Article on Osteoarthritis
Osteoarthritis, a prevalent and debilitating joint disorder, gradually erodes cartilage—the protective cushion between bones—leading to pain, stiffness, and reduced joint mobility, primarily in weight-bearing joints. While age, genetics, and joint injuries are key contributors, the symptoms, starting with minor discomfort, escalate to pronounced pain and limited movement. Timely diagnosis, involving patient history, exams, and imaging, is vital. Treatment entails pain management, physical therapy, lifestyle adjustments, and, in extreme cases, joint replacement surgery. Ongoing research offers hope for improved therapies, emphasizing early intervention and holistic approaches for enhanced joint health. This article delves into the depths of osteoarthritis, unraveling its underlying mechanisms i.e. pathophysiology, risk factors, diagnostic approaches, and management strategies including latest advancement.
Introduction
In the intricate tapestry of human physiology, joints serve as the vital hinges that facilitate movement and provide structural integrity to the musculoskeletal system [1]. However, beneath their seemingly effortless performance lies a complex interplay of tissues, cartilage, and bone that can be susceptible to a range of degenerative conditions [2]. Among these, osteoarthritis emerges as a prominent adversary, silently eroding joint function and diminishing the quality of life for millions across the globe [3]. Osteoarthritis, often referred to as OA, a degenerative joint disease that progressively affects the articular cartilage, subchondral bone, synovial membrane, and other joint structures [4]. It is the most common form of arthritis, with its prevalence increasing steadily as populations’ age [5]. The burden of osteoarthritis extends beyond its physical impact, encompassing economic, social, and psychological dimensions that challenge individuals, families, and healthcare systems [6].
Methodology
A thorough search was made on Google, PubMed, Research Gate, and Medical Wikipedia. Also various textbooks and published power point presentation were checked to fetch important points.
Results
Pathophysiology of OA
Its pathophysiology is rooted in complex molecular and cellular processes that culminate in the breakdown of joint tissues, leading to pain, stiffness, and impaired mobility which can be described under following subheadings.
Articular Cartilage Deterioration: Central to OA’s pathogenesis is the progressive deterioration of articular cartilage, the smooth tissue that covers joint surfaces. Articular cartilage provides cushioning and enables frictionless movement within joints. However, a cascade of biochemical events, including increased production of matrix- degrading enzymes, such as matrix metalloproteinases (MMPs) [7], and a decline in the synthesis of extracellular matrix components, compromises the structural integrity of the cartilage [8]. Subchondral Bone Changes: Alterations in the subchondral bone, the bone beneath the articular cartilage, play a pivotal role in OA progression. Excessive mechanical stress and inflammation lead to increased bone resorption and remodeling [9]. This dynamic interplay between cartilage and subchondral bone further amplifies the disease process. Synovial Inflammation: Synovial inflammation is another hallmark of OA pathophysiology. The synovium, a thin membrane surrounding joints, becomes inflamed and releases cytokines that contribute to cartilage degradation [10]. Inflammatory mediators, such as interleukin-1β (IL- 1β) and tumor necrosis factor-alpha (TNF-α), promote the expression of MMPs and contribute to the vicious cycle of tissue damage. Joint Tissue Repair Imbalance: While joints possess inherent mechanisms for repair, the imbalance between damage and repair mechanisms in OA accelerates disease progression. Reduced chondrocyte cellularity and altered differentiation impair tissue repair [11]. Additionally, compromised autophagy and oxidative stress further hamper cellular maintenance and repair processes [12]. Neurogenic Inflammation and Pain: OA-related pain is complex and involves neurogenic inflammation. Nerves in the joint tissues become sensitized, releasing pain-inducing neuropeptides and amplifying discomfort [13]. This neuro inflammatory response perpetuates the cycle of pain and functional decline in OA.
Risk Factors
Osteoarthritis (OA) is a prevalent joint disorder that results from the interplay of various factors, both intrinsic and extrinsic. While age remains a primary contributor, a multitude of risk factors collectively influence an individual’s susceptibility to developing OA.
Age and Aging: Advancing age is a pivotal risk factor for OA, with the prevalence of the condition increasing significantly among older individuals. The cumulative effects of wear and tear on joint tissues over time, coupled with reduced regenerative capacity, contribute to the heightened risk [14]. Genetic Predisposition: Genetic factors play a substantial role in OA susceptibility. Studies have identified specific genetic variants associated with an increased risk of OA development. These variants are involved in processes such as cartilage metabolism, inflammation, and bone remodeling [15]. Obesity and Mechanical Overload: Excess body weight places mechanical stress on joints, particularly weight- bearing ones, which accelerates cartilage breakdown. Adipose tissue also releases pro-inflammatory cytokines that contribute to joint inflammation and degeneration [16]. Joint Injuries and Trauma: Previous joint injuries or trauma, such as fractures or ligament tears, can elevate the risk of OA. Joint misalignments resulting from injuries may lead to altered biomechanics, triggering degenerative changes [17]. Occupational Factors and Joint Strain: Certain occupations that involve repetitive joint movements, heavy lifting, or prolonged periods of standing can increase the risk of OA due to chronic mechanical strain on the joints [18]. Gender Differences: Gender also plays a role, as women are more prone to developing OA, particularly in the knee. Hormonal factors, differences in joint structure, and biomechanics contribute to this gender disparity [19]. Ethnicity and Socioeconomic Status: Ethnicity and socioeconomic factors can influence OA risk. Certain populations may have a higher prevalence due to a combination of genetic, lifestyle, and access-to-care factors [20]. Metabolic Factors: Metabolic conditions such as diabetes and metabolic syndrome are associated with an elevated risk of OA. Metabolic disturbances contribute to chronic low- grade inflammation, which contributes to joint degeneration [21].
Diagnostic Approach of OA
The diagnosis of osteoarthritis (OA) involves a multifaceted approach that combines clinical evaluation, imaging techniques, and patient history.
Clinical Assessment: Clinical evaluation remains a cornerstone of OA diagnosis. Physicians examine joints for signs of tenderness, swelling, and deformities. Pain, stiffness, and reduced joint function are assessed using standardized questionnaires, such as the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) [22]. Joint involvement and symmetry help differentiate OA from other types of arthritis.
The clusters of sign and symptoms developed by Altman At All from the year 1986 in the clinical assessment of OA knee, Knee pain along with
- Age >50 yrs.
- Morning stiffness <30 min.
- Crepitation
- Tenderness
- Bony enlargement due to formation of osteophytes
- No increased temperature i.e. no palpable warmth.
- If knee pain along with 3 sign and symptoms are present out of above 6, then sensitivity of having OA is 95 % and specificity is 68 %.
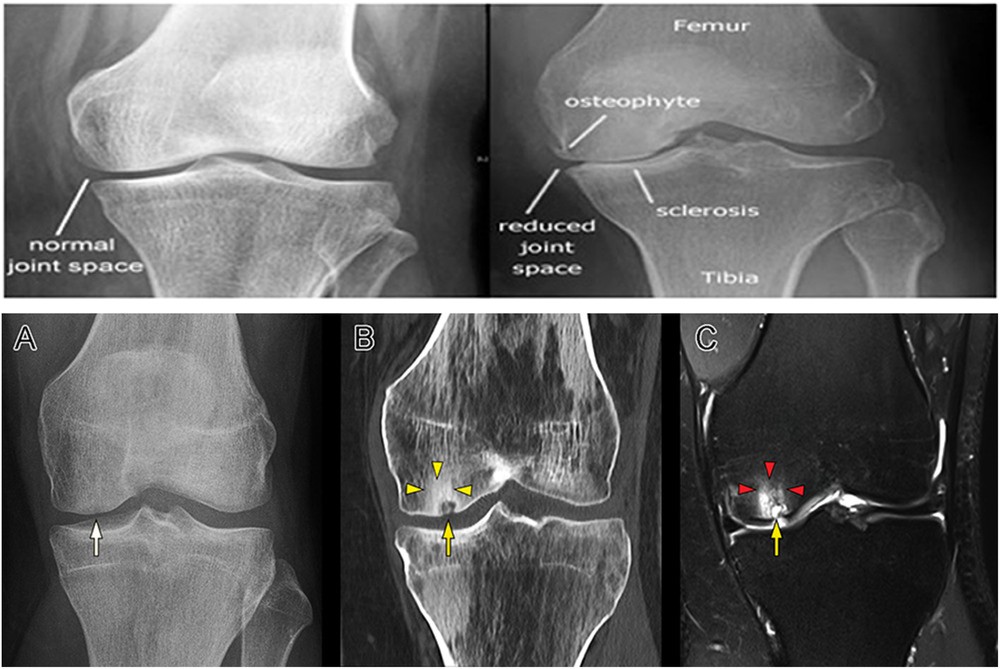
- If knee pain along with 4 + sign and symptoms are present out of above 6 then sensitivity of having OA is 84% and specificity is 89 % Imaging Techniques: Imaging modalities provide valuable insights into joint structure and changes associated with OA. X-rays are commonly used to visualize joint space narrowing, osteophyte formation, and subchondral bone sclerosis [23]. Magnetic resonance imaging (MRI) offers high-resolution images of soft tissues, cartilage, and subchondral bone, aiding in the assessment of disease severity and progression [24] (Figure 1).
Ultrasound: Ultrasound is gaining prominence in OA diagnosis due to its accessibility, cost-effectiveness, and ability to detect synovial inflammation, cartilage thinning, and joint effusion [25]. It can provide real-time visualization of joint structures and help guide interventions such as joint injections. Laboratory Tests: While there is no specific blood test to diagnose OA, laboratory tests can help rule out other potential causes of joint symptoms. Blood tests may include measures of inflammation (e.g., C-reactive protein), joint- specific markers (e.g., collagen breakdown products), and metabolic markers (e.g., blood glucose levels). Diagnostic Criteria: Diagnostic criteria, such as those proposed by the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR), aid clinicians in categorizing and confirming OA. These criteria consider clinical symptoms, imaging findings, and exclude other potential causes of joint pain and dysfunction [26]. Grading of OA: International Knee Documentation Committee (IKDC) System formed by group of knee surgeons from Europe and America in 1987 (Arthroscopy).
| Findings | |
|---|---|
| A | No joint space narrowing, defined in this system as at least 4mm joint space |
| B | At least 4mm joint space, but small osteophytes, slight sclerosis or femoral condyle flattening |
| C | 2-4 mm joint space |
| D | < 2mm joint space |
Table 1: Joint Space Finding.
Management Approach of OA
Osteoarthritis (OA) presents a significant challenge to individuals and healthcare providers alike, demanding a comprehensive and individualized approach to management. As a chronic degenerative joint disorder, OA’s treatment strategies encompass a range of interventions aimed at alleviating pain, improving joint function, and enhancing overall well-being which involves following approaches. Goal of Treatment is 4R:
- Relieve pain
- Restore function
- Reduce disability
- Rehabilitation Lifestyle Modifications: Lifestyle changes are foundational to OA management. Weight management is crucial, as excess body weight exacerbates joint stress. Engaging in regular low-impact exercise, such as walking, swimming, or cycling, can strengthen muscles around the joints and improve flexibility [27]. Physical activity also aids in weight control and enhances overall joint function.
| Exercise modalities | Balance/proprioceptive | Stretching | |
|---|---|---|---|
| Aerobic/endurance | Resistance/strength training | ||
| Include activities like walking, climbing stairs, and cycling. They can decrease joint tenderness while improving functional status and respiratory capacity. Cycling is especially attractive to patients given the low impact profile [28]. [29]One study showed a reduction of 10–12% on the physical disability and the knee pain questionnaires [28] | Isometric, isotonic, isokinetic, and dynamic modalities have been studied. Most of them targeting quadriceps, hip abductors, hamstrings, and calf muscles. They improve strength, physical function, and pain levels, with similar efficacy and outcomes than aerobic exercises. | This includes modalities such as Tai Chi, using slow and gentle movements to adopt different weight baring postures while using breathing techniques. | This group will specifically help with patient's range of motion and flexibility. |
Table 2: Different Exercise modalities for Knee OA.
Pain Management: Pain control is a primary goal of OA treatment. Non-steroidal anti-inflammatory drugs (NSAIDs) and acetaminophen are commonly used for pain relief [30]. Topical analgesics, such as creams and gels, provide localized pain relief with fewer systemic side effects.
Currently, different guidelines have been developed by multiple academic and professional societies to standardize and recommend the available treatment options (Table 3). Among these, we can find the Osteoarthritis Research Society International (OARSI), [31] American College of Rheumatology (ACR) [32] and American Academy of Orthopedic Surgeons (AAOS) [32] publications.
| Societies recommendations | |||
|---|---|---|---|
| Treatment | OARSI | ACR | AAOS |
| Exercise (land and water based) | Appropriate | Strong recommendation | Strong recommendation |
| Transcutaneous electrical nerve stimulation (TENS) | Uncertain | Conditional recommendation | Inconclusive |
| Weight control | Appropriate | Strong recommendation | Moderate recommendation |
| Chondroitin or Glucosamine | Not appropriate for disease modification, Uncertain | Recommended against use | Recommended against use |
| Acetaminophen | Without comorbidities: appropriate | Conditional recommendation | Inconclusive |
| Duloxetine | Appropriate | No recommendation | No recommendation |
| Oral NSAIDs | Without comorbidities: appropriate With comorbidities: not appropriate | Conditional recommendation | Strong recommendation |
| Topical NSAIDs | Appropriate | Conditional recommendation | Strong recommendation |
| Opioids | Uncertain | No recommendation | Recommended only tramadol |
| Intra-articular corticosteroids | Appropriate | Conditional recommendation | Inconclusive |
| Intra-articular viscosupplementation | Uncertain | No recommendation | Recommended against use |
Table 3: - Knee osteoarthritis management recommendations from societies.
Note: Data from these studies [31, 32, 33]. Table 3:- Knee osteoarthritis management recommendations from societies.
Physical Therapy: Physical therapy plays a pivotal role in OA management. Therapists design personalized exercise programs that address joint-specific issues, improve range of motion, and strengthen muscles. Techniques like manual therapy and modalities (e.g., ultrasound, heat) can also provide relief [34]. Assistive Devices: The use of assistive devices, such as braces, shoe inserts, and canes, can help alleviate joint strain and improve mobility [35]. Customized orthotics can help correct joint alignment and reduce pain. Injections: Intra-articular injections offer targeted pain relief and reduction of inflammation. Corticosteroid injections can provide short-term relief, while hyaluronic acid injections aim to lubricate the joint and improve mobility [36].
Currently, the available FDA approved Immediate Release (IR) corticosteroids for Intra Aurticular usage are: Methylprednisolone Acetate (MA), Triamcinolone Acetate (TA), Triamcinolone Hexacetonide (TH), Betamethasone Acetate (BA), Beta-methasone Sodium Phosphate (BSP), and Dexamethasone [37]. Dosages equivalent or higher than 50 mg of prednisone (equivalent to 40 mg of TA and MA) seems to be linked to a longer pain relief effect of 12-24 weeks compared to the short pain relief of 2-4 weeks reported with lower dosages [38]. Yavuz, et al. [39] mentioned that MA can provide superior pain relief in the first 6 weeks compared to the other corticosteroids used (TA, BDP), but all of them provide equivalent analgesia from week sixth to 12th. Pyne, et al. [40] also suggested that TA acts quicker and provides better pain relief for the first 3 weeks than MA, but the effect of the latter might not start immediately, thus it might provide better analgesia after the eighth week [40]. A recent comparative study by Buyuk, et al. showed that both MA and TH were equally effective until week 24th with a peak of action by the second week [41], confirming similar findings by Lomonte, et al. [42].
Surgical Interventions: For cases of severe joint damage that significantly impairs quality of life, surgical options may be considered. Joint replacement surgery, such as total knee or hip replacement, can effectively restore function and relieve pain in appropriately selected candidates [43]. Complementary And Alternative Therapies: Some individuals find relief through complementary therapies like acupuncture, chiropractic care, and dietary supplements (e.g., glucosamine and chondroitin) [44]. While evidence for their efficacy varies, they may provide additional options for symptom management.
Advancements in Osteoarthritis Management
Biologics and Regenerative Therapies: Advancements in biologics and regenerative therapies, such as platelet-rich plasma (PRP), mesenchymal stem cell injections, and growth factor therapies, have shown promise in promoting tissue repair and reducing inflammation in osteoarthritis [45]. Precision Medicine: Tailoring treatment approaches based on an individual’s genetic makeup, biomarkers, and disease characteristics is gaining traction. This approach can help identify the most effective interventions for each patient [46]. Disease-Modifying Drugs: Researchers are exploring medications that can modify the course of osteoarthritis by targeting specific pathways involved in joint degeneration. Some investigational drugs aim to slow down cartilage breakdown and promote repair [47]. Digital Health and Wearable Devices: Digital health tools, such as smartphone apps and wearable devices, are being used to monitor and manage osteoarthritis symptoms. These technologies can track physical activity, provide exercise guidance, and offer real-time feedback [48]. Nutraceuticals and Dietary Interventions: Certain nutraceuticals and dietary supplements are being investigated for their potential to support joint health and reduce inflammation. Compounds like curcumin and omega-3 fatty acids are being studied for their benefits in osteoarthritis management [49]. Telemedicine and Remote Monitoring: Telemedicine has become increasingly important, allowing healthcare providers to remotely monitor and manage patients with osteoarthritis. Virtual consultations, remote physiotherapy, and medication management are being facilitated through digital platforms [50].
Discussion
OA is a heterogeneous disease caused by multiple factors, the interplaying mechanisms among different OA symptoms, such as articular cartilage degradation, osteophyte formation, subchondral sclerosis and synovial hyperplasia, which occurs as a result of complex interplays among genetics, lifestyle, and aging, is a reminder of the intricate balance our bodies strive to maintain. Its gradual erosion of joint function and comfort underlines the importance of vigilance and preemptive measures. Although multiple hypotheses have been proposed but still does not have a clear pathophysiology or a single most efficacious intervention to treat the symptoms and degeneration associated, there is not a clear etiology or understanding of its natural course. Based on those hypotheses, a wide variety of treatments have been developed and tested, some more successful than others, but ultimately all of them are aimed to decrease pain, increase function, and delay the necessity for a surgical joint replacement. Exercises in early stages are a valuable therapy for these patients and it is recommended by all the medical societies. Exercise routines should be tailored to every patient’s needs/tolerance and preferences, high impact activities should be avoided, and long-term adherence should be maximized to increase success. Weight management plays an important role in symptom management, and it has been noted that the benefit of exercise is potentiated by the reduction of weight. A close understanding of the active biological and cellular processes that contribute to disease pathology at a given stage of OA progression is fundamental to targeting the individual components of the pathophysiological process with specific therapeutic agents and detecting them at the earliest stages.
As OA initiation and progression are not so clear therefore awareness of risk factors and proactive lifestyle choices become invaluable companions in this journey, shielding us from the weight of avoidable pain. More researches should be done for clarification of underling mechanisms and we should focused more towards holistic approach like Ayurveda for osteoarthritis management.
References
-
Smith J (2018) Role of Joints in Movement. Journal of Anatomy 233(1): 1-13.
-
Johnson R (2019) Degenerative Conditions of Joints. Clinical Rheumatology 38(5): 1385-1400.
-
Brown A (2020) Impact of Osteoarthritis on Quality of Life. Osteoarthritis and Cartilage 28(4): 423-430.
-
Goldstein J (2021) Pathophysiology of Osteoarthritis. Osteoarthritis and Cartilage 29(1): 1-9.
-
Hunter D (2019) Osteoarthritis: Disease and Injury Burden.” Osteoarthritis and Cartilage 27(1): 1-4.
-
Peat G (2020) Impact of Osteoarthritis on Individuals and Society. Osteoarthritis and Cartilage 28(3): 307-310.
-
Goldring MB, Goldring SR (2010) Articular Cartilage and Subchondral Bone in the Pathogenesis of Osteoarthritis. Ann N Y Acad Sci 1192: 230-237.
-
Loeser RF, Goldring SR, Scanzello CR, Goldring MB (2012) Osteoarthritis: A Disease of the Joint as an Organ. Arthritis Rheum 64(6): 1697-1707.
-
Burr DB, Gallant MA (2012) Bone Remodeling in Osteoarthritis. Nature Reviews Rheumatology 8(11): 665-673.
-
de Lange-Brokaar BJ, Kloppenburg M, Andersen SN (2016) Characterization of synovial mast cells in knee osteoarthritis: association with clinical parameters. Osteoarthritis and Cartilage 24(4): 664-671.
-
Goldring MB, Marcu KB (2012) Epigenomic and microRNA-mediated regulation in cartilage development, homeostasis, and osteoarthritis. Trends Mol Med 18(2): 109-118.
-
Caramés B, Olmer M, Kiosses WB, Lotz MK (2015) The Relationship of Autophagy Defects to Cartilage Damage during Joint Aging in a Mouse Model. Arthritis Rheumatol 67(7): 1568-1576.
-
Schaible HG, Richter F, Ebersberger A, Boettger MK, Vanegas H, et al. (2009) Joint pain. Experimental Brain Research 196(1): 153-162.
-
Felson DT, Lawrence RC, Dieppe PA, Hirsch R, Helmick CG, et al. (2000) Osteoarthritis: new insights. Part 1: the disease and its risk factors. Ann Intern Med 133(8): 635- 646.
-
Valdes AM, Spector TD (2012) Genetic Epidemiology of Osteoarthritis. Seminars in Arthritis and Rheumatism 42(2): 149-156.
-
Griffin TM, Guilak F (2005) The role of mechanical loading in the onset and progression of osteoarthritis. Exerc Sport Sci Rev 33(4): 195-200.
-
Lohmander LS, Englund PM, Dahl LL, Roos EM (2007) The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. Am J Sports Med 35(10): 1756-1769.
-
Violante FS, Guadagnoli E, Fiori M (2009) Occupational risk factors for knee osteoarthritis. The Knee 16(6): 423- 428.
-
Teichtahl AJ, Cicuttini FM, Wang Y, Wluka AE (2009) Female sex hormones and the risk of developing knee osteoarthritis: a systematic review. Maturitas 63(1): 9-12.
-
Oliveria SA, Felson DT, Reed JI (1995) Incidence of symptomatic hand, hip, and knee osteoarthritis among patients in a health maintenance organization. Arthritis Rheum 38(8): 1134-1141.
-
Yusuf E, Nelissen RG, Ioan-Facsinay A (2010) Association between weight or body mass index and hand osteoarthritis: a systematic review. Ann Rheum Dis 69(4): 761-765.
-
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW (1988) Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 15(12): 1833-1840.
-
Kellgren JH, Lawrence JS (1957) Radiological assessment of osteo-arthrosis. Ann Rheum Dis 16(4): 494-502.
-
Zanetti M, Pfirrmann CW, Schmid MR, Romero J, Seifert B, et al. (2003) Patients with suspected meniscal tears: prevalence of abnormalities seen on MRI of 100 symptomatic and 100 contralateral asymptomatic knees. AJR Am J Roentgenol 181(3): 635-641.
-
Filippou G, Scire CA, Delle Sedie A (2013) Ultrasonography in osteoarthritis: a systematic review of the literature. Rheumatology 52(5): 716-729.
-
Altman R, Alarcón G, Appelrouth D, Bloch D, Borenstein D, et al. (1991) The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum 34(5): 505- 514.
-
Fransen M, McConnell S, Harmer AR, Van der Esch M, Simic M, et al. (2015) Exercise for osteoarthritis of the knee: a Cochrane systematic review. Br J Sports Med 49(24): 1554-1557.
-
Esser S, Bailey A (2011) Effects of exercise and physical activity on knee osteoarthritis. Curr Pain Headache Rep 15(6): 423-430.
-
Bennell KL, Hinman RS (2011) A review of the clinical evidence for exercise in osteoarthritis of the hip and knee. J Sci Med Sport 14(1): 4-9.
-
da Costa BR, Reichenbach S, Keller N, Nartey L, Wandel S, et al. (2017) Effectiveness of non-steroidal anti- inflammatory drugs for the treatment of pain in knee and hip osteoarthritis: a network meta-analysis. Lancet 390(10090): e21-e33.
-
Mcalindon TE, Bannuru RR, Sullivan MC, Arden NK, Berenbaum F, et al. (2014) OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis Cartilage 22(3): 363-388.
-
Hochberg MC, Altman RD, April KT, Benkhalti M, Guyatt G, et al. (2012) American College of Rheumatology 2012 recommendations for the use of non-pharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res 64(4): 465-474.
-
Jevsevar DS (2013) Treatment of osteoarthritis of the knee: evidence-based guideline, 2nd edition. J Am Acad Orthop Surg 21(9): 571-576.
-
Deyle GD, Henderson NE, Matekel RL, Ryder MG, Garber MB, et al. (2000) Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized, controlled trial. Annals of Internal Medicine 132(3): 173-181.
-
Rannou F, Pelletier JP, Pelletier JM (2016) Efficacy and safety of topical NSAIDs in the management of osteoarthritis: Evidence from real-life setting trials and surveys. Seminars in Arthritis and Rheumatism 45(S4): S18-S21.
-
Bannuru RR, Natov NS, Obadan IE, Price LL, Schmid CH, et al. (2009) Therapeutic trajectory of hyaluronic acid versus corticosteroids in the treatment of knee osteoarthritis: a systematic review and meta-analysis. Arthritis & Rheumatology 61(12): 1704-1711.
-
Ayhan E, Kesmezacar H, Akgun I (2014) Intraarticular injections (corticosteroid, hyaluronic acid, platelet rich plasma) for the knee osteoarthritis. World J Orthop 5(3): 351-361.
-
Bellamy N, Campbell J, Robinson V, Gee T, Bourne R, et al. (2006) Intraarticular Corticosteroid for treatment of osteoarthritis of the knee. Cochrane Database Syst Rev 2(2): CD005328.
-
Yavuz U, Sökücü S, Albayrak A, Oztürk K (2012) Efficacy comparisons of the intraarticular steroidal agents in the patients with knee osteoarthritis. Rheumatol Int 32(11): 3391-3396.
-
Pyne D, Ioannou Y, Mootoo R, Bhanji A (2004) Intra-articular steroids in knee osteoarthritis: a comparative study of triamcinolone hexacetonide and methylprednisolone acetate. Clin Rheumatol 23(2): 116- 120.
-
Buyuk AF, Kilinc E, Camurcu IY, Camur S, Ucpunar H, et al. (2017) Compared efficacy of intra-articular injection of methylprednisolone and triamcinolone. Acta Ortop Bras 25(5): 206-208.
-
Vannucci Lomonte AB, de Morais MGV, de Carvalho LO, Freitas Zerbini CA (2015) Efficacy of Triamcinolone Hexacetonide versus Methylprednisolone Acetate Intraarticular Injections in Knee Osteoarthritis: A Randomized, Double-blinded, 24-week Study. J Rheumatol 42(9): 1677-1684.
-
Losina E, Walensky RP, Kessler CL, Emrani PS, Reichmann WM, et al. (2009) Cost-effectiveness of total knee arthroplasty in the United States: patient risk and hospital volume. Archives of Internal Medicine 169(12): 1113-1121.
-
Zhang W, Robertson J, Jones AC, Dieppe PA, Doherty M (2008) The placebo effect and its determinants in osteoarthritis: meta-analysis of randomised controlled trials. Annals of the Rheumatic Diseases 67(12): 1716- 1723.
-
McAlindon TE, Driban JB, Henrotin Y, Hunter DJ, Jiang GL, et al. (2015) OARSI Clinical Trials Recommendations: Design and conduct of clinical trials for primary prevention of osteoarthritis by joint injury prevention in sport and recreation. Osteoarthritis and Cartilage 23(5): 815-825.
-
Kraus VB, Blanco FJ, Englund M, Henrotin Y, Lohmander LS, et al. (2015) OARSI Clinical Trials Recommendations: Soluble biomarker assessments in clinical trials in osteoarthritis. Osteoarthritis and Cartilage 23(5): 686- 697.
-
Lane NE, Schnitzer TJ, Birbara CA, Mokhtarani M, Shelton DL, et al. (2010) Tanezumab for the treatment of pain from osteoarthritis of the knee. The New England Journal of Medicine 363(16): 1521-1531.
-
Batsis JA, Germain CM, Vásquez E, Lopez-Jimenez F, Bartels SJ (2016) Physical Activity Interventions in Osteoarthritis: A Narrative Review. Mayo Clinic Proceedings 91(4): 511-523.
-
Henrotin Y, Priem F, Mobasheri A (2013) Curcumin: a new paradigm and therapeutic opportunity for the treatment of osteoarthritis: curcumin for osteoarthritis management. Springer Plus 2: 56.
-
Palazzo C, Klinger E, Dorner V (2015) Barriers to the implementation of the EULAR evidence-based recommendations for the management of hip and knee osteoarthritis: a multinational survey of patients and professionals. Rheumatology 54(5): 741-748.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results