Approach to the Treatment of Diabetic Foot Osteomyelitis- Insertion of Bioactive BONALIVE Via Plantar Approach and Consequently External Fixation for Diabetic Foot Osteomyelitis: A Case Report
Diabetic foot osteomyelitis (DFO) is a clinical problem with a high risk of amputation, and it is always a complication of a preexisting infected foot wound. Prevalence can be as high as 60%. There is no consensus in the current literature regarding the management of these patients and this remains an unsolved challenge for the case manager. Surgical therapy, antibiotic therapy, or conservative treatment are among the current common treatments. Each one of them has its inherent advantage and disadvantages. In the past few years, Bioactive and soluble glasses have had the potential for use in wound healing and infection eradication. The use of new bone substitutes aims to support the load of the bone segments and to ensure the eradication of the infectious process. The approach to the infection is also a challenge. We present the management of a case of DFO that has been treated by systemic antibiotics and the insertion of bioglass, Bonalive, via plantar approach and additional external fixation. This novel way of treatment allows the closure of a diabetic ulcer that was already planned for below-knee amputation (BKA) in other institutions. A long follow-up shows the resolution of the infectious process, no ulcer recurrence, and persistent recovery of the ability to walk. Our results are in line with current literature that suggests bioglass may be considered a useful option to manage DFO and achieve healing with a very conservative approach.
Introduction
Diabetic ulcers disperse on the foot, About 15% on the forefoot [1, 2]. They are very difficult to treat, It involves offloading and the end-staged wound closure, fixations treatment, stabilization, and convalescence.
The common surgical approach is dorsal, since a lot of surgeons consider plantar approach problematic due to the scar which can harm the soft tissue under it. Since we had a huge sore on the plantar surface which reached the bone infection, we have been forced to use the plantar approach.
Moreover, In critical cases like this patient it is quite common to consider BKA amputation as a radical treatment, and this was suggested to the patient in another institution.
Patient information
A 50-year-old male, worked as jeweler, married with 3 children, doesn’t smoke nor keeping healthy diet. His past medical history included Gout Arthritis, Osteomyelitis, Uncontrolled diabetes, and kidney disease. He came to our department with a plantar ulcer on the right foot (Figure 1). The lateral ray was excised previously

Materials and Method
Offloading consisted of a non-walking regime.
CT scan, probing and technetium bone scan Showed infection penetrating through the tibial, sesamoid and mp1 joint.
We choose to do an unconventional plantar incision [3], the Sesamoid was amputated, infected joint was debrided, Cultures were taken [4] and were positive for Enterobacter cloacae complex, and started taking IV antibiotic FLAGYL, INVANZ treatment.
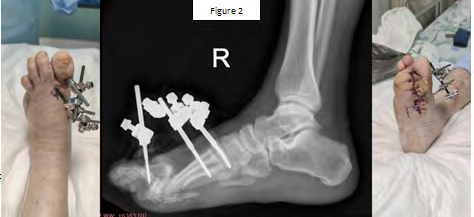
We also planted Bonalive bioglass [5], an artificial bone substitute, promoting bone consolidation and preventing infection due to the low PH (acidity) of the substitute, stabilization was made by X-fixation with biplanar system (figure 2).
Shortly afterwards X-fixation the was removed and we put plaster of Paris for 3 weeks.
After 10 weeks of treatment, the wound was closed. Following consolidation on x-ray the patient was suggested an insole.
Conclusions
Forefoot MP1 ulcer is difficult for treatment, one needs the whole picture of infection to treat the pathogen. While nowadays many advocates for other approaches, in present case a plantar wound with sesamoid and Mp1 joint osteomyelitis drives us to plantar approach which is described well in older literature [2, 3, 6]. We also used anterior rocker shoe to offload the foot [7, 8].
Infections can be treated by systemic antibiotic and bioglass, and biplanar External fixators provide good alternative for fixation.
References
-
Mohammadi MS, Stähli C, Nazhat SN (2011) Bioactive glasses for wound healing. In Bioactive Glasses (pp246- 266).
-
Prissel MA, Hyer CF, Donovan JK, Quisno AL (2017) Plantar Plate Repair Using a Direct Plantar Approach: An Outcomes Analysis. J Foot Ankle Surg 56(3): 434-439.
-
Tillmann K (1997) Surgery of the Rheumatoid Forefoot with Special Reference to the Plantar Approach. Clin Orthop Relat Res 340: 39-47.
-
Pinzur MS (2016) Surgical treatment of the Charcot foot. Diabetes Metab Res Rev 32(S1): 287-291.
-
Gurumurthy B, Tucci MA, Fan LW, Benghuzzi HA, Pal P, et al. (2020) Collagen-Elastin-Like Polypeptide-Bioglass Scaffolds for Guided Bone Regeneration. Adv Healthc Mater 9(4): e1901385.
-
McAlister JE, Hyer CF (2013) The Direct Plantar Plate Repair Technique. Foot Ankle Spec 6(6): 446-451.
-
Bajuri MY, Ong SL, Das S, Mohamed IN (2022) Charcot Neuroarthropathy: Current Surgical Management and Update A Systematic Review. Front Surg 9: 820826.
-
Panunzi A, Giurato L, Meloni M, Uccioli L (2022) Bioactive Glass in a Multi Drug Resistance Osteomyelitis in Diabetic Foot: Case Report. Int J Low Extrem Wound National Library of Medicine: (pp15347346221102643).
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results