Prevalence of Intertrochanteric Fractures of the Femur and Comparison of Radiological Outcomes when Managed with Proximal Femoral Nail vs the Dynamic Hip Screw with Locking Side Plate in the Indian Population
Background: Currently, the preferred implants for stable trochanteric fractures are the Proximal Femoral Nail and the Dynamic Hip Screw with Locking Side Plate. The Locking side plate has resolved many of the limitations associated with the standard DHS. Although numerous studies have compared the standard DHS and PFN, there is a scarcity of literature on the prevalence of IT fractures in the Indian population and comparison of Locking DHS and PFN in term of radiological union times. The purpose of this study is to assess and compare the effectiveness of both implants in stable intertrochanteric fractures. Methods: The objective of this study was to assess the prevalence of intertrochanteric fractures in the Indian population and compare the radiological outcomes of using Locking DHS and PFN for fixation in 40 patients who were admitted to SUT Academy of Medical Sciences between October 2019 and April 2021. Serial x-rays were used to evaluate the patients' progress, and regular follow-up was conducted to compare their outcomes. Results: All 40 fractures united. The time to union ranged from 16 to 30 weeks, with an average of 22.0 weeks in the DHS group and 19.40 weeks in the PFN group. %). 3 complications were noted. 2 in the DHS group, namely malunion and superficial infection and 1 delayed union in the PFN group. Conclusions: The DHS group relatively took more time to achieve union while the PFN group achieved union faster. However our finding was not statistically significant. Based on these findings, we can conclude that both the Proximal Femoral Nail and Dynamic Hip Screw with Locking Side Plate are similarly effective in treating stable intertrochanteric fractures.
Introduction
Trochanteric fractures are frequently observed in the elderly population, especially in women with osteoporosis, and even a minor fall can result in these fractures due to weakened bone structure. Intertrochanteric fractures resulting from such falls are prevalent. Failure to address these fractures can lead to mortality due to complications associated with cardiac, pulmonary, or renal problems, as well as factors such as advanced age and medical comorbidities.
In earlier times, non-surgical methods were the primary approach for managing these fractures. Nevertheless, extended immobilization and staying in bed resulted in poorly aligned fractures, abnormal gait, and increased mortality rates. To counter these problems, internal fixation techniques were developed to achieve early recovery of patients to their pre-injury state, enhanced comfort, and reduced complications related to bed rest.
In earlier times, the sliding hip screw was the preferred treatment approach, but it had drawbacks such as prolonged surgical time, lateral wall blowout, lag screw cut out, and varus collapse. To counter these issues, the Proximal Femoral Nail was developed as an intramedullary implant with benefits like closer placement to the mechanical axis, shorter operation duration, lesser blood loss, and early weight- bearing. However, this method also had some complications, such as jamming of the sliding mechanism, stress risers at the distal locking bolts, and the “Z” effect.
The Dynamic Hip Screw with Locking Compression Plate is a new method used to stabilize intertrochanteric fractures. However, the benefits of using the intramedullary fixation method with PFN over dynamic screw plate devices remain uncertain and subject to debate. In addition, there are only a limited number of studies comparing Proximal Femoral Nail and Dynamic Hip Screw with Locking Compression Plate.
Therefore, this study aimed to examine the prevalence of trochanteric fractures, possible complications, and evaluate radiological union times after fixation with PFN and locking DHS.
Methods
Source of Data
This was a prospective study conducted at SUT Academy of Medical Sciences from October 2019 to April 2021. 40 patients with Boyd & Griffin Types 1 & 2 pertrochanteric fractures were selected for the study. 20 patients were treated with Open Reduction and Internal Fixation using Dynamic Hip Screw with locking side plate and the other 20 patients were treated with Closed Reduction and Internal Fixation using Proximal Femoral Nailing. The cases were placed alternately into each groups with odd numbered pts placed into the PFN group and even numbered pts placed into the locking DHS group.
Method of Data Collection
On arrival to the casualty department, a detailed history about the trauma and mode of injury was obtained from the patient/patient’s attenders. A thorough clinical examination was then carried out, including general physical examination, systemic examination and local examination of the injured extremity. All the findings were recorded in the proforma.
On admission, all patients were given analgesics and skin traction was applied in the affected limb. Any comorbidities were noted and medication started for the same. All routine blood investigations were sent and a pre-anesthetic check- up was done regarding fitness for the surgical procedure.
All patients were taken for surgery only after an informed and written consent was obtained from the patient and patient’s attenders. 40 cases with Type 1 and Type 2 intertrochanteric fractures were studied.
Instrument Details
The study included the use of Dynamic Hip Screw (DHS) with Locking Compression Plate (LCP) and Proximal Femoral Nail (PFN).
Inclusion Criteria
- Patients with trochanteric fractures of the femur (Boyd & Griffin Type 1 &
Exclusion Criteria
- Patients with trochanteric fractures of the femur (Boyd & Griffin Type 3 & 4).
- Patients with polytrauma and multiple fractures in the same limb.
- Open fractures.
- Neurovascular injuries.
Period of Follow-Up
Patients were evaluated and assessed for radiological union and functional recovery post-operatively, at 3 weeks,
6 weeks, 3 months and 6 months with the help of Modified Harris Hip score and results were compared.
Parameters For Evaluation
- Patients were evaluated clinically, preoperatively and postoperatively.
- Radiological outcomes were determined using serial xrays and assessed till formation of bridging callus at the fracture site.
The following investigations were done for all patients Complete haemogram.
- Blood urea, Serum creatinine, Serum electrolytes.
- Blood grouping and Rh typing.
- PT, aPTT, INR.
- Urine routine.
- RBS; FBS and PPBS wherever required.
- X-rays: Pelvis with bilateral hips (AP view) and Femur with hip (AP, lateral views in traction internal rotation).
- HbSAg.
- HIV.
- ECG, Chest x-ray.
- 2D ECHO.
- CT Hip (if required) No investigations and interventions were conducted on other humans and/or animals.
Surgical intervention was undertaken after adequate pre- operative assessment was made, physician and anesthesia fitness were obtained and only after taking informed/written consent.
Initial Management
All patients after admission were thoroughly assessed and a comprehensive musculo-skeletal examination along with detailed history was taken.
Primary stabilization was done with the use of skin traction kit.
Average time interval between admission and surgery was 2-3 days during which period patients were evaluated for medical problems if any.
Spinal anaesthesia was given for all the patients and combined with epidural anesthesia in selected pts.
C-arm and fracture table were used for all the patients.
Surgical Technique: Dynamic Hip Screw with Locking Side Plate
Instruments and Implants

- Kidney tray
- Locking cortical screws
- Guide pins
- Towel clips
- Mops
- Langenbeck’s retractors
- T-handle
- Fixed angled guide
- Scissors and forceps
- Tap
- Triple reamer
- Locking sleeves
- Lag screws
- Bone holding clamps
- Locking side plates
- Osteotome
- Mallet
- Homan’s retractors/Bone levers
- Needle holder, artery forceps
Patient Positioning
After administration of spinal anaesthesia, the patient was positioned supine on a fracture table with a radiolucent, padded countertraction post between the patient’s legs.
The uninjured leg was kept flexed and abducted at the hip in a leg holder. The knee of the uninjured leg was padded in this position.
The injured leg was secured by a boot attached to the extension leg of the fracture table.
The adequacy of reduction in both antero-posterior and true lateral views was verified before surgical preparation.
Draping: Skin scrub and preparation was done over the hip till the umbilicus and the lateral aspect of the hip from the iliac crest to the distal thigh.
The operative site was draped with towels and drapes and towel clips placed so that they were not superimposed on the fracture during further imaging. The C-arm was draped separately.
Reduction: A closed reduction of the fracture was performed under C-arm guidance. The reduction was checked by both anteroposterior and lateral views in C-arm, paying special attention to cortical contact medially and posteriorly.
Exposure: Skin incision was made from the tip of the greater trochanter and then extended down the line of shaft of the femur for approximately 8 cm. The fat and underlying deep fascia were incised and the cut edges of the fascia retracted to pull the tensor fascia lata anteriorly. The fibres of vastus lateralis were split along its line of fibres and elevated from the lateral inter-muscular septum taking care to coagulate the perforating branches of the profunda femoris artery. The greater trochanter was exposed for introduction of guide pin.
Insertion of Guide Pin: The level of insertion of the guide pin varies with the angle of the plate used. The proximal aspect of the osseous insertion of the gluteus maximus and the tip of the lesser trochanter, which are approximately 2 cm below the vastus lateralis ridge, helped identify the level of entry of a 135-degree angle plate.
If higher angle side plate was used, the entrance site was moved 5 mm distally for each 5 – degree increase in barrel angle. The appropriate fixed – angle guide was fixed midway on the lateral cortex so that the guide pin entered at the designated level with the guide pin aimed towards the apex of the femoral head. The central placement was confirmed on the lateral view as well.
Another parallel guide pin was inserted to provide temporary stability, in which the reduction could be lost if the guide pin backed out and to prevent rotation of the femoral head during reaming.
Reaming:
- Once the guide pin had been inserted and measured, it was advanced an additional 5 mm and secured into the subchondral bone.
- Reaming was done according to the exact measurement of the lag screw length, and a lag screw that matched the length measurement was selected.
- The triple reamer was set to the lag screw length indicated by the measuring gauge and reaming was done until the distal aspect of the stop reached the lateral cortex.
Insertion of Plate and Lag Screw: The appropriate locking side-plate and Lag screw were assembled onto the insertion wrench. The lag screw was inserted until the desired length. The lag screw was advanced into the proximal femur to the predetermined level and its position was verified with image intensification. The position and depth of the screw was verified with image intensification in both planes. The centering sleeve was removed and the side plate was advanced onto the lag screw shaft. The plate tamper was used to fully seat the plate. The threaded guide pin is then removed.
Plate Fixation: The plate clamp was used to secure the plate to the shaft. Traction was slowly released to allow impaction of the fracture fragments. The plate was attached to the shaft of femur using 4.5 mm locking cortical screws. When all screws had been inserted and all traction had been released, the fracture could be compressed with the compression screw, (usually the 19 mm screw). If a short barrel was used, placement of compression screw was mandatory to prevent potential disengagement of the screw plate assembly.
Proximal Femoral Nail

- Screwdriver
- Guide Wire
- Drill Bit (4.0mm)
- Reamer (11.0 mm) for Lag Screw
- Drill Bit (6.5 mm) for Derotation Screw
- Entry point reamer
- Sliding Hammer
- Cannulated Awl
- Wrench
- Sleeve
- Trocar
- Jig
- Connecting Screw
- Proximal Femoral Nails
- Protecting Sleeve
- 8.0mm Lag screws
- 6.4mm Derotation Screws
- Distal Locking Screws
Positioning
The patient was positioned supine on the traction table. The ipsilateral arm was placed in arm sling. The unaffected limb was flexed , abducted and externally rotated for providing enough space for positioning of the image intensifier. The affected lower limb was held in traction and adduction in the foot piece. Reduction was achieved by traction (disengaging fracture fragments) and internally rotating the limb while maintaining traction and confirmed with image intensifier.
Approach
A 3cm incision was made proximal to the tip of greater trochanter slightly bent dorsally. Skin, subcutaneous tissue and deep fascia were incised. Gluteus maximus was split by blunt dissection and the tip of trochanter felt with finger.
Entry Point
After confirming the anatomical reduction , entry point was made with bone awl over the tip of greater trochanter. By confirming the position in AP and lateral view, the awl was driven just proximal to the level of lesser trochanter.
Guide Wire Insertion and Reaming
A 3.2mm guide wire was inserted and driven into the distal fragment. Proximal reaming was done with 15mm cannulated awl upto 7 cm distally to accommodate the proximal portion of the nail. Distal reaming was done 1mm more than the desired diameter of the nail.
Nail Insertion
The nail closely matching to the neck shaft angle of the unaffected hip was selected and assembled in the jig. The nail was inserted by gentle twisting movements to the appropriate depth to allow placement of two screws within the femoral neck. The guide wire was then removed.
Proximal Targeting
The nail with the jig was checked for alignment of proximal and distal targeting guide to the corresponding holes in the nail before insertion . Through a stab incision drill sleeves were inserted into the proximal targeting guide upto the lateral cortex with the help of trocar. Under C- arm control the guide pins for the lag screw and derotation screw were driven in through guide pin sleeves upto 5 mm from the articular surface of the femoral head. The lag screw and derotation screw of appropriate length was inserted after drilling with cannulated drill bit. The derotation screw was kept 10 to 15mm smaller than the lag screw.
Distal Targeting
Distal targeting was done with distal targeting guide and drill sleeves using 4.0mm drill bit.
Post-Operative Regimen:
- Appropriate I/V and oral antibiotics were given.
- Static quadriceps, ankle range of motion exercises and mobilization was started immediately on post-op day 2.
- Aseptic dressing change and wound inspection was done on post-op day 3.
- Toe-touch weight bearing was started on post-op day 4.
- Suture removal was done on post-op day 14th.
- Partial weight bearing with walker support was started from 2nd week as tolerated by the patient and based on quality of fixation.
- Additional drugs were given if osteoporosis was noted and managed accordingly Period of Follow-Up: Patients were evaluated and assessed post-operatively, subsequently for a minimum period of 6 months, at regular intervals of 3 weeks, 6 weeks, 3 months and 6 months for functional outcome with the help of Modified Harris Hip score and radiological union/fracture healing.
Results
The results observed are as follows.
| Age | Number of cases | Percentage |
|---|---|---|
| 30-40 | 4 | 10.00% |
| 41-50 | 9 | 22.50% |
| 51-60 | 10 | 25.00% |
| 61-70 | 8 | 20.00% |
| 71-80 | 9 | 22.50% |
| Total | 40 | |
| DHS | PFN | |
| Mean ± SD | Mean ± SD | |
| Age | 60.90 ± 12.54 | 57.65 ± 14.02 |
Table 1: Age distribution.
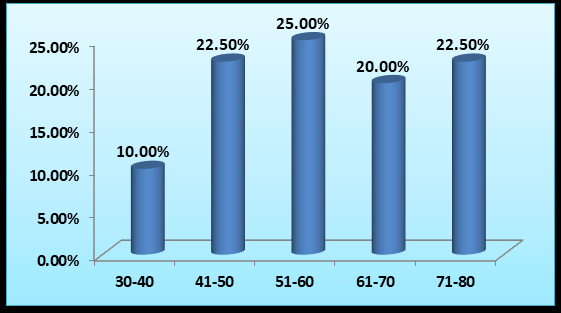
Trochanteric fractures were common in the age group of 51-60 years in this study. Minimum age of the patient was 33 years. Maximum age was 79 years (Table 1).
| Number of cases | Percentage | ||
|---|---|---|---|
| Left | 19 | 47.50% | |
| Right | 21 | 52.50% | |
| Total | 40 |
Table 3: Side distribution.
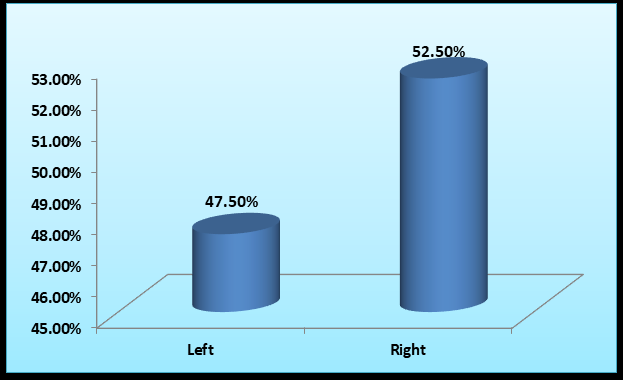
52.50% of the patients had fracture on the right side, whereas 47.50% had fracture on the left side.
| Sex | Number of cases | Percentage |
|---|---|---|
| Males | 30 | 75% |
| Females | 10 | 25% |
| Total | 40 |
Table 2: Gender distribution.
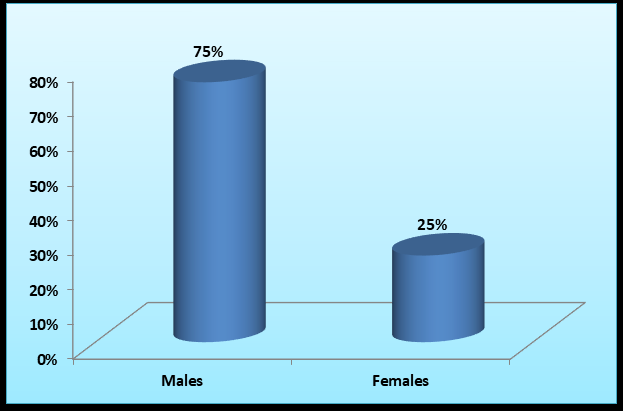
Majority of patients were males (75%) and only 25% were female patients (Figure 2).
| Number of cases | Percentage | Mechanism of trauma | Number of cases | Percentage | |
|---|---|---|---|---|---|
| Left | 19 | 47.50% | RTA | 7 | 17.50% |
| Right | 21 | 52.50% | Trivial fall | 33 | 82.50% |
| Total | 40 | Total | 40 |
Table 4: Mechanism of trauma distribution.
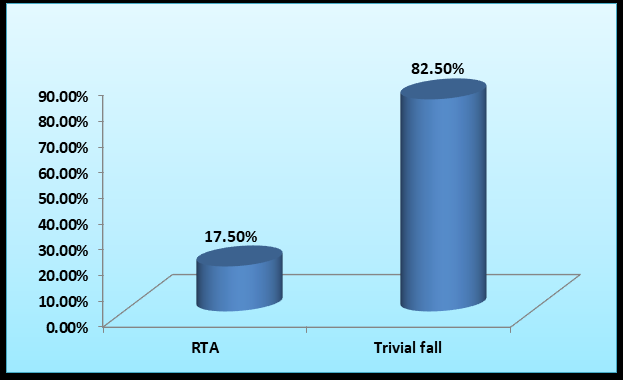
In majority of patients, mechanism of injury was trivial fall (TF) i.e. 82.50% whereas in the remaining 17.50% patients, injury was due to road traffic accidents (RTA) (Table 2).
| Boyd and Griffin fracture type | Number of cases | |||
|---|---|---|---|---|
| DHS | PFN | Total | Percentage | |
| Type 1 | 7 (35%) | 8 (40%) | 15 | 37.50% |
| Type 2 | 13 (65%) | 12 (60%) | 25 | 62.50% |
| Total | 20 | 20 |
Table 5: Fracture classification distribution.
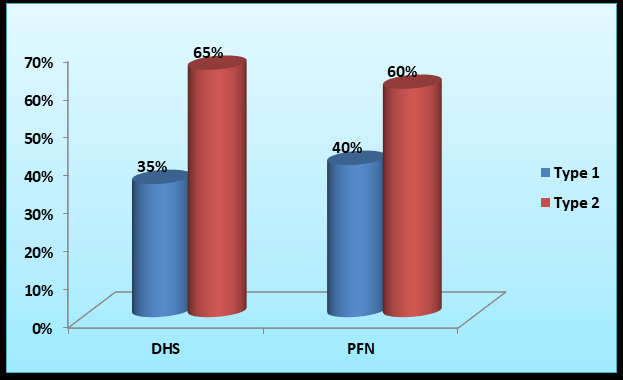
The predominant fracture type in our study was type 2 of Boyd and Griffin classification (62.50%).
In our study, of the 15 type 1 fractures, 7 were treated with Locking DHS and 8 with PFN. Of the 15 type 2 fractures, 13 were treated with Locking DHS and 2 with PFN.
| Time of union (in weeks) | Implant | ||
|---|---|---|---|
| Locking DHS | PFN | Total | |
| 16 | 2 (10%) | 5 (25%) | 7 (17.50%) |
| 18 | 2 (10%) | 6 (30%) | 8 (20.00%) |
| 20 | 5 (25%) | 4 (20%) | 9 (22.50%) |
| 22 | 4 (20%) | 3 (15%) | 7 (17.50%) |
| 24 | 3 (15%) | 0 | 3 (7.50%) |
| 26 | 1 (5%) | 1 (5%) | 2 (5.00%) |
| 28 | 2 (10%) | 1 (5%) | 3 (7.50%) |
| 30 | 1 (5%) | 1 (2.50%) | |
| Total | 20 | 20 | 40 |
Table 7: Time to union distribution
| DHS | PFN | P-Value | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Time of union (weeks) | 22.0 ± 3.89 | 19.40 ± 3.32 | 0.079 |
Table 6: Time to union distribution.
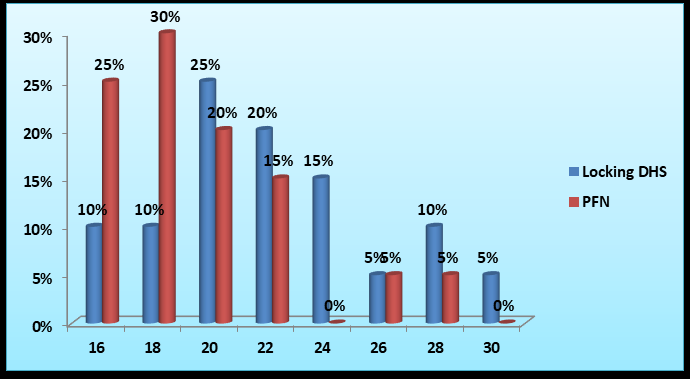
Union was defined as the absence of fracture line on two radiographic views.
All 40 fractures united. The time to union ranged from 16 to 30 weeks, with an average of 22.0 weeks in the DHS group and 19.40 weeks in the PFN group.
Complications
| DHS | PFN | Total | ||
|---|---|---|---|---|
| 22 | 4 (20%) | 5 (15%) | 7 (17.50%) | |
| 24 | 3 (15%) | 0 | 3 (7.50%) | |
| 26 | 1 (5%) | 1 (5%) | 2 (5.00%) | |
| 28 | 2 (10%) | 1 (5%) | 3 (7.50%) | |
| 30 | 1 (5%) | 1 (2.50%) | ||
| Total | 20 | 20 | 40 |
Table 8: Complication.
In our study, we noted 3 complications. 2 in the DHS group, namely delayed union and superficial infection and 1 malunion and implant failure in the PFN group.
Discussion
Age
The age criteria of our study was 20-80yrs. In our study, the majority of patients were in the age group of 51-60. There were 10 patients in this age group. The mean age in our DHS group was 60.9 and in our PFN group was 57.65.
In a study of 40patients conducted by Amandeep, et al. [1] the mean age in the DHS group was 60.3 and that in the PFN group was 56.85. In another study of 52patients conducted by Kushal, et al. [2], the mean age in the DHS group was 65 and that in the PFN group was 70.2. Our study has statistics similar to that of Amandeep, et al. [1].
| Mean Age (in Years) | |||||
|---|---|---|---|---|---|
| Study | Age Criteria (in Years) | DHS | PFN | ||
| Study | Age Criteria (in Years) | ||||
| Amandeep, et al. [1] | 20-80 | 60 | 57 | ||
| Kushal, et. al. [2] | 20-80 | 65 | 70 | ||
| Present Study | 20-80 | 61 | 58 |
Table 10: Studies comparing age distribution.
Sex
In our study, 30 (75%) were males and the remaining 10 (25%) were females. In the comparative study by Pan, et al. [3], the males comprised 75% of the study group. In his study of 80 cases, Shakeel, et al. [4] found that 66% of his study group were males. Zhao, et al. [5] describes the male incidence his study at 40%. In his study of 80 cases, Gill, et al. [6] found that males comprised only 32% of the study group. Our study has findings similar to that of Pan, et al. [3] but in terms of incidence of intertrochanteric fractures among sex, there is no uniformity in literature.
| Study | Males (In %) | Females (In %) |
|---|---|---|
| Pan, et al. [3] | 75 | 25 |
| Zhao, et al. [4] | 40 | 60 |
| Shakeel, et al. [5] | 66 | 33 |
| Gill, et al. [6] | 32 | 68 |
| Present Study | 75 | 25 |
| Study | Average Duration of Union (in Weeks) | |
| DHS | PFN | |
| Amandeep, et al. [1] | 14 | 14 |
| Venkatesh, et al. [9] | 10 | 8 |
| Kushal, et al. [2] | 17 | 17 |
| Shivraj, et al. [10] | 14 | 16 |
Table 12: Studies comparing sex distribution.
Mechanism of Injury
The major mechanism of injury was trivial fall in our study, accounting for 33 cases. In other 7 cases, the injury was sustained due to RTA. In his study of 30 cases, Mundla, et al. [7] described 70% of his cases as a result of trivial fall while 23% was due to RTA. Jonnes, et al. [8] conducted a study on 30 cases where he described 77% of his cases as a result of trivial fall while the remaining 23% was due to RTA. In his study on 80 patients, Gill, et al. [6] concluded that 66% of his cases were a result of trivial fall while the remaining were due to RTA. Our study also highlights that trivial fall is perhaps the important contributing cause of IT fractures.
| Study | Mechanism of Injury | ||
|---|---|---|---|
| Trivial Fall | RTA | Assault | |
| Mundla, et al. [7] | 70% | 23.30% | - |
| Jonnes, et al. [8] | 77% | 23% | - |
| Gill, et al. [6] | 66% | 34% | |
| Present Study | 82% | 18% |
Table 9: Studies comparing MOI distribution.
Duration of Union
In his comparative study of 80 patients using the Locking DHS and PFN, Gill, et al. [6] found that the average time for bony union was found to be 12weeks in the DHS group and 12.15 weeks in the PFN group. In our study the average duration of union in the DHS group was 22 weeks while that in PFN was 19.40 weeks.
| Study | Average Duration of Union (In Weeks) | |
|---|---|---|
| DHS | PFN | |
| SPS Gill, et al. [6] | 12 | 12 |
| Present Study | 22 | 19 |
Table 11: Studies comparing union times between Locking DHS and PFN.
In literature, studies comparing LOCKING DHS and PFN are scarce.
Studies Comparing Standard DHS and PFN: In his comparative study of 40 pts by Amandeep, et al. [1], average time for union was 14 weeks both in the DHS and the PFN group. Venkatesh, et al. [9], in this study of 400 pts found that average time for union was 10 weeks and 8 weeks in the DHS and PFN groups respectively. Kushal, et al. [2] in his study of 52 pts noted that there was no significant difference between union times in the DHS and PFN groups. Shivraj, et al. [10], in his study of 50 cases noticed that duration of union was higher in the PFN group (16weeks), while it was 14 weeks in the DHS group.
Studies of Locking DHS In a study of 44 patients by N.D. Chatterjee et al(11), the average duration of fracture union was 15.75 weeks. In another study of 25 patients by Nikhil et al(12), the average duration of fracture union was 13.96 weeks. In our study the average duration of union in the DHS group was 22weeks.
| Study | Average Duration of Union (In Weeks) |
| Chatterjee, et al. [11] | 15.75 |
| Nikhil, et al. [12] | 13.96 |
| Present Study | 22 |
Table 13: Studies comparing union times in Locking DHS.
The patient in the DHS group had moderate restriction of activities of daily living associated with malunion due to excessive collapse and the patient in the PFN group had moderate restriction of activities of daily living associated with deformities which had resulted from prolonged immobilization against our orders.
During our study, we have observed that few patients (5 pts) in the DHS group required blood transfusions during the post-operative period due to the longer length of incision and associated blood loss. This was not seen in the PFN group, in whom we used a shorter length of incision. Also, the PFN surgeries were associated with a longer operating time and increased C-ARM exposure than DHS surgeries. But patients in the PFN group were mobilized partial weight bearing earlier than those in the DHS group.
In our study, there were 2 pts with COPD, 7 pts with DM and 9 pts with HTN. Of them, surgery had to be delayed in 4 pts with DM due to poor sugar control. One pt with DM in the DHS group was found to have superficial infection.
Acknowledgements
I would like to thank my patients and colleagues who have immensely contributed to the study.
References
-
Amandeep Singh B, Pardeep K, Brar BS (2018) Comparative study between DHS and PFN in intertrochanteric fractures of femur. International Journal of Orthopaedics Sciences 4(1): 259-262.
-
Nikhil ParikhK, Chintan P, Mitesh P, Shalin Bharat S (2018) Functional and radiological outcome of proximal femoral nailing versus dynamic hip screw in unstable intertrochanteric femur fractures. Int J Res Orthop 4(6): 861-866.
-
Pan X, Xiao D, Lin B, Huang G (2004) Dynamic hip screws (DHS) and proximal femoral nails (PFN) in treatment of intertrochanteric fractures of femur in elderly patients. Chinese Journal of Orthopaedic Trauma 6(7): 785-789.
-
Shakeel AQ, Robin S, Amit MN, Vikas T, Afroz AK, et al. (2019) Comparative study of functional outcome of the intertrochanteric fracture of femur managed by Dynamic hip screw and proximal femoral nail. National Journal of Clinical Orthopaedics 3(1): 26-30.
-
Zhao C, Liu DY, Guo JJ (2009) Comparison of proximal femoral nail and dynamic hip screw for treating intertrochanteric fractures. China J Orthop & Trauma 7: 535-537.
-
Gill SPS, Ankit M, Manish R, Pulkesh S, Sunil K, et al. (2017) Dynamic hip screw with locked plate vs proximal femoral nail for the management of intertrochanteric fracture: a comparative study. International Journal of Orthopaedics Sciences 3(2): 173-180.
-
Mundla MKR, Shaik MR, Buchupalli SR, Chandranna BA (2018) prospective comparative study between proximal femoral nail and dynamic hip screw treatment in trochanteric fractures of femur. Int J Res Orthop 4(1): 58-564.
-
Cyril J, Shishir SM, Najimudeen S (2016) Type II Intertrochanteric Fractures: Proximal Femoral Nailing (PFN) Versus Dynamic Hip Screw (DHS). Arch Bone Jt Surg 4(1): 23-28.
-
Venkatesh G, Veera Shekar V (2015) Comparative study between dynamic hip screw vs proximal femoral nailing in inter-trochanteric fractures of the femur in adults. International Journal of Orthopaedics Sciences 1(1): 7-11.
-
Shivraj SK, Santosh SB, Rohit S, Abhijit M, Prashant K (2018) Dynamic Hip Screw and Proximal Femoral Nail as a Mode of Surgical Treatment in Intertrochanteric Fractures of Femur in Elderly Patients. International Journal of Contemporary Medical Research 5(4): D4-D7.
-
Chatterjee ND, Goutham B, Thirthankar B (1991) Dynamic hip screw and sliding plate for trochanteric fractures of femur. Review 34(3): 153-155.
-
Nikhil J, Partap SV, Jaspal S (2017) Role of locking dynamic hip screw in management of inter-trochanteric fractures of femur in elderly patients. IJOS 3(1): 529-533.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results