Anomalous Origin and Course of the Posterior Circumflex Humeral Artery: Clinical Interest in Shoulder Arthroscopy and Open Procedures
The posterior circumflex humeral artery usually cross the quadrilateral space with the axillary nerve but there are variations as this case, that artery runs down this space. We study this artery and its relations in order to advice to injury it during surgical and invasive procedures such as shoulder arthroscopy and also prevent vascular repercussions. An embryological and clinical explanation is also considered.
Roberto Seijas3,4, Laura Cuni1, Mónica Buxeda1 and Andrés
Combalia5
embryological and clinical explanation is also considered.
Introduction
A few studies have reported variations of origin and course of the posterior circumflex humeral artery. However, to our knowledge there are no studies which correlate the posterior circumflex humeral artery variation course with adjacent bone, muscular and neurovascular structures. Knowledge of this variation can avoid injury to it during surgical and invasive procedures such as shoulder arthroscopy and also prevent vascular repercussions. An embryological and clinical explanation is also considered.
Material and Methods
Thirty six dissections fixed in 10% formalin, selected consecutively and dissected in the Area of Human Anatomy and Embryology at the University of Barcelona in eighteen cadavers were studied (average age 77.4 year); 18 (50%) of them were men and 18 (50%) women. The dissection was performed by planes: first subcutaneous cell skin and tissue, then the origins and insertions of the muscles and their relations with vessels and nervous of the axillar zone. The axillar plexus and theirs nerves and the artery axillary branches were identified. As no scars were seen in any corpse, previous surgery was ruled out. In one right upper limb in a 70- year-old female, an unusual origin and course of the posterior circumflex humeral artery was observed. In order to measure the length of the axillary artery and its branches the upper limb was kept in the abducted position. The axillary space, the brachial plexus and the axillary artery with all its branches were carefully dissected.
Results
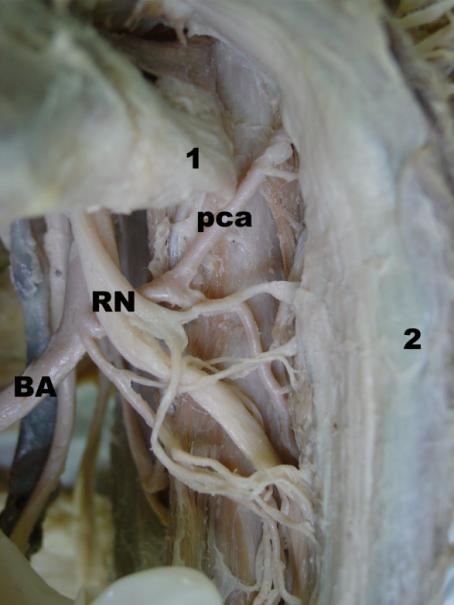
The posterior circumflex humeral artery were seen arising from the third part of the axillary artery in common with the profunda brachii artery very close to the radial nerve (Figure 1 and 2). The common trunk ran parallel 1.5 cm along the inferior border of the teres major muscle and divided 2 cm distal to the brachial artery. While the profunda branchii artery followed the radial nerve and crossed the triangular space, the posterior circumflex humeral artery did not cross the quadrilateral space with the axillary nerve (Figure 2). Thus, the posterior circumflex humeral artery was located 4 cm below the axillary nerve, perpendicular to the inferior margin of the teres major muscle, crossing the anterior face of the long head of the triceps muscle, curving round the humeral neck of the humerus along 3 cm and ending at the deep surface of the middle third of the deltoid muscle (Figure 1). This artery supplied the shoulder joint, deltoid, teres major, teres minor and long head of the triceps muscles. A small branch arising from the common trunk of the posterior circumflex humeral artery and the profunda brachii artery, at 0.5 cm from the axillary artery, was observed piercing and supplying the coracobrachialis muscle and finishing at the proximal humerus bone.
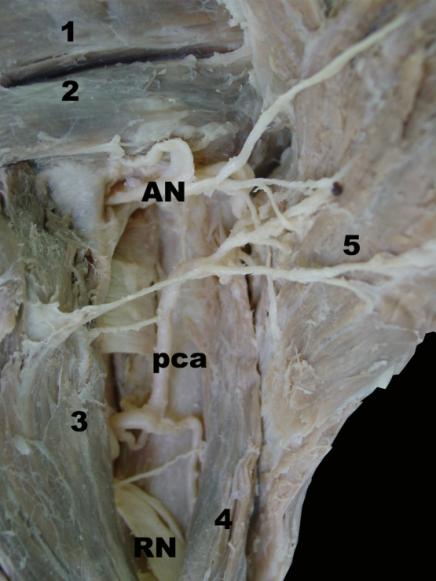
Figure 1: Posterior view of right shoulder shows the infraspinous (1) and teres minor muscle (2), under, axillary nerve (AN) is crossing the quadrilateral space. The posterior circumflex humeral artery (pca) goes close to the radial nerve (RN), outside the quadrilateral space, under the longus head of triceps brachii muscle (3) and medial to the lateral head of triceps brachii muscle (4) ending at the deep surface of the deltoid muscle (5).
Discussion
The importance of the posterior circumflex humeral artery resides in several aspects. First of all, from the classical anatomical point of view, one should consider the wide vascular territory that it supplies, which includes the humerus head, the shoulder joint, posterior and middle parts of the deltoid muscle, teres major and minor muscles, and long and lateral heads of the triceps muscle [1, 2]. The posterior circumflex humeral artery normally arises independently from the third part of the axillary artery at the distal border of the subscapularis [3, 4]. It runs backwards with the axillary nerve through a quadrilateral space and curves posteriorly to the surgical neck of the humerus [5]. It gives off a descending branch which anastomoses with the deltoid branch of the profunda brachii artery and with the anterior circumflex humeral and acromial branches of the suprascapular and thoraco-acromial arteries [6]. With regards to its origin, the posterior circumflex humeral artery may arise as a common trunk with the subscapular artery in 22-40% of cases [4, 7], as a common trunk with the anterior circumflex humeral artery in 16- 23.4% of cases [4, 6]; or, less frequently, with the profunda brachii artery in 2-11.5% of cases [4, 8]. Few studies have reported variations of the posterior circumflex humeral artery. Gray [5] cites a variation of the posterior circumflex humeral artery passing back below the teres major muscle but no other details have been reported. We describe an artery which did not cross the quadrilateral space and reached the deltoid muscle passing inferior to the shoulder joint. From a clinical point of view, knowledge of arterial variation is essential in planning surgical and reconstructive procedures. It should be emphasised that this artery can be injured during shoulder arthroscopy [9, 10] and surgical treatment of fractures (whether percutaneous or open procedures, [11, 12, 13, 14], and knowledge of its normal course and variations can be of great interest in both plastic reconstructive procedures [1] and cases of comminute fractures of the proximal humerus [15]. Although some authors argue that its alteration does not generally have vascular repercussions because blood supply can be replaced by the profunda brachii artery [16], others point out that a deficient vascular supply of the posterior circumflex humeral artery territory may have significant consequences with regard to the success or failure of a variety of surgical procedures [9, 10, 17]. Moreover, aneurysms of the posterior circumflex humeral artery could cause ischemia of the arm and hand [18]. Thus, although this artery has been surprisingly neglected in some previous reports, it has attracted more attention in current publications because of its important role in circulation. Here we have reported the association of two unusual anatomical variations affecting the origin and course of the posterior circumflex humeral artery. According to the literature, the variation of the origin observed in the specimen cadaver studied is the less frequent [19, 20, 4, 8]. The course and variations for the posterior circumflex humeral artery have not widely been reported. Interestingly, we have observed that in the reported anatomical variation case the artery does not cross the quadrilateral space but follows the lower border of the teres major muscle. Thus, although it does not strictly participate in the pathogenesis of quadrilateral space syndrome [21, 22, 23], it must be taken into account in the posteroinferior portal for shoulder arthroscopy [24] in order to avoid damaging it in any subsequent approach. The origin of these anomalies is attributed to defects in the embryonic development of the vascular plexi of the upper limb buds [25]. The vascular system of the upper limb begins at stage 12 (3-5 mm; 26 days) as a capillary plexus entering the limb bud, but it is not until stage 15 (7-9 mm; 33 days) that both subclavian and axillary arteries can first be seen entering the limb and branching into an undifferentiated capillary network [26]. As differentiation of the humerus proceeds in stage 17 (11- 14 mm, 41 days) [27] the axillary artery acquires a differentiated morphology. From a gestational age of 24 weeks, minimal differences compared with the adult shoulder joint and its structures are observed [28]. An arrest at any stage of development, showing regression, retention, or reappearance, may produce variations in the arterial origin and courses of the major upper limb vessels [29]. In conclusion, we would like to emphasize that surgeons should keep this variation in mind in order to preserve this vessel and avoid unpredicted bleeding caused by accidental injury to it. An inexperienced surgeon may become anatomically disoriented by the absence of the posterior circumflex humeral artery in the quadrilateral space, and thus knowledge of anatomical variations is indispensable for performing successful shoulder surgery.
References
-
Hue E, Gagey O, Mestdagh H, Fontaine C, Drizenko A, et al. (1998) The blood supply of the deltoid muscle. Application to the deltoid flap technique. Surg Radiol Anat 20(3): 161-165.
-
Testut L, Latarjet A (1979) Anatomía Humana (vol II) 1th Barcelona: Salvat S.A. pp: 285.
-
Bergman RA, Thompson SA, Afifi AK (1984) Catalog of human variation. Vol 1. Munich: Urban & Schwarzenberg. pp: 103-106.
-
Patnaik VVG, Kalsey G, Singla Rajan K (2000) Branching pattern of axillary artery - A morphological study. J Anat Soc India 49: 127-132.
-
Gray H (2005) Gray’s Anatomy. 39th (Edn.), New York: Elsevier Churchill Livingstone. pp: 844-845.
-
Trotter M, Henderson JL, Gass H, Brua RS, Weisman S, et al. (1930) The origin of branches of the axillary arteries in white and American Negros. Anat Rec 46: 133-137.
-
Adachi B (1928) Das arteriensystem der Japaner. Vol 1, Kyoto, pp: 205-210.
-
Pelligrini A (1906) Le arteriae subclavia e axillaris nell uomo studiate col. Metodo statisco Arch Ital Anat Embriol 5: 205-466.
-
Lo IK, Lind CC, Burkhart SS (2004) Glenohumeral arthroscopy portals established using an outside-in technique: neurovascular anatomy at risk. Arthroscopy 20(6): 596-602.
-
McCarthy WJ, Yao JS, Schafer MF, Nuber G, Flinn WR, et al. (1989) Upper extremity arterial injury in athletes. J Vasc Surg 9(2): 317-327.
-
Kamineni S, Ankem H, Sanghavi S (2004) Anatomical considerations for percutaneous proximal humeral fracture fixation. Injury 35(11): 1133-1136.
-
Meyer C, Alt V, Hassanin H, Heiss C, Stahl JP, et al. (2005) The arteries of the humeral head and their relevance in fracture treatment. Surg Radiol Anat 27(3): 232-237.
-
Riemer BL, D’Ambrosia R (1992) The risk of injury to the axillary nerve, artery, and vein from proximal locking screws of humeral intramedullary nails. Orthopedics 15(6): 697-699.
-
Rowles DJ, McGrory JE (2001) Percutaneous pinning of the proximal part of the humerus. An Anatomic study. J Bone Joint Surg Am 83-A(11): 1695-1699.
-
Brooks CH, Revell WJ, Heatley FW (1993) Vascularity of the humeral head after proximal humeral fractures. An anatomical cadaver study. J Bone Joint Surg Br 75(1): 132-136.
-
Gerber C, Lambert S, Hoogewoud H (1996) Absence of avascular necrosis of the humeral head after post- traumatic rupture of the anterior and posterior humeral circumflex arteries. A case report. J Bone Joint Surg Am 78(8): 1256-1259.
-
Abrassart S, Stern R, Hoffmeyer P (2006) Arterial supply of the glenoid: An anatomic study. J Shoulder Elbow Surg 15(2): 232-238.
-
Vlychou M, Spanomichos G, Chatziioannou A, Georganas M, Zavras GM (2001) Embolisation of a traumatic aneurysm of the posterior circumflex humeral artery in a volleyball player. Br J Sport Med 35(2): 136-137.
-
DeGaris CF, Swartley WB (1928) The axillary artery in white and negro stocks. Am J Anat 41(2): 353-397.
-
Huelke DF (1959) Variations in the origins of the branches of the axillary artery. Anat Rec 135(1): 33- 41.
-
Cahill BR, Palmer RE (1983) Quadrilateral space syndrome. J Hand Surg Am 8(1): 65-69.
-
Francel TJ, Delton AL, Campbell JN (1991) Quadrilateral space syndrome: diagnosis and operative decompression technique. Plast Reconstr Surg 87(5): 911-916.
-
McKowen HC, Voorhies RM (1987) Axillary nerve entrapment in the quadrilateral space. Case report. J Neurosurg 66(6): 932-934.
-
Davidson PA, Rivenburgh DW (2002) The 7-o’clock posteroinferior portal for shoulder arthroscopy. Am J Sport Med 30(5): 693-696.
-
Çavdar S, Zeybek A, Bayramiçli M (2000) Rare variation of the axillary artery. Clin Anat 13(1): 66-68.
-
Rodriguez Niederführ M, Burton GJ, Deu J, Sañudo JR (2001) Development of the arterial pattern in the upper limb of staged human embryos: normal development and anatomic variations. J Anat 199: 407-417.
-
O’Rahily R, Gardner E (1975) The timing and sequence of events in the development of the limbs in the human embryo. Anat Embryol 148(1): 1-23.
-
Tena-Arregui J, Barrio-Asensio C, Puerta-Fonolla J, Murillo-Gonzalez J (2005) Arthroscopic study of the shoulder joint in fetuses. Arthroscopy 21(9): 1114- 1119.
-
Hamilton WJ, Mossman HW (1972) Cardiovascular system. In: Human embryology. 4th(Edn.), Baltimore: Williams & Wilkins. pp: 271-290.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results