Rib-Based Anchors are Associated with Proximal Translational Deformity in Early Onset Spinal Deformity Patients undergoing Growth-Friendly Surgical Treatment
Objective/Background: No studies to date have evaluated the the effect of rib-based anchors on the translational relationship between the rib and spine. We hypothesized that there would be an increase in the translational distance between the rib anchor and anterior vertebral body in early onset spinal deformity patients managed with long-term rib-based anchors. Methods: All patients with EOSD from a single tertiary level institution treated with a growth-friendly technique surgery utilizing proximal rib-based anchors from 2006-2015 with a minimum of 2-year follow-up were included. Thoracic kyphosis and the translational distance from the rib anchor to the corresponding anterior vertebral body were measured. Results: Twenty-seven patients (13 female, 14 male) qualified for inclusion. Mean age at implantation of the index proximal rib-based construct was 5±1.9 years (range, 1-9). EOSD etiology was congenital: 3, neuromuscular: 17, syndromic: 3, and idiopathic: 4. Mean kyphosis improved from 31±33° preoperatively to 25±20° immediately post-operatively. No significant changes in kyphosis were noted over 1 and 2 year follow-up (p=0.3). Twenty-one (78%) patients demonstrated an increase in translational distance from the rib anchors to the adjacent anterior vertebral body. Immediately post-operatively, mean distance was 25±1 mm and increased at 1-year (26±1 mm) and significantly at 2-year (29±1 mm) follow-up (p=0.005). Conclusion: The use of long term rib-based anchors may lead to an increase in the distance between the rib utilized for proximal fixation and the associated vertebral body, generating what appears to be increased anterior translation of the spine. This translation, in conjunction with increased or increasing overall thoracic kyphosis, may be the source of unexpected obstacles at the time of future surgical procedures for revision or final fusion
Introduction
Early Onset Spinal Deformity (EOSD) is characterized by abnormal curvature of the spine greater than 10° before the age of 10 years [1]. Due to the risk of progressive spinal deformity with growth, EOSD may be associated with coronal or sagittal imbalance, and/or compromised pulmonary function [2]. The management of EOSD is challenging, with treatment options consisting of casting, bracing, or “growth-friendly” fusionless constructs, such as spine-based traditional growing rods (TGR), or rib-based constructs, which include the Vertical Expandable Prosthetic Titanium Rib (VEPTR, Synthes, Paoli, PA) [3].
Complications associated with the management of EOSD with growth-friendly constructs are well documented in the literature. These include wound dehiscence and surgical site infection following multiple lengthening operations [4, 5], and proximal rib fractures associated with rib-based anchors [5]. Furthermore, increased thoracic kyphosis often seen in EOSD patients can be worsened by posterior-based distraction systems [6, 7, 8, 9]. Anedoctal clinical findings noted during the care of EOSD patients with proximal rib-based anchors led the authors to believe that long term use of these implants appears to potentiate the apparent proximal thoracic kyphosis in surgically treated patients. No studies to date have evaluated the the effect of a rib-based anchor on the relationship between the rib and adjacent anterior spine.
The primary purpose of this study was to determine the effect of rib-based anchors on the distance between the proximal anchor rib/ribs and the anterior vertebral body of the spine at the same level. We hypothesized that over time rib-based anchors would be associated with an increase in distance between the rib anchor point and the associated anterior vertebral body. Such an increase may act to magnify the existing thoracic kyphosis. The combination of kyphosis and anterior spinal translation may lead to difficulties with exposure of posterior elements of the proximal thoracic spine at the time of future surgical procedures.
Methods
Following Institutional Review Board approval, a retrospective review of all patients aged 0-18 with a diagnosis of EOSD from a single tertiary level institution treated with growth-friendly posterior surgery was performed. Inclusion criteria included use of proximal rib anchors, a minimum of 2-year follow-up, and representative radiographs pre- operatively, post-operatively, and at 1-year and 2-year follow-up. Exclusion criteria consisted of patients who underwent a fusion procedure as the index procedure or within the 2-year follow-up from the initial growth friendly implantation, as well as those with incomplete radiographic records. Demographic data including age, sex, and diagnosis was retrieved from the electronic medical record.
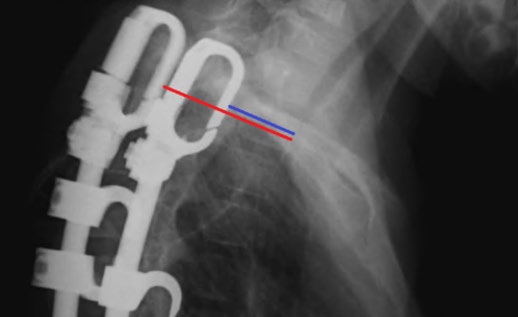
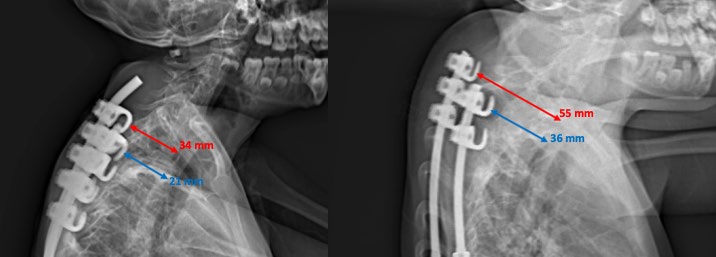
Radiographic assessment was conducted using IMPAX (AGFA; Mortsel, Belgium). Thoracic kyphosis, measured from the superior end plates of T1 and T12, was assessed on upright lateral images obtained pre-operatively, immediately post-operatively, and at 1 and 2-year follow-up. The distance from the anterior aspect of the rib hook to the corresponding anterior vertebral body cortex was measured and termed the “Translational Distance” (Figure 1). This distance was assessed on upright lateral images obtained immediately post-operatively and at 1- and 2-year follow-up. All measurements were performed by members of the research group who were not directly involved in the surgical or clinical care of the patients included in the study. Computerized tomography (CT) of the proximal implants were obtained on a very limited number of patients, and for that reason were not part of the analysis. Clinical variables for this study included age, gender and EOSD etiology. Data analysis consisted of a repeated measures ANOVA with pairwise comparison for mean kyphosis and translational distance. Statistics were generated using IBM SPSS Statistics-v24.
Results
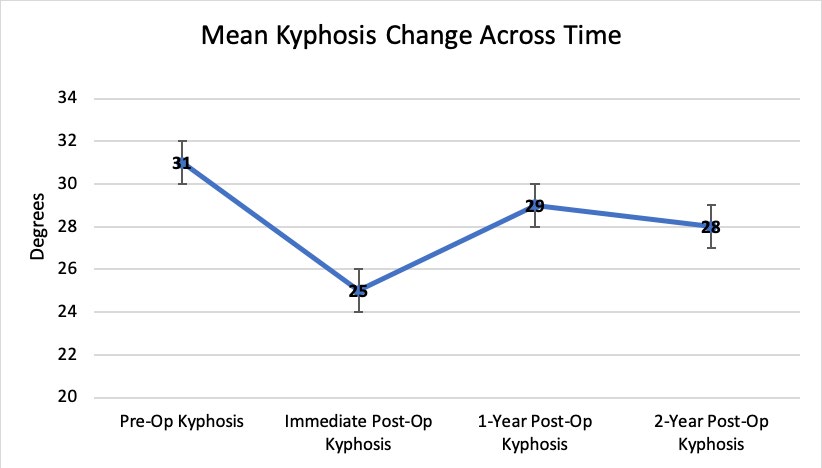
Twenty-seven patients qualified for inclusion in the study (13 female, 14 male) with a mean average age at proximal rib-based construct implantation of 5 years (range, 1y-9y). Etiologies of EOSD included congenital 11% (n=3), neuromuscular 62% (n=17), syndromic 11% (n=3), and idiopathic 15% (n=4). The mean and standard deviation for sagittal angular kyphosis across time are presented in Table
1 and Figure 2. Pairwise comparisons for mean kyphosis at any time point did not show significance (p>0.05).
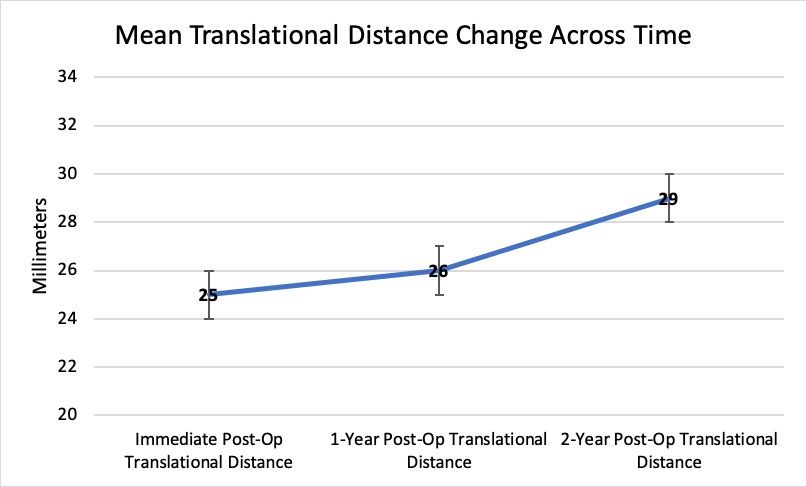
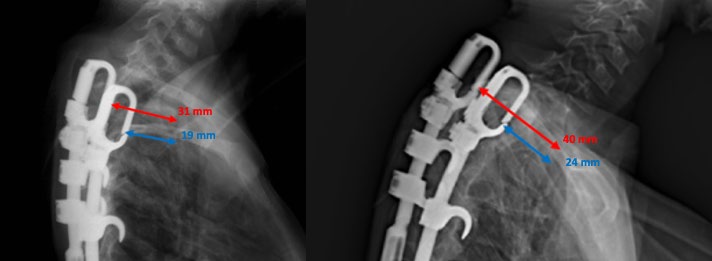
Twenty-one (78%) patients demonstrated an increase in translational distance from the rib anchors to the anterior vertebral body over the follow-up period. Change in mean translational distance and standard deviation over time are presented in Table 1 and Figure 3. Representative radiographs highlighting this increase in mean translational distance are shown in Figures 4 and 5. Pairwise comparisons of translational distance showed statistically significant increases between immediate post-op and 2-year follow-up radiographs (p=0.001), as well as between 1-year and 2-year follow-up (p=0.005) (Table 1).
| Mean and Standard Deviation | p value | |
|---|---|---|
| Pre-Op Kyphosis (deg.) | 31°±33° | -- |
| Immediate Post-Op Kyphosis (deg.) | 25°±20° | 0.995 |
| 1-Year Post-Op Kyphosis (deg.) | 29°±25° | 0.539 |
| 2-Year Post-Op Kyphosis (deg.) | 28°±23° | 1 |
| Immediate Post-Op Translational Distance (mm) | 25±1 | -- |
| Immediate Post-Op Translational Distance (mm) | 25±1 | -- |
| 1-year Post-Op Translational Distance (mm) | 26±1 | 0.732 |
| 2-year Post-Op Translational Distance (mm) | 29±1 | 0.005 |
Table 1: Mean and standard deviation of measured kyphosis and translational distance following initial operation.
Discussion
Distraction-based, posterior non-fusion techniques are utilized frequently in the surgical management of EOSD.
Each consist of proximal and distal anchors attached to the spine or ribs which connect with an expandable rod. Following implantation, periodic lengthening procedures are performed to control deformity progression and promote continued spinal growth. During the time period in which this patient cohort underwent surgical management for EOSD, the most frequently used rib-based device in growth- friendly spine constructs was the Vertical Expandable Prosthetic Titanium Rib (VEPTR). Other rib-based systems generally include the use of standard transverse process or laminar hooks. Although VEPTR use was limited originally to patients with EOSD associated with fused ribs, recent reports have validated the efficacy of VEPTR in a diverse group of patients with and without chest wall abnormalities [7, 10]. Studies have demonstrated a range of effects of the VEPTR device on pulmonary function in EOSD patients, from improvement in vital capacity to decreased deterioration of overall pulmonary status [8].
Rib-based cradles that are part of the VEPTR system were utilized commonly for the surgical management of EOSD in the authors’ practices from 2006 until approximately 2015 when other devices became available. This was particularly true for those patients who were felt to benefit from proximal rib fixation at part of a fusionless, growth-friendly construct. The authors tended to use rib fixation proximally rather than spine anchors in patients younger than 7 years of age who either failed nonoperative management of EOSD or presented with a deformity or physical limitations that precluded attempted casting or bracing.
As the authors followed this cohort of EOSD patients with proximal rib fixation, it became clinically and radiographically apparent that many patients developed increased proximal thoracic deformity over time. At the termination of the growth-friendly treatment, the majority of these patients underwent definitive instrumented spinal fusion, colloquially referred to as “graduation” in the literature [11, 12]. While performing the exposure of the posterior thoracic spine in many of our patients at the time of final fusion, the actual proximal thoracic deformity appeared to be clinically greater than that expected and planned for based on the proximal kyphosis measured on preoperative imaging. The combination of underlying proximal kyphosis and associated rib prominence appeared to generate an anatomic deformity that often caused significant difficulties with both surgical exposure of the proximal spine and final implant placement.
In this patient cohort, implantation of a growth-friendly posterior device with proximal rib fixation led to a reduction in radiographic thoracic kyphosis immediately following the index procedure. This finding of initial reduction in kyphosis confirms the results of Gantner, et al. [13], who reported an
11° improvement in kyphosis following VEPTR implantation. Despite an immediate reduction in angular kyphosis at the time of the index procedure, our results demonstrate a modest increase in thoracic kyphosis over time, which is comparable to other reports of EOSD patients managed with VEPTR [7, 8].
In contrast to these previously well-described findings regarding thoracic kyphosis, the unique aspect of this study was the investigation into changes in the distance from the proximal rib fixation point and the anterior aspect of the adjacent vertebral body (Translational Distance). Review of the lateral radiographic images demonstrated a statistically significant increase in the measured distance both at 2-year post op versus immediately post index procedure, as well as between 1- and 2-year post-implantation. To our knowledge, no previous investigators have assessed the relationship between the rib anchors and the spine itself in patients with long-term proximal rib fixation. Specifically how and why this increased rib-to-vertbral body distance occurs is unclear. We propose that these changes are most likely the result of mobility of the rib at the costovertebral junction in combination with gradual ploughing of the device and subsequent remodeling of the ribs during the period of distraction.
Regardless of the etiology, rib-based proximal anchors appear to alter the relationship between the point of rib fixation and the adjacent spine. Use of proximal rib- based anchors are associated with significantly increased translational distance between the point of rib fixation and the anterior cortex of the associated vertebral body when comparing immediate post-operative images to those at 2-year follow-up. From a clinical and anatomic standpoint, this secondary deformity seems to potentiate the effect of the proximal thoracic kyphosis. This combination of deformities appears to become most problematic at the time of implant revision surgery or during conversion of an existing posterior growing construct to a final fusion.
There are several limitations to this study, including those inherent to retrospective reviews. A relatively small cohort of patients was available for analysis, which limited the statistical power of this study. Because this was a single institution study, standardization of radiographic technique and patient positioning was a goal in all cases. However, due to the variability in patients’ mobility and physical characteristics, true standardization may have been compromised.
In addition, the authors acknowledge the potential role that progressive spinal rotation may have played in altering the relationship between the rib cradle and the adjacent anterior vertebral body as viewed with standard radiographs. Computerized Tomography evaluations of the proximal ribs and the associated rib cradles may have provided more detailed information. However, these were obtained infrequently in this cohort so as to limit overall radiation exposure, and never in a sequential fashion.
These results demonstrate that the use of rib-based anchors may lead to an increase in distance, between the rib utilized for proximal fixation and the associated vertebral body, generating radiographic evidence of increasing anterior translation of the spine at that level. This radiographic finding, in conjunction with inherent or increasing proximal thoracic kyphosis, may lead to unforeseen anatomic alterations, which may be a source of unexpected surgical difficulties at the time of revision or final fusion procedures. Awareness and appreciation of this potential deformity pre-operatively may prove valuable to those involved in the later surgical care of an already complicated patient population.
Acknowledgement
No funding or support was sought or gained for the purposes of design, implementation, or preparation of this work. There was no pharmaceutical and industry support that requires acknowledgment.
There was no support from any of the following organizations: National Institutes of Health (NIH); Wellcome Trust; Howard Hughes Medical Institute (HHMI); and other(s).
References
-
Skaggs D, Tenner J Guillaume, Smith J, Ron El-Hawary, John Emans, et al. (2015) Early Onset Scoliosis Consensus Statement, SRS Growing Spine Committee, 2015. Spine Deformity 3(2): 107.
-
Yang S, Lindsay M Andras, Gregory J Redding, David L Skaggs (2016) Early-Onset Scoliosis: A Review of History, Current Treatment, and Future Directions. Pediatrics 137(1): e20150709.
-
Yazici M, Emans J (2009) Fusionless instrumentation systems for congenital scoliosis: expandable spinal rods and vertical expandable prosthetic titanium rib in the management of congenital spine deformities in the growing child. Spine (Phila Pa 1976) 34(17): 1800-1807.
-
Garg S, Jaren La Greca, Tricia St Hilaire, Dexiang Gao, Michael Glotzbecker, et al., (2014) Wound complications of vertical expandable prosthetic titanium rib incisions. Spine (Phila Pa 1976) 39(13): E777-E781.
-
Dayer R, Ceroni D, Lascombes P (2014) Treatment of congenital thoracic scoliosis with associated rib fusions using VEPTR expansion thoracostomy: a surgical technique. Eur Spine J 23(S4): S424-S431.
-
Schroerlucke SR, Behrooz A Akbarnia, Jeff B Pawelek, Pooria Salari, Gregory M Mundis, et al. (2012) How does thoracic kyphosis affect patient outcomes in growing rod surgery? Spine (Phila Pa 1976) 37(15): 1303-1309.
-
Murphy RF, Alice Moisan, Derek M Kelly, William C Warner, Tamekia L Jones, et al. (2016) Use of Vertical Expandable Prosthetic Titanium Rib (VEPTR) in the Treatment of Congenital Scoliosis Without Fused Ribs. J Pediatr Orthop 36(4): 329-335.
-
Dede O, Etsuro K Motoyama, Charles I Yang, Rebecca L Mutich, Stephen A Walczak, et al. (2014) Pulmonary and Radiographic Outcomes of VEPTR (Vertical Expandable Prosthetic Titanium Rib) Treatment in Early-Onset Scoliosis. J Bone Joint Surg Am 96(15): 1295-1302.
-
Reinker K, James W Simmons, Vishwas Patil, Zachary Stinson (2010) Can VEPTR® Control Progression of Early-onset Kyphoscoliosis?: A Cohort Study of VEPTR® Patients With Severe Kyphoscoliosis. Clinical orthopaedics and related research 469(5): 1342-1348.
-
Emans JB, Jean François Caubet, Claudia L Ordonez, Edward Y Lee, Michelle Ciarlo (2005) The treatment of spine and chest wall deformities with fused ribs by expansion thoracostomy and insertion of vertical expandable prosthetic titanium rib: growth of thoracic spine and improvement of lung volumes. Spine (Phila Pa 1976) 30(17): 58-68.
-
Murphy RF, Mark A Pacult, William R Barfield, Richard H Gross, James F Mooney (2019) Experience with definitive instrumented final fusion after posterior- based distraction lengthening in patients with early- onset spinal deformity: single center results. J Pediatr Orthop B 28(1): 10-16.
-
Flynn JM, Lauren A Tomlinson, Jeff Pawelek, George H Thompson, Richard McCarthy, et al. (2013) Growing-rod graduates: lessons learned from ninety-nine patients who completed lengthening. J Bone Joint Surg Am 95(19): 1745-1750.
-
Gantner AS, Lena Braunschweig, Konstantinos Tsaknakis, Heiko M Lorenz, Anna K Hell (2018) Spinal deformity changes in children with long-term vertical expandable prosthetic titanium rib treatment. Spine J 18(4): 567- 574.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results