting and risk of rod perforation. The downward direction used in our series provided immediate stability and sufficient reduction of the deformity. Also, the reduction was maintained without loss till the end of follow-up period.
Conclusion
The combined use of S1 pedicle screws and the Galveston technique provided immediate stability and sufficient reduction for sacroiliac dislocation. This hybrid internal fixation procedure is useful for reduction and fixation of sacroiliac dislocation associated with the vertical and rotational instability of the pelvic ring.
References
-
Abumi K, Saito M, Iida T, Kaneda K (2000) Reduction and fixation of sacroiliac joint dislocation by the combined use of S1 pedicle screws and the Galveston technique. Spine 25(15): 1977-1984.
-
Lee YS, Kim WS, Park TH (2012) Pediculo-Iliac Screw Fixation in Vertically Unstable Posterior Pelvic Ring Injury. J of Korean Orthop Assoc 47(5): 375-381.
-
Osterhoff G, Ossendorf C, Wanner G, Simmen HP, Werne C (2011) Posterior screw fixation in rotationally unstable pelvic ring injuries. Injury 42(10): 992-996.
-
Lonstein JE, Koop SE, Novachek TF, Perra JH (2012) Results and complications after spinal fusion for neuromuscular scoliosis in cerebral palsy and static encephalopathy using luque galveston instrumentation: experience in 93 patients. Spine 37(7): 583-591.
-
Van Savage JG, Dahners LE, Renner JB, Baker CC (1992) Fracture-dislocation of the lumbosacral spine: case report and review of the literature. J Trauma 33(5): 779-784.
-
Tile M (1999) The management of unstable injuries of pelvic ring. J Bone Joint Surg Br 81(6): 941-943.
-
Nelson DW, Duwelius PJ (1991) CT-guided fixation of sacral fractures and sacroiliac joint disruptions. Radiology 180(2): 527-532.
-
Tile M (1988) Pelvic ring fractures: should they be fixed? J Bone Joint Surg Br 70(1): 1-12.
-
Dujardin FH, Roussignol X, Hossenbaccus M, Thomine JM (2002) Experimental study of the sacroiliac joint micromotion in pelvic disruption. J Orthop Trauma 16(2): 99-103.
-
Grubor P, Milicevic S, Biscevic M, Tanjga R (2011) Selection of treatment method for pelvic ring fractures. MED Arh 65(5): 278-822.
-
Lefaivre KA, Starr AJ, Reinert CM (2009) Reduction of displaced pelvic ring disruptions using a pelvic reduction frame. J Orthop Trauma 23(4): 299-308.
-
Mason WT, Khan SN, James CL, Chesser TJ, Ward AJ (2005) Complications of temporary and definitive external fixation of pelvic ring injuries. Injury 36(5): 599-604.
-
Galois L, Pfeffer F, Mainard D, Delagoutte JP (2003) The value of external fixation for unstable pelvic ring injuries. Acta Orthop Belg 69(4): 321-327.
-
Ponsen KJ, Hoek van Dijke GA, Joosse P, Snijders CJ (2003) External fixator’s for pelvic fractures: comparison of the stiffness of current systems. Acta Orthop Scand 74(2): 165-171.
-
Calafi LA, Routt ML Jr (2013) Posterior iliac crescent fracture-dislocation: What morphological variations are amenable to iliosacral screw fixation? Injury 44(2): 194-198.
-
Chen W, Pan ZJ, Chen JS (2009) Biomechanical research on anterior double-plate fixation for vertically unstable sacroiliac dislocations. Orthop Surg 1(2): 127-131.
-
Korovessis PG, Magnissalis EA, Deligianni D (2006) Biomechanical evaluation of conventional internal contemporary spinal fixation techniques used for stabilization of complete sacroiliac joint separation: a 3-dimensional unilaterally isolated experimental stiffness study Spine 31(25): E941-E951.
-
Sagi HC, Ordway NR, DiPasquale T (2004) Biomechanical analysis of fixation for vertically unstable sacroiliac dislocations with iliosacral screws and symphyseal plating. J Orthop Trauma 18(3): 138- 143.
-
Korovessis P, Stamatakis M, Baikousis A (2000) Posterior stabilization of unstable sacroiliac injuries with the Texas Scottish Rite Hospital spinal instrumentation. Orthopedics 23(4): 323-327.
-
Jacob AL, Messmer P, Stock KW, Suhm N, Baumann B, et al. (1997) Posterior pelvic ring fractures: closed reduction and percutaneous CT-guided sacroiliac screw fixation. Cardiovasc Intervent Radiol 20(4): 285-294.
-
Baskin KM, Cahill AM, Kaye RD, Born CT, Grudziak JS, et al. (2004) Closed reduction with CT-guided screw fixation for unstable sacroiliac joint fracture- dislocation. Pediatr Radiol 34(12): 963-969.
-
Tsukushi S, Katagiri H, Nakashima H, Shido Y, Wasa J (2003) Computed tomography-guided screw fixation of a sacroiliac joint dislocation fracture: a case report. J Orthop Sci 8(5): 729-732.
-
Griffin DR, Starr AJ, Reinert CM, Jones AL, Whitlock S (2003) Vertically unstable pelvic fractures fixed with percutaneous iliosacral screws: does posterior injury pattern predict fixation failure? J Orthop Trauma 17(6): 399-405.
-
Calafi LA, Routt ML (2013) Posterior iliac crescent fracture-dislocation: What morphological variations are amenable to iliosacral screw fixation? Injury 44(2): 194-198.
-
Pan WB, Liang JB, Wang B, Chen GF, Hong HX, et al. (2012) The invention of an iliosacral screw fixation guide and its preliminary clinical application. Orthop Surg 4(1): 55-59.
-
Zheng Z, Zhang Y, Hou Z, Hao J, Zhai F, et al. (2012) The application of a computer-assisted thermoplastic membrane navigation system in screw fixation of the sacroiliac joint-a clinical study. Injury 43(4): 495-499.
-
Fischer A, Binder E, Reif U, Biel M, Bokemeyer J, et al. (2012) Closed reduction and percutaneous fixation of sacroiliac luxations in cats using 2.4 mm cannulated screws - a cadaveric study. Vet Comp Orthop Traumatol 25(1): 22-27.
-
Mattei TA, Fassett DR (2013) Low-profile pelvic fixation with sacral alar-iliac screws. Acta Neuro chir (Wien) 155(2): 293-297.
-
Mindea SA, Chinthakunta S, Moldavsky M, Gudipally M, Khalil S (2012) Biomechanical comparison of spinopelvic reconstruction techniques in the setting of total sacrectomy. Spine 37(26): E1622-E1627.
-
Tis JE, Helgeson M, Lehman RA, Dmitriev AE (2009) A biomechanical comparison of different types of lumbopelvic fixation. Spine 34(24): E866-E872.
-
Jackson RJ, Gokaslan ZL (2000) Spinal-pelvic fixation in patients with lumbosacral neoplasms. J Neurosurg 92(S1): 61-70.
-
Allen BL, Ferguson RL (1988) A 1998 perspective on the Galveston technique of pelvic fixation. Orthop Clin North Am 19(2): 409-418.
-
Allen BL Jr, Ferguson RL (1988) The Galveston experience with L-rod instrumentation for adolescent idiopathic scoliosis Clin Orthop Relat Res 229: 59-69.
-
Allen BL Jr, Ferguson RL (1984) The Galveston technique of pelvic fixation with L-rod instrumentation of the spine. Spine 9(4): 388-394.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results