Allied Disorders and Complications of Rheumatoid Arthritis - A Statistical Comorbidity Study of 234 Autopsy Patients
Objective: The incidence of co-morbidities is higher in rheumatoid arthritis (RA) than in the general population. Associated diseases accompanying RA may modify the clinical course and symptoms of RA and may influence the prevalence and mortality of complications related to the basic diseases and vica versa. The aim of this study was to determine statistically the possible effect of certain allied disorders: type 2 diabetes mellitus (DM), atherosclerosis (Ath), hypertension (HT), tuberculosis (Tb) with miliary dissemination (mTb), and malignant tumours (mTu) on the prevalence and mortality of RA related complications: systemic autoimmune vasculitis (AV), AA amyloidosis (AAa), lethal cardiac insufficiency (CI) caused by endo-, myo- or pancarditis, with or without interstitial pneumonitis, furthermore lethal septic infection (SI) combined with septic vasculitis (SV) or purulent arthritis (PA) Patients and Methods: Twohundred thirty four (234) non- selected autopsy patients with RA were studied. RA was confirmed clinically according to the criteria of the American College of Rheumatology (ACR). The presence of DM, Ath, HT, Tb, mTb, or mTu was determined and analyzed retrospectively, reviewing the clinical and pathological reports. The prevalence and mortality of AV, AAa, CI, SI, SV and PA was determined at autopsy and confirmed by a detailed review of extensive histological material. Demographics of different patient cohorts were compared with the Student (Welch) tprobe. The link between Ath, HT, DM, Tb, mTb, or mTu and AV, AAa, CI, SI, SV or PA was analyzed by Pearson's chisquared (χ2) test. Results: RA associated with DM in 41 (17.52%), with severe Ath in 107 (45.72%), with HT in 41 (17.52%), with with Tb in 28 (11.96%), including active disseminated mTb in 9 (3.85%), and with mTu in 27 (11.54%) of 234 patients. RA was complicated by AV in 43 (18.38 %), by AAa in 48 (20.51%), by CI in 15 (6.41%), and by lethal SI in 33 (14.10%) of 234 patients. SI was combined with PA in 15 (6.41% of 234; 45.45% of 33) or with SV in 7 (2.99% of 234; 21.21% of 33) patients; PA or SV did not occur without generalized SI. The relationship between Ath and AV, AV (lethal), AAa, AAa (lethal), CI, SI, PA or SV was consequently inverse and mostly significant. There was a positive and significant correlation between Tb or mTb and AV, furthermore between mTb and mortality of AV. Discussion and Conclusions: The consequently inverse and (in most cases) significant correlation between atherosclerosis and autoimmune vasculitis, amyloidosis or sepsis shows that the prevalence or mortality of AV, AAa and SI was not influenced by Ath. RA patients with Ath may represent a special group, characterized by lower incidence of SV, AAa, SI, CI, and carry a better prognosis. Ath is basically an age-dependent phenomenon, characteristically present in RA patients with advanced age, while AV, AAa (with or without lethal outcome) and SI are complications of RA, and characterize severe forms of disease, mostly in younger patients and with an earlier onset (without pronounced atherosclerosis). The positive and significant correlation between Tb or mTb and AV suggest a positive influence of Tb or mTb on the prevalence of vasculitis, e.g. the presence of Tb or endogenous exacerbation and miliary dissemination of Tb may promote the AV. The significant connection between mTb and mortality of AV indicates an increased risk of lethal outcome.
Introduction
The incidence of co-morbidities (including “hypertension, dyslipidemia, myocardial infarction or angina, stroke, osteoarthritis, lung cancer, colon cancer, pulmonary tuberculosis, asthma, diabetes, depression, thyroid disease and chronic kidney disease”) is higher in rheumatoid arthritis (RA) than in the general population [1]. According to van den Hoek, et al. (2017) the mortality in patients with rheumatoid arthritis is higher for cardiovascular, respiratory, musculoskeletal and digestive diseases than in the general population [2].
Associated diseases accompanying RA may modify the clinical course and symptoms of RA and may influence the prevalence and mortality of complications related to the basic diseases and vica versa [3].
The aim of this study was to determine statistically the possible effect of certain allied disorders: type 2 diabetes mellitus (DM), atherosclerosis (Ath), hypertension (HT), tuberculosis (Tb) with miliary dissemination (mTb), and malignant tumours (mTu) on the prevalence and mortality of RA related complications: systemic autoimmune vasculitis (AV), AA amyloidosis (AAa), lethal cardiac insufficiency (CI) caused by endo-, myo- or pancarditis, with or without interstitial pneumonitis, furthermore lethal septic infection (SI) combined with septic vasculitis (SV) or purulent arthritis (PA)
Patients and Methods
Twohundred thirty four (234) non- selected autopsy patients with RA were studied. RA was confirmed clinically according to the criteria of the American College of Rheumatology (ACR) [4].
The presence of DM, Ath, HT, Tb, mTb, or mTu was determined and analyzed retrospectively, reviewing the clinical and pathological reports. The prevalence and mortality of AV, AAa, CI, SI, SV and PA was determined at autopsy and confirmed by a detailed review of extensive histological material.
Demographics of different patient cohorts were compared with the Student (Welch) t-probe [5]. The link between Ath, HT, DM, Tb, mTb, or mTu and AV, AAa, CI, SI, SV or PA was analyzed by Pearson's chi-squared (χ2) test [5].
Glossary of Definitions
- Allied disorder: important comorbidity associated with RA with or without direct causal role in death
- RA related complication: consequence of RA with or without direct causal role in death
Atherosclerosis was diagnosed in RA patients only in cases when it was present macroscopically as a “severe” atherosclerotic process (characterized by occlusive thrombosis or sclerotic ulcers) or when it was the basic disease leading to death. Moderate changes like hyaline or sclerotic plaques without causal role in death were not mentioned as “atherosclerosis” since such changes are frequent in elderly RA patients [3].
- "Prevalence" of vasculitis: concerns the presence of inflammatory infiltration and structural changes in blood vessels of different calibers
- Systemic vasculitis of autoimmune origin (AV): was defined as one of the basic manifestations of RA, excluding other causes of vasculitis, like hypertension, diabetes mellitus, tumors, septic infections etc. [3, 6].
- Systemic vasculitis of septic origin (SV) was defined as an important complication of generalized lethal septic infection (SI). The clinically identified pathogenic agents and the strong, significant and positive correlation between SV and SI supported the infectious origin of SV [3, 7].
- "Prevalence" of AAa: concerns the presence of amyloid A deposits in blood vessels of different calibers or in different tissue structures of various organs.
- AAa was diagnosed histologically according to Romhányi by a modified (more sensitive) Congo red staining [8, 9]. Amyloid A deposits were identified in serial histologic sections by immunohistochemical and histo chemical methods [10].
Results
RA associated with DM in 41 (17.52%), with severe Ath in 107 (45.72%), with HT in 41 (17.52%), with with Tb in 28 (11.96%), including active disseminated mTb in 9 (3.85%), and with mTu in 27 (11.54%) of 234 patients.
Adult type 2 DM was clinically recognized and controlled in all cases and no patients died of it; the basic diseases leading to death were different in all RA patients associated with DM. Ath led directly to death in 61 (57.01% of 107 and 26.06% of 234), HT in 2 of 41, Tb with mTb in 3 of 28, and mTu in 12 of 27 patients. In lethal cases only the influence of Ath was analyzed as a RA related complication; the others, because of their limited numbers were not tested.
RA was complicated by AV in 43 (18.38%), by AAa in 48 (20.51%), by CI with lethal outcome (caused exclusively by endo-, myo- or pancarditis with or without interstitial pneumonitis) in 15 (6.41%), and by lethal SI in 33 (14.10%) of 234 patients. SI was combined with PA in 15 (6.41% of 234; 45.45% of 33) or with SV in 7 (2.99% of 234; 21.21% of 33) patients; PA or SV did not occur without generalized SI.
AV led to death in 24 (10.25%), AAa in 20 (8.54%) of 234 patients. The prevalence and mortality of CI, SI (with or without SV and PA) were identical, because only lethal cases were listed.
Demographics, onset and duration of RA associated with DM, Ath, HT, Tb, mTb and mTu or complicated by AV, AAa, CI and SI (including PA or SV) are summarized in Table 1.
| Sex | Number of autopsies | Mean age in years at death ± SD | Range (in years) | Mean age at onset of disease ± SD | Disease duration (in years) mean ± SD |
| :--- | :--- | :--- | :--- | :--- | :--- |
| RA patients (total) | 234 | 66.25±13.15 | 16–88 | 51.02±16.58 | 14.76±10.79 |
| Female | 170 | 66.31±12.82 | 16–88 | 50.46±15.92 | 15.42±11.12 |
| Male | 64 | 66.08±13.97 | 19–88 | 52.55±18.18 | 12.96±9.60 |
| With DM | 41 of 234 | 68.17±8.85 | 47–83 | 54.32±13.99 | 15.10±10.67 |
| Female | 30 | 66.77±8.04 | 47–82 | 53.00±14.52 | 15.13±11.74 |
| Male | 11 | 72.00±9.75 | 48–83 | 58.13±11.54 | 15.00±6.69 |
| With Ath | 107 of 234 | 71.90±10.76 | 47–88 | 56.85±14.23 | 14.43±11.56 |
| Female | 78 | 71.47±11.62 | 47–88 | 54.98±14.19 | 15.94±12.36 |
| Male | 29 | 73.03±7.69 | 56–88 | 61.70±13.12 | 10.50±7.90 |
| Ath (lethal) | 61 of 107 | 72.83±12.49 | 47–88 | 54.59±13.97 | 17.05±12.45 |
| Female | 49 | 72.15±13.44 | 47–88 | 53.67±13.79 | 17.61±13.01 |
| Male | 12 | 75.58±6.01 | 64–84 | 58.38±14.08 | 14.75±9.47 |
| Ath (associated) | 46 of 107 | 70.67±7.86 | 56 – 88 | 59.84±14.00 | 10.97±9.18 |
|---|---|---|---|---|---|
| Female | 29 | 70.34±7.63 | 56 – 84 | 57.26±14.59 | 13.05±10.53 |
| Male | 17 | 71.24±8.21 | 56 – 88 | 63.92±11.93 | 7.67±4.92 |
| With HT | 41 of 234 | 69.37±8.67 | 47 – 86 | 49.05±14.00 | 19.14±9.18 |
| Female | 29 | 68.93±7.63 | 47 – 86 | 46.44±15.01 | 21.06±12.43 |
| Male | 12 | 70.42±6.98 | 59 – 82 | 56.88±13.65 | 13.38±7.73 |
| With Tb | 28 of 234 | 68.93±10.10 | 47 – 84 | 54.96±15.66 | 14.33±12.14 |
| Female | 21 | 69.76±10.78 | 47 – 84 | 55.00±16.87 | 15.30±13.28 |
| Male | 7 | 66.43±7.11 | 56 – 78 | 54.86±11.54 | 11.57±7.40 |
| With mTb | 9 of 28 | 68.00±9.75 | 50 – 82 | 59.38±7.35 | 9.75±4.89 |
| Female | 8 | 67.88±10.34 | 50 – 82 | 58.71±7.63 | 10.43±4.87 |
| Male | 1 | 69.00±0.00 | 69 – 69 | 64.00±0.00 | 5.00±0.00 |
| With mTu | 27 of 234 | 66.81±12.72 | 34 – 87 | 55.41±16.86 | 11.64±8.04 |
| Female | 19 | 64.37±12.84 | 34 – 81 | 52.47±16.81 | 11.41±8.23 |
| Male | 8 | 72.63±10.32 | 53 – 87 | 64.40±12.67 | 12.40±7.31 |
| With AV | 43 of 234 | 68.26±10.80 | 32 – 88 | 56.85±15.24 | 12.08±10.82 |
| Female | 26 | 68.96±11.84 | 32 – 88 | 58.04±13.68 | 12.71±9.58 |
| Male | 17 | 67.12±8.84 | 53 – 83 | 55.06±17.16 | 11.13±12.39 |
| AV (lethal) | 24 of 43 | 63.96±10.86 | 32 – 82 | 52.83±16.34 | 12.52±11.96 |
| Female | 15 | 65.00±12.65 | 32 – 82 | 54.29±13.65 | 13.07±9.25 |
| Male | 9 | 62.22±6.56 | 53 – 72 | 50.56±19.60 | 11.67±15.20 |
| With AAa | 48 of 234 | 63.75±14.76 | 19 – 88 | 46.66±17.82 | 17.18±9.85 |
| Female | 38 | 65.13±11.36 | 32 – 88 | 47.25±16.48 | 17.75±10.55 |
| Male | 10 | 58.50±22.81 | 19 – 88 | 44.00±22.72 | 14.63±5.02 |
| AAa (lethal) | 20 of 48 | 56.80±17.55 | 19 – 88 | 40.33±20.31 | 17.28±9.44 |
| Female | 13 | 59.54±12.09 | 32 – 75 | 40.25±17.49 | 18.67±10.74 |
| Male | 7 | 51.71±23.86 | 19 – 88 | 40.50±25.00 | 14.50±5.02 |
| With CI | 15 of 234 | 66.67±15.45 | 20 – 83 | 56.17±18.99 | 11.17±9.95 |
| Female | 9 | 69.56±10.19 | 52 – 82 | 61.14±17.50 | 12.71±12.30 |
| Male | 6 | 62.17±20.18 | 20 – 83 | 49.20±18.80 | 9.00±4.20 |
| With SI | 33 of 234 | 62.33±8.63 | 41 – 83 | 49.00±12.41 | 13.45±9.04 |
| Female | 23 | 61.35±9.42 | 41 – 83 | 48.45±13.50 | 13.20±9.65 |
| Male | 10 | 64.60±5.87 | 52 – 71 | 50.22±9.43 | 14.00±7.48 |
| With PA | 15 of 33 | 59.47±7.03 | 46 – 71 | 44.08±10.45 | 16.38±10.31 |
| Female | 10 | 58.20±6.69 | 46 – 68 | 42.88±10.84 | 16.63±11.34 |
| Male | 5 | 62.00±7.01 | 52 – 71 | 46.00±9.49 | 16.00±8.39 |
| With SV | 7 of 33 | 61.57±7.74 | 51 – 70 | 51.14±12.03 | 10.43±8.78 |
| Female | 4 | 57.25±7.36 | 51 – 69 | 45.75±13.12 | 11.50±11.15 |
| Male | 3 | 67.33±3.09 | 63 – 70 | 58.33±4.19 | 9.00±3.27 |
Table 1: Sex, mean age with SD, range, onset and disease duration of RA patients associated with DM (n=41), Ath (n=107), HT (n=41
Table 1: Sex, mean age with SD, range, onset and disease duration of RA patients associated with DM (n=41), Ath (n=107), HT (n=41), Tb (n=28), mTb (n=9) and mTu (n=27) or complicated by AV (n=43), AAa (n=48), CI (n=15), SI (n=33) including PA (n=15) or SV (n=7). Glossary to Table 1: RA – Rheumatoid Arthritis Lethal – allied disorder or RA related complication with lethal outcome Associated – allied disorder (accompanying disease) without direct causal role in death DM – type 2 Diabetes Mellitus; Ath: Atherosclerosis; HT: HyperTension; Tb: Tuberculosis; mTb: miliary Tuberculosis; mTu: malignant Tumors; AV: systemic Autoimmune Vasculitis; AAa: systemic AA amyloidosis; CI: Cardiac Insufficiency with lethal outcome; SI: lethal Septic Infection; PA: Purulent Arthritis; SV: systemic Septic Vasculitis; SD: Standard deviation Comparing the mean age of female and male RA patients (n=234) associated with DM, Ath, HT, Tb, mTb and mTu or complicated by AV, AAa, CI and SI (including PA or SV) to the mean age of total population, there was no significant difference between patient cohorts except RA patients with Ath, lethal AAa, and SI including PA.
The mean age of RA patients associated with Ath (n=107) was significantly higher (71.90 years versus 66.25; p< 0.0000015), both of females (71.47 years versus 66.31; p< 0.00014) and males (73.03 years versus 66.08; p< 0.003).
Comparing the subgroups of Ath (lethal outcome n=61 of 107, and coexistent associated disease n=46 of 107) with the mean age of the total population (n=234), the tendency was the same only the levels of difference were disparate:
The mean age of RA patients with lethal outcome of Ath (n=61) was significantly higher (72.83 years versus 66.25; p< 0.0000043), for both females (72.15 years versus 66.31; p< 0.00036) and males (75.58 years versus 66.08; p< 0.001), and the mean age of RA patients with coexistent associated Ath (n=46) was significantly higher (70.67 years versus 66.25; p< 0.003), and it was the same in women (70.34 years versus 66.31; p< 0.022). The mean age of males was higher than the mean age of total population (71.24 years versus 66.08; p< 0.063 – NS), but this difference was not significant (Tables 1 & 2).
Comparing the onset of RA and duration of disease there was a collateral (parallel) tendency between RA patients (n=234) with mTb (n=9) or AV (n=43).
RA started later in patients with mTb (59.38 years versus 51.02; p< 0.033), who died earlier (9.75 years versus 14.36; p< 0.563; p< 0.020), and it was the same in women (58.71 years versus 50.46; p< 0.050, and 10.43 years versus 15.42; p< 0.040).
RA patients with complications of AV (n=43) showed a similar predisposition as patients with mTb. RA started later in patients with AV (56.85 years versus 51.02; p< 0.037), who died earlier (9.75 years versus 14.36; p< 0.167 – NS), but the latter was not significant. The tendency was similar both in women (onset of RA: 58.04 years versus 50.46; p< 0.022, and duration of disease: 10.43 years versus 15.42 p< 0.230 – NS) and men (onset of RA: 55.06 years versus 52.55; p< 0.630 – NS, and duration of disease: 11.13 years versus 12.96; p< 0.604 – NS), but partly without significant relationship.
The mean age of RA patients with lethal AAa (n=20) was lower (56.80 years versus 66.25; p< 0.032), and RA started significantly earlier (40.33 years versus 51.02; p< 0.049), than in the general population (n=234).
The mean age of RA patients with SI (n=33) or PA (n=15) was significantly lower collate to the average of total population (62.33 or 59.47 years versus 66.25; p< 0.028 or p< 0.004). The mean age of females complicated by SI (n=23) or PA (n=10) was significantly lower as well (61.35 or 58.20 years versus 66.31 or 66.08; p< 0.031 or p< 0.005). The mean age of males complicated by SI (n=10) or PA (n=5) was lower also (64.60 or 62.00 years versus 66.08; p< 0.579 – NS or p< 0.337 – NS), but these differences were not significant.
The statistical links (“p” values of significance) between RA patients with DM, Ath, HT, Tb, mTb, mTu or complicated by AV, AAa, SI (including PA or SV) are summarized in Table 2.
| RA patients n=234 | Age | Onset of disease | Disease Duration | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| RA pts. n=234 versus pts. with DM n=41 of 234 | p< 0,240 | p< 0,251 | p< 0,873 | ||||||||
| Female n=170 of 164 versus n=30 of 41 | p< 0,797 | p< 0,459 | p< 0,915 | ||||||||
| Male n=64 of 164 versus n=11 of 41 | p< 0,113 | p< 0,294 | p< 0,493 | ||||||||
| RA pts. n=234 versus pts. with Ath n=107 of 234 | p< 0,00000 | p< 0,006 | p< 0,873 | ||||||||
| Female n=170 of 164 versus n=78 of 107 | p< 0,00014 | p< 0,065 | p< 0,793 | ||||||||
| Male n=64 of 164 versus n=29 of 107 | p< 0,003 | p< 0,287 | p< 0,026 | ||||||||
| RA pts. n=234 versus pts. Ath (lethal) n=61 of 107 | p< 0,00000 | p< 0,164 | p< 0,286 | ||||||||
| Female n=170 of 164 versus n=49 of 61 | p< 0,00036 | p< 0,258 | p< 0,386 | ||||||||
| Male n=64 of 164 versus n=12 of 61 | p< 0,001 | p< 0,348 | p< 0,652 | ||||||||
| RA pts. n=234 versus pts. Ath (associated) n=45 of 107 | p< 0,003 | p< 0,003 | p< 0,047 | ||||||||
| Female n=170 of 164 versus n=7 of 45 | p< 0,022 | p< 0,079 | p< 0,283 | ||||||||
| Male n=64 of 164 versus n=2 of 45 | p< 0,063 | p< 0,017 | p< 0,014 | ||||||||
| RA pts. n=234 versus pts. with HT n=41 of 234 | p< 0,055 | p< 0,517 | p< 0,062 |
- Female n=170 of 164 versus n=29 of 41 p< 0,191 p< 0,249 p< 0,050
- Male n=64 of 164 versus n=12 of 41 p< 0,125 p< 0,471 p< 0,900
- RA pts. n=234 versus pts. with Tb n=28 of 234 p< 0,212 p< 0,242 p< 0,867
- Female n=170 of 164 versus n=21 of 28 p< 0,193 p< 0,280 p< 0,970
- Male n=64 of 164 versus n=7 of 28 p< 0,920 p< 0,678 p< 0,686
- RA pts. n=234 versus pts. with mTb n=9 of 234 p< 0,634 p< 0,033 p< 0,020
- Female n=170 of 164 versus n=8 of 9 p< 0,708 p< 0,050 p< 0,040
- Male n=64 of 164 versus n=1 of 9
- -
- -
- -
- RA pts. n=234 versus pts. with mTu n=27 of 234 p< 0,832 p< 0,269 p< 0,116
- Female n=170 of 164 versus n=19 of 27 p< 0,545 p< 0,654 p< 0,091
- Male n=64 of 164 versus n=8 of 27 p< 0,157 p< 0,115 p< 0,892
- RA pts. n=234 versus pts. with AV n=43 of 234 p< 0,285 p< 0,037 p< 0,165
- Female n=170 of 164 versus n=26 of 43 p< 0,304 p< 0,022 p< 0,230
- Male n=64 of 164 versus n=17 of 43 p< 0,715 p< 0,630 p< 0,604
- RA pts. n=234 versus pts. with AV (lethal) n=24 of 234 p< 0,348 p< 0,629 p< 0,410
- Female n=170 of 164 versus n=15 of 24 p< 0,713 p< 0,356 p< 0, 404
- Male n=64 of 164 versus n=9 of 24 p< 0,201 p< 0,793 p< 0,821
- RA pts. n=234 versus pts. with AAa n=48 of 234 p< 0,281 p< 0,149 p< 0,159
- Female n=170 of 164 versus n=38 of 48 p< 0,572 p< 0,307 p< 0,256
- Male n=64 of 164 versus n=10 of 48 p< 0,354 p< 0,368 p< 0,489
- RA pts. n=234 versus pts. with AAa (lethal) n=20 of 234 p< 0,032 p< 0,049 p< 0,311
- Female n=170 of 164 versus n=13 of 20 p< 0,082 p< 0,085 p< 0,354
- Male n=64 of 164 versus n=7 of 20 p< 0,194 p< 0,338 p< 0,573
- RA pts. n=234 versus pts. with CI n=15 of 234 p< 0,923 p< 0,397 p< 0,269
- Female n=170 of 164 versus n=9 of 15 p< 0,405 p< 0,189 p< 0,614
- Male n=64 of 164 versus n=6 of 15 p< 0,687 p< 0,746 p< 0,153
- RA pts. n=234 versus pts. with SI n=33 of 234 p< 0,028 p< 0,449 p< 0,491
- Female n=170 of 164 versus n=23 of 33 p< 0,031 p< 559 p< 0,366
- Male n=64 of 164 versus n=10 of 33 p< 0,579 p< 0,589 p< 0,733
- RA pts. n=234 versus pts. with PA n=15 of 234 p< 0,004 p< 0,049 p< 0,606
- Female n=170 of 164 versus n=10 of 15 p< 0,005 p< 0,115 p< 0,791
- Male n=64 of 164 versus n=5 of 15 p< 0,337 p< 0,267 p< 0,522
- RA pts. n=234 versus pts. with SV n=7 of 234 p< 0,196 p< 0,982 p< 0,279
- Female n=170 of 164 versus n=4 of 7 p< 0,121 p< 0,582 p< 0,588
- Male n=64 of 164 versus n=3 of 7 p< 0,672 p< 0,193 p< 0,221
Table 3: Statistical correlations (“p” values of significance) between female and male RA patients associated with DM, Ath,
Ath (n=107) accompanied AV in 12, AV (lethal) in 4, AAa in 12, AAa (lethal) in 4, CI in 5, SI in 9, PA in 3, SV in none of 107 patients. The relationship between Ath and Ath with lethal outcome (n=61) went together AV in 3 and AAa in none of 61 patients. The relationship between Ath (with lethal outcome) and AV or AAa was inverse and significant (Table 3). In other words Ath (lethal) was not associated with AV (lethal), AAa (lethal), CI, SI, PA or SV (since a patient may have only one cause of death; the links were inverse and usually significant (Table 3).
HT (n=41) occurred with AV in 4, AV (lethal) in 2, AAa in 8, AAa (lethal) in 3, CI in 2, SI in 3, PA in 1, SV in none of 41 patients.
Tb (n=28) coexisted with AV in 9, AV (lethal) in 5, AAa in 2, AAa (lethal) in none, CI in 3, SI in 5, PA in 1, SV in 1 of 28 patients.
mTb (n=9) accompanied AV in 4, AV (lethal) in 4, AAa in 2, AAa (lethal) in none, CI in 1, SI in 2, PA in none, SV in 1 of 9 patients. There was a positive and significant correlation between Tb and AV (χ²=4.0188, p<0.04) or mTb and AV (χ²=4.2406, p<0.03) (Table 3). There was a The statistical links (“p” values of significance) between allied disorders and prevalence or mortality of RA related complications are summarized in Table 3. *asterisk indicates a negative value of associations’ coefficient with inverse relationship.
very close connection between mTb and mortality of AVas well (χ²=11.88, p<0.0005).
mTu (n=27) was observed with AV in 1, AAa in 4, CI in 1, SI in 3, PA in 1, SV in none of 27 patients.
The links between allied disorders and the most important complications of RA, apart from the above mentioned positive and significant relationship of Tb and mTb, were in most cases not significant and mainly inverse.
| Ath | Ath | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Allied disorders in | HT 41 of | Tb 28 of | mTb 9 | mTu 27 | |||||||||||||||||||
| DM 41 of 234 | n=107 of | (lethal) | |||||||||||||||||||||
| RA | 234 | 234 | of 28 | of 234 | |||||||||||||||||||
| 234 | n=61 | ||||||||||||||||||||||
| Complications of RA | |||||||||||||||||||||||
| AV n=43 of 234 | ²p | ² p | ² p | ² p | ² p | ² p | ² p | ||||||||||||||||
| AV lethal n=24 of 43 | ²p | ² p | ² p | ² p | ² p | ² p | ² p | ||||||||||||||||
| AAa n=48 of 234 | ²p | ² p | ² p | ² p | ² p | ² p | ² p | ||||||||||||||||
| AAa lethal n =24 of 48 | ²p | ² p | ² p | ² p | ² p | ² p | ² p | ||||||||||||||||
| CI n=15 of 234 | ²p | ² p | ² p | ² p | ² p | ² p | ² p | ||||||||||||||||
| SI n=33 of 234 | ²p | ² p | ² p | ² p | ² p | ² p | ² p | ||||||||||||||||
| PA n=15 of 33 | ²p | ² p | ² p | ² p | ² p | ² p | ² p | ||||||||||||||||
| SV n=7 of 33 | ²p | ² p | ² p | ² p | ² p | ² p | ² p |
Table 4: The statistical links (“p” values of significance) between allied disorders and prevalence or mortality of RA related co
Table 3: The statistical links (“p” values of significance) between allied disorders and prevalence or mortality of RA related complications. Glossary to Table 3: RA: Rheumatoid Arthritis n=234 Ath: Atherosclerosis n=107 of 234, with lethal outcome n=61 of 107 HT: HyperTension n=41 of 234 DM: adult type 2 Diabetes Mellitus n=41 of 234 Tb: Tuberculosis n=28 of 234 mTb: Tuberculosis with miliary dissemination n=9 of 234 mTu: malignantTumour n=27 of 234 AV: systemic Autoimmune Vasculitis n=43 of 234, with lethal outcome n=24 of 43 AAa: AA amyloidosis n=48 of 234, with lethal outcome n=20 of 48
CI: Cardiac Iinsufficiency caused exclusively by endo-, myo- or pancarditis n=15 of 234 SI: Lethal Septic Infection n=33 of 234 SV: systemic Septic Vasculitis n=7 of 33 PA: Purulent Arthritis n=15 of 33 The most important RA related complications and comorbidities are demonstrated in Figures 1-10 including but not limited to all possibilities.
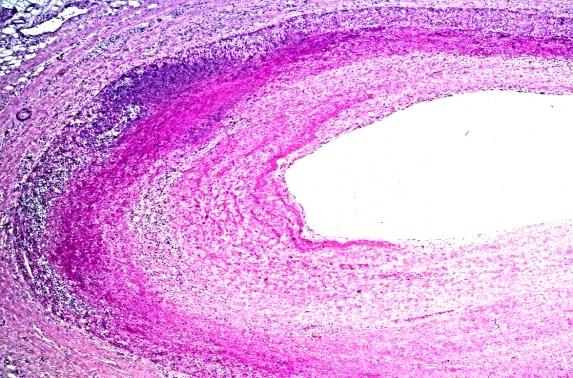
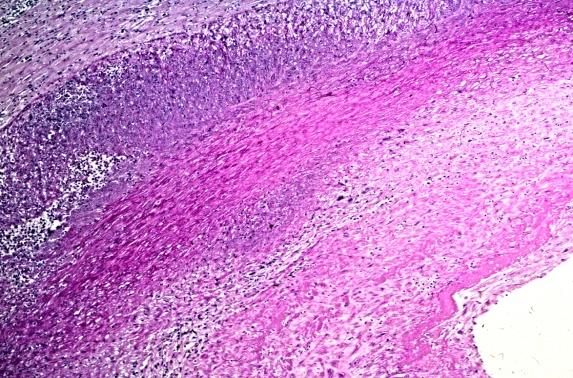
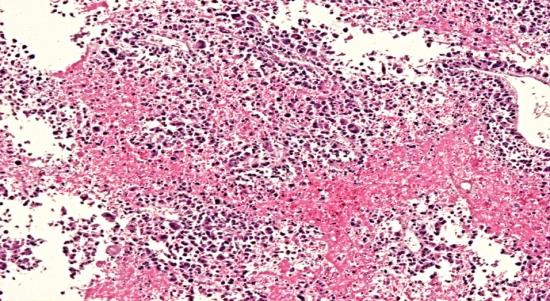
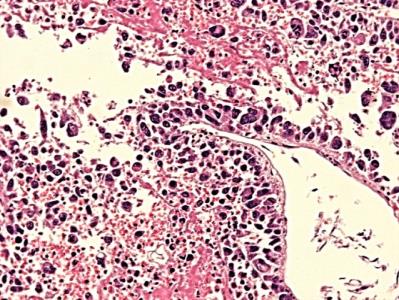
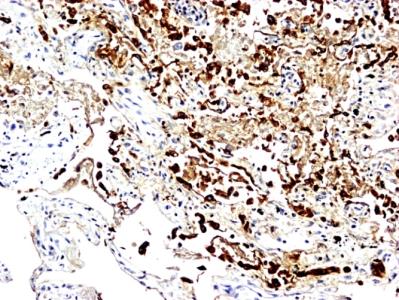
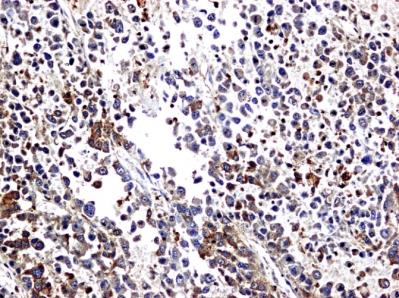
Figures 1-3 show different types and stages of autoimmune coronary vasculitis, Figures 4-5 early and late stages of amyloid a deposition in adrenal gland, Figures 6-7 fibrocaseous and exudative mTb, and Figures
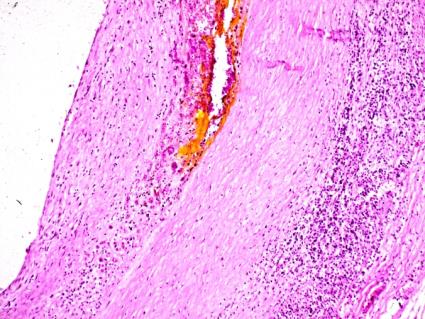
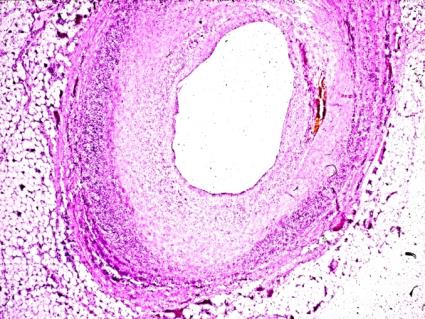
8-10 the most frequent mTu (bronchoalveolar carcinoma) in RA.
Original magnifications correspond to the 24x36 mm transparency slide; the correct height: width ratio is 2:3. The printed size may be different; therefore it is necessary to indicate the original magnifications.
a b
a b
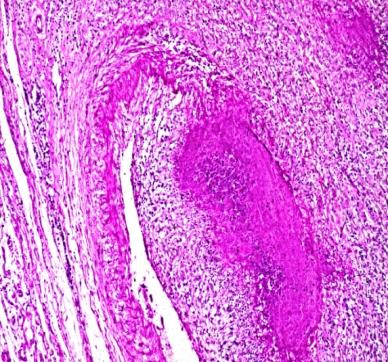
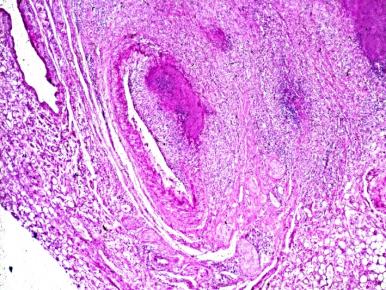
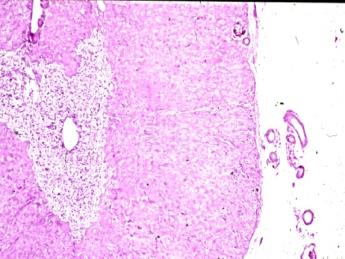
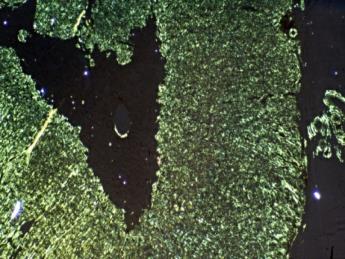
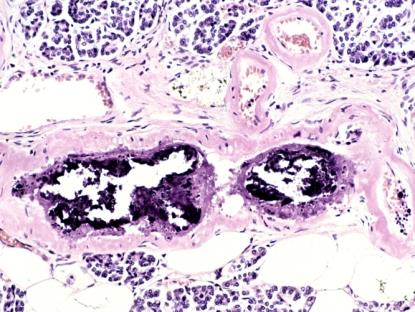
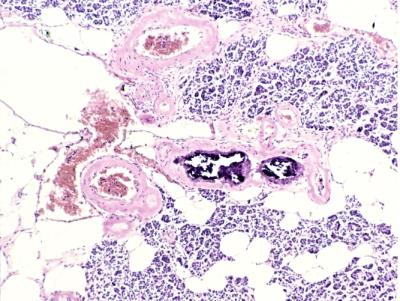
Figure 4: RA, adrenal gland and periadrenal fat tissue, early stage of systemic secondary AA amyloidosis Amyloid A deposited within reticular zone of adrenal gland, in the wall of periadrenal blood vessels (arterioles) and along reticular and collagen fibers. (a) HE, x 50, (b) same as (a) Congo red staining, without alcoholic differentiation, covered with gum arabic. Viewed under polarized light x50
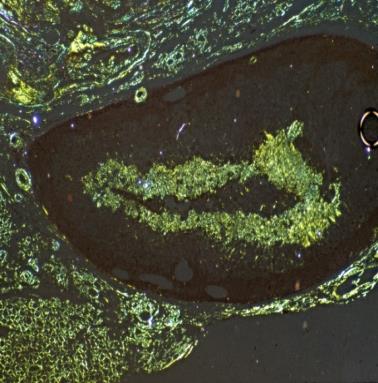
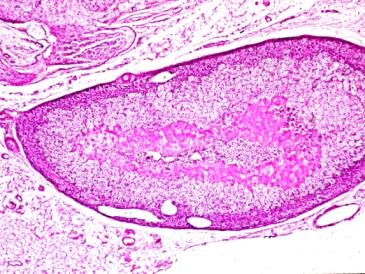
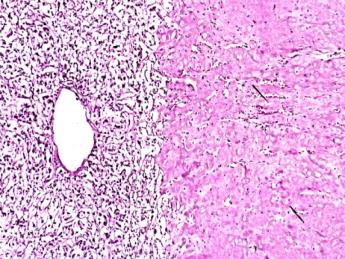
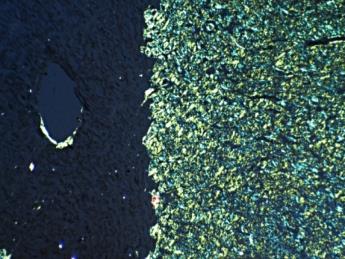
Figure 5: RA, adrenal gland and periadrenal fat tissue, late stage of systemic secondary AA amyloidosis Amyloid A deposited within the reticular, fascicular and glomerular zones of adrenal cortex, involving periadrenal blood vessels, reticular and collagen fibers (a) HE, x 50, (b) same as (a) x125, (c) same as Figure (a) Congo red staining viewed under polarized light, x50, (d) same as Figure (b and c) Congo red staining viewed under polarized light, x125
a b
a b
a b
c d
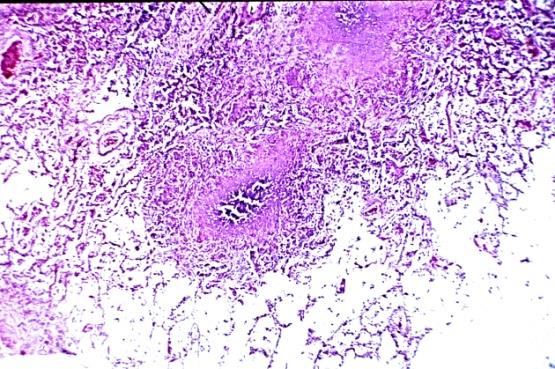
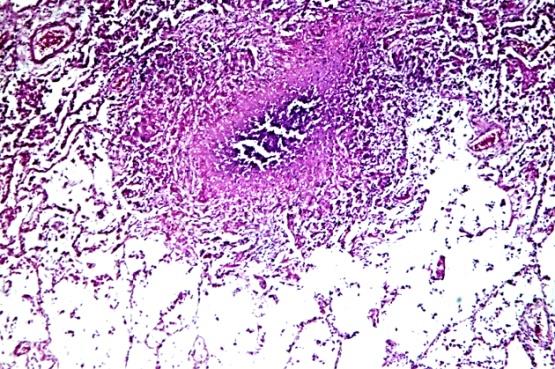
a b Figure 6: RA, miliary disseminated caseous tuberculosis in the lung (a) HE, x 50, (b) same as (a) x125
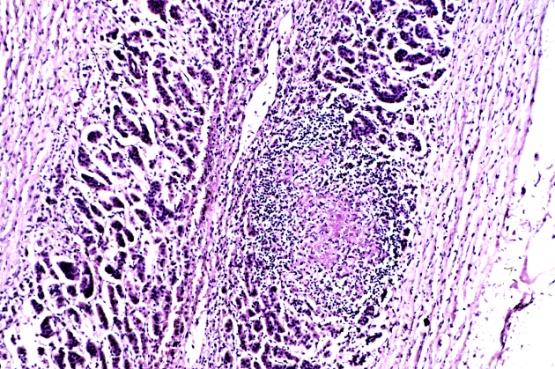
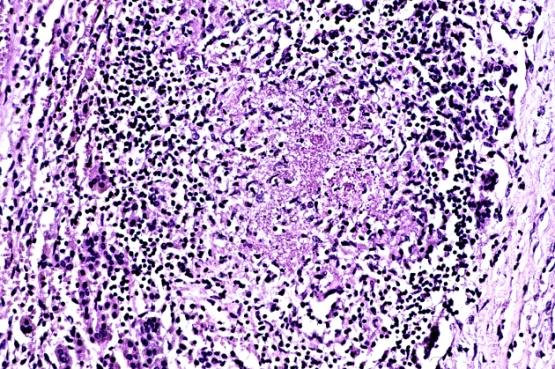
a b Figure 7: RA, exudative miliary epithelioid granulomas in atrophic suprarenal gland (a) HE, x 50, (b) same as (a) x125
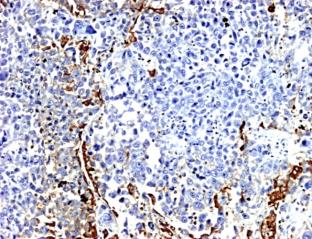
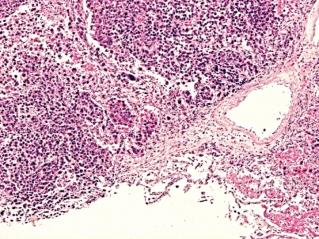
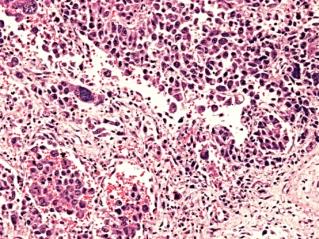
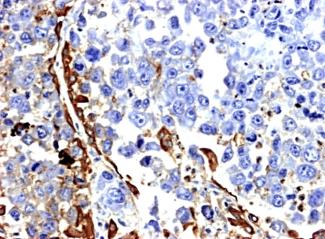
a b c d Figure 8: RA, lung, undifferentiated bronchoalveolar carcinoma Irregular spaces separated by fibrotic septa, and enveloped by tall partly columnar epithelium (a) HE, x 40, (b) same as (a) x100, (c) Anti-human epithelial membrane antigen (mono/DAKO N1504), x 100 (d) same as (c) x200
a b
c d
a b Figure 10: RA, DM, pancreas, severe atherosclerosis involving small arteries (a) HE, x 50, (b) same as (a) x125
Discussion
Severe atherosclerosis was present nearly in half, in 107 (45.72%) of 234 RA patients, and led to death in more than half 61 (57.01%) of them. Ath was the most important allied disorder leading to death in RA.
The mean age of atherosclerotic female and male RA patients was higher than the mean age of the others or of the total population, and RA started consequently later in these patients. RA associated with Ath may represent a special subgroup of RA patients with a better prognosis, which may correspond to the clinically benign elderly- onset or late-onset RA [11]. The negative correlations between allied disorders and RA related complications represent an inverse relationship between them. The high prevalence of allied disorder suggests a rarer (less common) occurrence of RA related complication. Ath with lethal outcome surmises an especially lower risk for RA related complications (AV, AV lethal, AAa, AAa lethal, CI, SI or PA), based on the strong and significant but negative correlations between them. With other words, the most important complications of RA are presumably less frequent in atherosclerotic RA patients.
The negative correlation between Ath and CI shows that cardiac insufficiency in our patients’ group was caused by endo-, myo-, epi- or pancarditis, and polyserositis with or without interstitial pneumonitis, which complicated RA earlier and in younger patients (without prominent atherosclerosis).
The lower mean age of RA patients complicated by lethal AAa (56.80 years versus 66.25; p< 0.032) and the early onset of disease (40.33 years versus 51.02; p< 0.049) in these patients indicate also, that the most dangerous complications of RA involve mainly the younger generation, which was also supported by the strong negative and significant correlations to Ath (χ=5.83*, p<0.01) or to Ath with lethal outcome (χ²=6.30*, p<0.01).
Septic complication including PA led to early death of the patients (SI: 62.33 and PA: 59.47 years versus 66.25; p< 0.028 and p< 0.004), which also showed a distinct difference in women (SI: 61.35 and PA: 58.20 years versus 66.31; p< 0.031 and p< 0.005). The strong negative and significant relationship between Ath and SI(χ=5.27*, p<0.02) or PA (χ²=3.23*, p<0.07 – NS), and between Ath with lethal outcome and SI (χ=12.05*, p<0.0005) or PA(χ=4.29*, p<0.03) referred again to the explicit involvement of younger people.
Diabetes and hypertension are the basic risk factors of atherosclerosis and its complications. DM and HT raise the prevalence of Ath, cardiovascular diseases, limited renal function, progressive endothelial dysfunction, higher intraocular pressure, decreased erectile function etc. independently from each other, and the risk of these increases in case of coexistence [12, 13, 14].
According to our data mTu did not influence the prevalence and mortality of RA related complications. The prevalence and mortality of malignant tumors in pertinent literature and our RA autopsy population is summarized in Table 4.
According to the literature, DM is often associated with HT, and it is also mentioned in several studies as an evidence statement [15, 16, 17, 18]. According to our data DM, HT or Ath did not influece the prevalence and mortality of RA related complications, and the clinically well controlled DM or HT does not diminish the chances of survival.
Tuberculosis is one of the most important associated diseases accompanying RA [3]. The positive and significant correlation between Tb and AV (χ²=4.02, p< 0.04) or mTb and AV (χ²=4.24, p< 0.03) suggest a positive role of tuberculosis on the prevalence and mortality of autoimmune vasculitis in RA. The presence of Tb (especially of its fibrocaseous form) or endogenous exacerbation and miliary dissemination of tuberculosis (mTb) increases, promotes, and facilitates the risk of AV and modifies the histological type of vasculitis [19, 20]. The significant connection between mTb and mortality of AV (χ²=11.88, p< 0.0005) means an increased risk of lethal outcome. This statement was also supported by the late and collateral (parallel) onset of RA in patients with mTb (59.38 years versus 51.02; p< 0.033) and AV (56.85 years versus 51.02; p< 0.037) compared these to the total population. The tendency was the same and especially pronounced in females with mTb (58.71 years versus 50.46; p< 0.033) and with AV (58.04 years versus 50.46; p< 0.022).
Published data indicate that the overall risk of malignancy (especially prevalence of lymphomas and lung cancer) is higher in RA, compared with the general population [21, 22]. According to Buchbinder, et al. the incidence of malignancy was low in an Australian RA patients’ cohort and anti-tumour necrosis factor treatment did not increase the risk of malignancy. Only the incidence of melanoma increased in comparison with the general population [23].
| Tumor | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Authors | Year of Publication-[References] | No of Autopsy | Prevalence | Mortality | ||||||||||
| N - % | N - % of Total | |||||||||||||
| Bayles | 1943 [24] | 23 | ND | 2 of 23– 8.7% | ||||||||||
| Baggenstoss and Rosenberg | 1943 [25] | 30 | ND | 1 of 30– 3.3% | ||||||||||
| Young and Schwedel | 1944 [26] | 33 | ND | 2 of 33– 6.1% | ||||||||||
| Bywaters | 1950 [27] | 27 | ND | 4 of 27– 14.8% | ||||||||||
| Gedda | 1955 [28] | 45 | ND | 1 of 45 – 2.2% |
Table 5: Literature on the morbidity and mortality of malignant tumors in autopsied RA patients. Glossary to Table 4 ND: no data
| Goehrs, et al. | 1960 [29] | 36 | ND | 4 of 36– 11.1% |
|---|---|---|---|---|
| Lebowitz | 1963 [30] | 62 | ND | 6of 62– 9.7% |
| Gardner | 1972 [31] | 142 | 24 – 16.9% | ND |
| Vroninks, et al. | 1973 [32] | 62 | ND | 7 of 62– 11.3% |
| Rainer, et al. | 1978 [33] | 79 | ND | 2 of 79 – 2.53% |
| Lindahl | 1984 [34] | 82 | ND | 3 of 82 – 3.7% |
| Suzuki, et al. | 1994 [35] | 81 | ND | 5 of 81 – 6.2% |
| Bély and Apáthy | 1998 [36] | 161 | 13 – 8.1% | 7 of 13 – 4.4% |
| Bély and Apáthy | 2003 [37] | 161* | 15 – 9.3% | 7 of 15 – 4.4% |
| Bély and Apáthy | 2005 [38] | 234* | 27 – 11.5% | 12 of 27 – 6.4% |
Table 6: Literature on the morbidity and mortality of malignant tumors in autopsied RA patients. Glossary to Table 4 ND: no data
Conclusion
The consequently inverse and (in most cases) significant correlation between atherosclerosis and autoimmune vasculitis, amyloidosis or sepsis shows that the prevalence or mortality of AV, AAa and SI was not influenced by Ath. RA patients with Ath may represent a special group, characterized by lower incidence of SV, AAa, SI, CI, and carry a better prognosis. Ath is basically an age- dependent phenomenon, characteristically present in RA patients with advanced age, while AV, AAa (with or without lethal outcome) and SI are complications of RA, and characterize severe forms of disease, mostly in younger patients and with an earlier onset (without pronounced atherosclerosis).
The positive and significant correlation between Tb and AV (χ²=4.02, p < 0.04) or mTb and AV (χ²=4.24, p < 0.03) suggest a positive influence of Tb or mTb on the prevalence of vasculitis, e.g. the presence of Tb or endogenous exacerbation and miliary dissemination of Tb may promote the AV; and modify the histological type of vasculitis [19, 20]. The significant connection between mTb and mortality of AV (χ²=11.88, p< 0.0005) indicates an increased risk of lethal outcome.
Finalizing the results of interaction between coexistent allied disorders and complications of RA it may be concluded that there is a more or less close link between them. The knowledge of these complications and the likelihood of their occurrence should be considered when management, particularly therapeutic decisions are made: “one sees what one knows”.
References
-
Jeong H, Baek SY, Kim SW, Eun YH, Kim IY, et al. (2017) Correction: Comorbidities of rheumatoid arthritis: Results from the Korean National Health and Nutrition Examination Survey. PLoS One 12(5): e0178309.
-
Van den Hoek J, Boshuizen HC, Roorda LD, Tijhuis GJ, Nurmohamed MT, et al. (2017) Mortality in patients with rheumatoid arthritis: a 15-year prospective cohort study. Rheumatol Int 37(4): 487-493.
-
Bély M, Ágnes A (2013) Clinical pathology of rheumatoid arthritis: Cause of death, lethal complications and associated diseases in rheumatoid arthritis, pp: 1-440.
-
Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, et al. (1988) The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 31(3): 315- 324.
-
Lentner C (1982) “Statistical methods”. In Geigy scientific tables, 8th revised and enlarged ed: Ciba- Geigy Limited, Basle, Switzerland, 2: 227.
-
Bély M, Apáthy Á (2017) Myocardial necrosis caused by systemic vasculitis or atherosclerosis in rheumatoid arthritis-A postmortem clinicopathologic study of 161 patients. EC Cardiology 3(3): 74-91.
-
Apáthy Á, Bély M (2016) AB0528 Organ Involvement with Systemic Vasculitis of Autoimmune and of Septic Origin-A Comparative Postmortem Study of 38 Rheumatoid Arthritis Patients. Annals of the Rheumatic Diseases 75(S2): 1096.
-
Romhányi G (1971) Selective differentiation between amyloid and connective tissue structures based on the collagen specific topo-optical staining reaction with Congo red. Virchows Arch A Pathol Pathol Anat 354(3): 209-22.
-
Bély M, Makovitzky J (2006) Sensitivity and specificity of Congo red staining according to Romhányi- Comparison with Puchtler's or Bennhold's methods. Acta Histochemica 108(3): 175-180.
-
Bély M (2006) Histochemical differential diagnosis and polarization optical analysis of amyloid and amyloidosis. ScientificWorldJournal 6: 154-68.
-
Der Sarkissian C (2017) What You Need to Know About Elderly-Onset RA. WebMD Medical Reference, Reviewed by Carol DerSarkissian.
-
Park HY, Schumock GT, Pickard AS, Akhras K (2003) A structured review of the relationship between microalbuminuria and cardiovascular events in patients with diabetes mellitus and hypertension. Pharmacotherapy 23(12): 1611-1616.
-
Preik M, Kelm M, Rosen P, Tschope D, Strauer BE (2000) Additive effect of coexistent type 2 diabetes and arterial hypertension on endothelial dysfunction in resistance arteries of human forearm vasculature. Angiology 51(7): 545-554.
-
Hennis A, Wu SY, Nemesure B, Leske MC (2003) Hypertension, diabetes, and longitudinal changes in intraocular pressure. Ophthalmology 110(5): 908- 914.
-
Basile JN, Lackland DT, Basile JM, Riehle JE, Egan BM (2004) A statewide primary care approach to cardiovascular risk factor control in high-risk diabetic and nondiabetic patients with hypertension. Journal of Clinical Hypertension 6(1): 18-25.
-
Bouhanick B, Laboureau Soares BS, Marre M (2000) Hypertension and diabetes. Archives des maladies du coeur et des vaisseaux 93: 1429-1434.
-
Sowers JR, Epstein M, Frohlich ED (2001) Diabetes, hypertension, and cardiovascular disease: an update. Hypertension 37(4): 1053-1059.
-
El Atat F, McFarlane SI, Sowers JR (2004) Diabetes, hypertension, and cardiovascular derangements: pathophysiology and management. Curr Hyperten Rep 6(3): 215-223.
-
Bély M, Apáthy Á (2013) AB0644 Mortality of tuberculosis in rheumatoid arthritis-a retrospective clinicopathologic study of 234 autopsy patients. Annals of the Rheumatic Diseases 72(S3): A986-A986.
-
Apáthy Á, Bély M (2013) THU0437 Disease Modifying Effect of Tuberculosis on Coexistent Systemic Vasculitis in Rheumatoid Arthritis-A Retrospective Clinicopathologic Study of 234 Autopsy Patients. Annals of the Rheumatic Diseases 72(S3): A312.
-
Smitten AL, Simon TA, Hochberg MC, Suissa S (2008) A meta-analysis of the incidence of malignancy in adult patients with rheumatoid arthritis. Arthritis Res Ther 10(2): R45.
-
Simon TA, Thompson A, Gandhi KK, Hochberg MC, Suissa S (2015) Incidence of malignancy in adult patients with rheumatoid arthritis: a meta-analysis. Arthritis Res Ther 17: 212.
-
Buchbinder R, Van Doornum S, Staples M, Lassere M, March L (2015) Malignancy risk in Australian rheumatoid arthritis patients treated with anti- tumour necrosis factor therapy: analysis of the Australian Rheumatology Association Database (ARAD) prospective cohort study. BMC Musculoskelet Disord 16: 309.
-
Bayles TB (1943) Rheumatoid arthritis and rheumatic heart disease in autopsied cases. American Journal of Medical Sciences 205: 42-48.
-
Baggenstoss AH, Rosenberg EF (1943) Visceral lesions associated with chronic infectious (rheumatoid) arthritis. Archives of Pathology 35: 503-516.
-
Young D, Schwedel JB (1944) The heart in rheumatoid arthritis. American Heart Journal 28(1): 1-23.
-
Bywaters EGL (1950) The relation between heart and joint disease including “rheumatoid heart disease” and chronic post-rheumatic arthritis (type Jaccoud). Br Heart J 12(2): 101-131.
-
Gedda PO (1955) On amyloidosis and other causes of death in Rlicurnatoid arthritis. Acta Medica Scandinavica 150(6): 443-452.
-
Goehrs HR, Baggenstoss AH, Slocumb CH (1960) Cardiac lesions in rheumatoid arthritis. Arthritis and Rheumatism 3: 298-308.
-
Lebowitz WB (1963) The heart in rheumatoid arthritis (Rheumatoid disease). A clinical and pathological study of sixty-two cases. Annals of Internal Medicine 58: 102-123.
-
Gardner DL (1972) The pathology of rheumatoid arthritis. In: Edward Arnold, (Ed.), Causes of death, pp: 183-197.
-
Vroninks Ph, Cats A, Eulderink F, Goslinks J (1973) Heart defects in rheumatoid arthritis, in particular pericarditis. Nederlands Tijdschrift voor Geneeskunde 117: 10-17.
-
Rainer F, Klein G, Schmid P, Härringer M (1978) Untersuchungen über Art und Häufigkeit der Todesursachen bei chronischer Polyarthritis. Zeitschrift für Rheumatologie 37: 335-341.
-
Lindahl BI (1984) The reliability of Swedish mortality statistics for rheumatoid arthritis. Scandinavian Journal of Rheumatology 13(4): 289-296.
-
Suzuki A, Ohosone Y, Obana M, Mita S, Matsuoka Y, et al. (1994) Cause of death in 81 autopsied patients with rheumatoid arthritis. Journal of Rheumatology 21(1): 33-36.
-
Bély M, Apáthy Á (1998) Daganatos megbetegedések rheumatoid arthritisben. Orvosi Hetilap 139: 2567- 2574.
-
Bély M, Apáthy Á (2004) Tumors in reumatoid arthritis-A retrospective clinicopathologic study of 161 autopsy patients. Annals of the Rheumatic Diseases 63(S1): 539.
-
Apáthy Á, Bély M (2004) Clinical and laboratory parameters, demographics and duration of disease associated with benign and malignant tumors in rheumatoid arthritis-A retrospective clinicopathologic study of 161 autopsy patients. Annals of the Rheumatic Diseases 63(1): 167-168.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results