Management of Diaphyseal Forearm Fractures in Paediatric Patients: Lesson Learnt During COVID-19 Pandemic
Objectives: Our objectives were to study the epidemiology, management and change in trends in management of paediatric diaphyseal forearm fractures during the COVID-19 pandemic. Methods: It was a prospective study which included all fresh (≤ 3 weeks), traumatic, forearm diaphyseal fractures in paediatric patients ≤ 16 years. Closed & compound grade I fractures were included. Pathological fractures, compound grade II/III fractures and fractures ≥ 3 weeks old were excluded. All patients underwent closed reduction and above elbow cast application. Acceptability of reduction was graded as per the criteria described by Noonan KJ, et al. At 2 weeks follow-up, repeat check radiograph was done for assessing acceptable reduction. Patients with acceptable reduction were continued with nonsurgical treatment and patients with loss of reduction were offered operative intervention. But due to refusal of operative intervention by the parents, patients were continued with the nonsurgical treatment. Results: Eighty patients were available for follow-up. Mean age was 7.78 years. Left to right side involvement was 58% & 42% respectively. Out of 80 patients, 20 patients were operated due to failed closed reduction, while 60 patients were managed nonsurgically. Out of 60 patients, 18 (30%) presented with loss of reduction and were offered surgery. Refusal to surgery pushed us to continue with nonsurgical treatment and evaluation as a separate group in the study as nonsurgically treated, not meeting the acceptability criteria. In nutshell out of 80 patients, 20 were managed operatively, while 60 were managed nonsurgically, 42 (70%) patients meeting the acceptable reduction criteria while 18 patients (30%) were not meeting the acceptable reduction criteria. Restriction of forearm rotations was found to be statistically insignificant in all nonsurgically treated patients irrespective of the reduction criteria met or not. Furthermore, on sub-grouping the patients with loss of reduction, on the basis of age and angulation it was observed that there was no significant change in the final functional outcome in the patients with angulation of 15-18 degrees in ≤ 10 years of age and 10-13 degrees in > 10 years of age weather treated conservatively or operatively (p value = 0.522). However, when angulation was > 18 degrees in ≤ 10 years of age and > 13 degrees in > 10 years of age, it was observed that operated patients had statistically significant better functional outcome when compared to conservatively treated patients (p value < 0.05). Conclusion: Our study attempts to highlight the management of paediatric forearm diaphyseal fractures with emphasis on nonsurgical management of these injuries to deal with the scarcity of follow-up care during the global health crisis. The encouraging results of our conservatively treated patients, even when angulation is few degrees more than the acceptable limit, allows us to widen the acceptable limit of reduction in paediatric population, especially when the health care system is challenged by the global pandemic and its restrictions. However more studies are required to confirm our findings before making them generalizable.
Introduction
Both bone forearm fractures account for 3-6% of all fractures in children [1]. Forearm fractures are the 3rd most common fracture in children [2]. The most common mechanism of injury is fall onto an outstretched hand [3]. Management of paediatric forearm fracture is a challenge for the treating orthopaedic surgeon. The diagnosis of forearm fracture is straight forward. However treatment of such fractures is contentious (surgical vs nonsurgical) due to fewer acceptances of deformity and functional loss. In the 1960s, closed reduction and immobilisation in plaster were recommended for all of the paediatric forearm fractures, and the criteria of acceptable reduction varied. Management of paediatric forearm fractures has witnessed a significant transform in last two to three decades of the 20th century with the prototype shift from conventional nonsurgical management to surgical management. Schmittenbecher have shown that surgical management of diaphyseal forearm fractures at their institution has increased from 1% between 1976 and 1985 to 40.4% between 1998 and 2000 [4]. Ever since there is an increased interest in surgical treatment of diaphyseal forearm fractures, especially in older age group (≥ 10 years). However, the COVID-19 global pandemic not only has profound effect on the volume and epidemiology of paediatric diaphyseal forearm fractures, but also raised a concomitant concern about follow-up and subsequent management. Orthopaedic daily practice has been profoundly revolutionized by the pandemic. During the COVID pandemic, there was an increased emphasis on nonsurgical strategies [5].
Our objectives were to study the epidemiology and management of the paediatric diaphyseal forearm fractures during the COVID-19 pandemic. We further studied the change in trends from surgical to nonsurgical management of these injuries to deal with the scarcity of follow-up care during the global health crisis.
Methods
Study Design
This was a prospective study of the management of paediatric diaphyseal forearm fractures, from October 2020 to September 2022. The study was approved by the institutional ethical committee (IECJNMC/380). Informed consent was obtained from the parents of all the patients. The study was performed according to the ethical standards of the 1964 Declaration of Helsinki as revised in 2000.
Inclusion and Exclusion Criteria
We included all fresh (≤ 3 weeks), traumatic, forearm diaphyseal fractures in paediatric patients ≤ 16 years of age. Closed as well as compound grade I fractures [6] were included. Pathological fractures, compound grade II & III fractures and fractures >3 weeks old were excluded from the study.
Management Protocol
Paediatric patients with pain and deformity following trauma to the forearm were carefully evaluated clinically for any associated injuries, skeletal or otherwise. Once patients were haemodynamically stable, radiological evaluation of the forearm was carried out by obtaining two orthogonal views of forearm including the wrist and elbow joints. After assessment, all closed and compound grade I fractures were treated with closed reduction and above elbow cast application with post-reduction check radiographs in two orthogonal planes (AP and lateral views). Acceptability of reduction was graded as per the criteria described by Noonan KJ, et al. [7] (Table 1).
| Patient age | Angulation (degrees) | Mal-rotation (degrees) | Bayonet apposition |
| 0-9 years | <15 | <45 | Yes, if <1 cm short |
| ≥10 years (mid/distal shaft) | <15 | <30 | |
| ≥10 years (proximal shaft) | <10 | 0 | |
| Approaching skeletal maturity (<2 years remaining growth) | 0 | 0 |
Table 1: Acceptable reduction guidelines for paediatric both-bone forearm fractures stratified by age and fracture location [7].
If fracture reduction was found in acceptable range, patients were discharged with the advice to follow up after 2 weeks for repeat check radiograph. If the fracture reduction is not as per the reduction criteria, then another trial of closed reduction and cast application was given for getting an acceptable reduction and now if the reduction is achieved, the patient is asked to come after 2 weeks for repeat check radiograph. However, if the reduction criterion is not met then the patient is planned for operative intervention. At 2 weeks follow-up, repeat check radiograph was done for assessing acceptable reduction (as per the study criteria). Patients with acceptable reduction were continued with nonsurgical treatment. However, parents of patients with loss of reduction were explained and offered operative intervention. But due to refusal of operative intervention by the parents, patients were continued with the nonsurgical treatment.
Functional Outcome Evaluation
All the patients included in the study were followed up and assessed for functional outcome score at minimum of 6 months by the criteria proposed by Flynn JM, et al. [1] (Table 2).
| Clinical Outcome Score | Criteria |
|---|---|
| Excellent | Full range of motion (supination and pronation), and no postoperative complications |
| Fair | Minimal loss of range of motion (< 30 degree of supination and/or pronation) and/or minor, resolving postoperative complication |
| Poor | Loss of range of motion (supination and pronation) > 30 degree, and/or major postoperative complication (i.e., infection, compartment syndrome, or delayed union) |
Table-2: Outcome Classification for paediatric Forearm Fractures.
Hence, based on treatment received and refusal to surgery by parents at 2 weeks follow-up in loss of reduction cases, the study subjects have been divided into 3 groups and clinic-radiological evaluation was done in these three groups as per the criteria proposed by Flynn JM, et al. [1].
- Nonsurgical management (coming in reduction criteria)
- Nonsurgical management (not coming in reduction criteria)
- Operatively treated
Statistical Analysis
Qualitative variables were recorded as frequencies and percentages and compared by chi-square test (χ_2 test). Quantitative variables were presented as means ± SD and compared by Student’s _t test. A p_-_value less than 0.05 was considered statistically significant.
Results
Study Population and Demographic Characteristics
A total of 100 patients with diaphyseal forearm fractures presented to our institute, from October 2020 and September 2022, were examined, assessed and treated according to the study treatment protocol. Twenty patients were lost to follow up due to COVID-19 lockdown restrictions. Finally 80 patients (80%) were available for follow-up and observations were recorded as per fixed proforma. Out of 80 patients, 52 patients (65%) in the study were males and 28 (35%) were females. Mean age of patients in the study was 7.78 years (range 2 months to 16 years). Twenty five patients were in the age group of 0-5 years, 32 patients were in age group of 6-10 years and 23 were in 11-16 years age group. In the present study, 58% patients had involvement of left side, while 42% had involvement of right side (Table 3).
| Variables | Number of patients | |
|---|---|---|
| Excellent | Full range of motion (supination and pronation), and no postoperative complications | Male = 52 (65%); Female = 28 (35%) |
| Excellent | ||
| Fair | Minimal loss of range of motion (< 30 degree of supination and/or pronation) and/or minor, resolving postoperative complication | Range = 2 months to 16 years; Mean = 7.78 years |
| Fair | ||
| Poor | Loss of range of motion (supination and pronation) > 30 degree, and/or major postoperative complication (i.e., infection, compartment syndrome, or delayed union) | Right = 33 (41.25%); Left = 47 (58.75%) |
| Poor | ||
| Poor | Diaphyseal Location | Proximal = 24 (30%); Middle = 29 (36.25%); Distal = 27 (33.75%) |
| Poor | Number on bone involved | Both bones = 62 (77.5%); Single Bone = 18 (22.5%) |
| Method of treatment | Nonsurgical = 60 (75%); Surgical = 20 (25%) |
Table 3: Demographical details of our study population.
Sixty two patients (77.5%) sustained injury to both bones while 18 patients (22.5%) sustained injury to either ulna or radius. Out of 18 patients who had single bone involved two cases have distal radio ulnar joint subluxation. Twenty four patients had proximal 1/3 fracture, 29 of the patients had middle 1/3 fracture and 27 had distal 1/3 fracture. In the study all patients were given an attempt of closed reduction and cast application at presentation, failing which patients were operated. Out of 80 patients, 20 patients were operated due to failed closed reduction, while 60 patients were managed nonsurgically. Among the surgically treated patients, 10 patients were treated with K-wires, 8 with titanium elastic nails, and 2 with compression plating. Range of follow-up varied from 6 months to 24 months (mean = 11.7 months).
Loss of Reduction at 2 Weeks in Nonsurgically Treated Patients
In the current study, we treated 60 patients nonsurgically as per the criteria described by Noonan KJ (1998) based on acceptable reduction guidelines for paediatric forearm bone fractures stratified by age and fracture location [7]. Out of the 60 patients, 18 (30%) patients presented with loss of reduction at 2 weeks (deviation from acceptable reduction criteria). Although we offered surgical intervention to the patients, refusal to surgery due to one or other reason pushed us to continue with nonsurgical treatment in these 18 cases. So they were evaluated as a separate group in the study as nonsurgically treated, not meeting the acceptability criteria. In nutshell out of 80 patients, 20 were managed operatively, while 60 were managed nonsurgically, 42 (70%) patients meeting the acceptable reduction criteria while 18 patients (30%) were not meeting the acceptable reduction criteria.
Treatment Type Versus Restriction of Forearm Rotations (Supination and Pronation)
In current study, restriction of forearm supination movement was found to be statistically insignificant in all nonsurgically treated patients irrespective of the reduction criteria met or not. Twenty seven patients (64%) treated nonsurgically as per the reduction criteria, had no restriction in supination, while 13 patients (32%) had 10 degree of restriction, and 2 patients (4%) had 20 degree of restriction. While 8 patients (45%) treated nonsurgically, deviating from the acceptable reduction (not coming in the reduction criteria) had no restriction in supination, 7 patients (41%) had 10 degree of restriction and 3 patients (14%) had 20 degree of restriction. Similarly, the range of restriction in pronation was found to be statistically insignificant in patients who were treated nonsurgically weather coming in the reduction criteria or not. Twenty four patients (57%) who were treated nonsurgically as per reduction criteria had no restriction in pronation, while 15 patients (35%) had 10 degree of restriction and 3 patients (8%) had 20 degree of restriction. While, 7 patients (37.5%) who were treated nonsurgically, deviating from the acceptable reduction (not coming in the reduction criteria) had no restriction in pronation, 6 of them (33.3%) had 10 degree of restriction and 5 patients (29.2%) had 20 degree of restriction. Figures 1 & 2 represents the patients with loss of reduction at 2 weeks follow-up in our study population with good clinico-radiological healing.
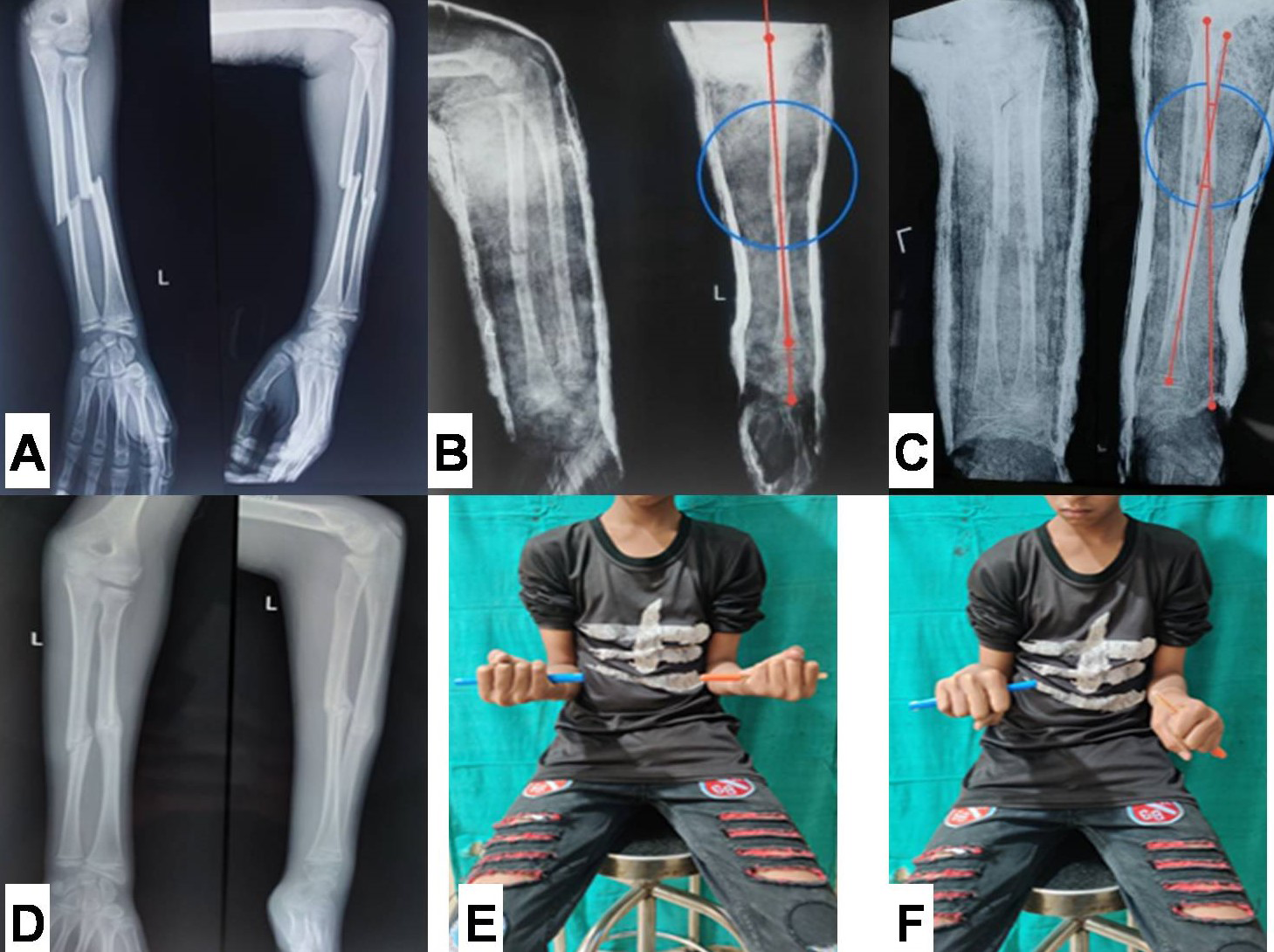
Figure 1: A: Pre-reduction plain radiograph showing both bone forearm fracture in 14 year old boy. B: Immediate radiograph following closed reduction showing acceptable reduction. C: Radiograph at 2-weeks, showing angulation of 11˚ (outside range of acceptable limits). D: Radiograph showing united fracture with remodelling of angulation. E & F: Clinical photograph showing full supination with terminal 20˚ of pronation restriction.
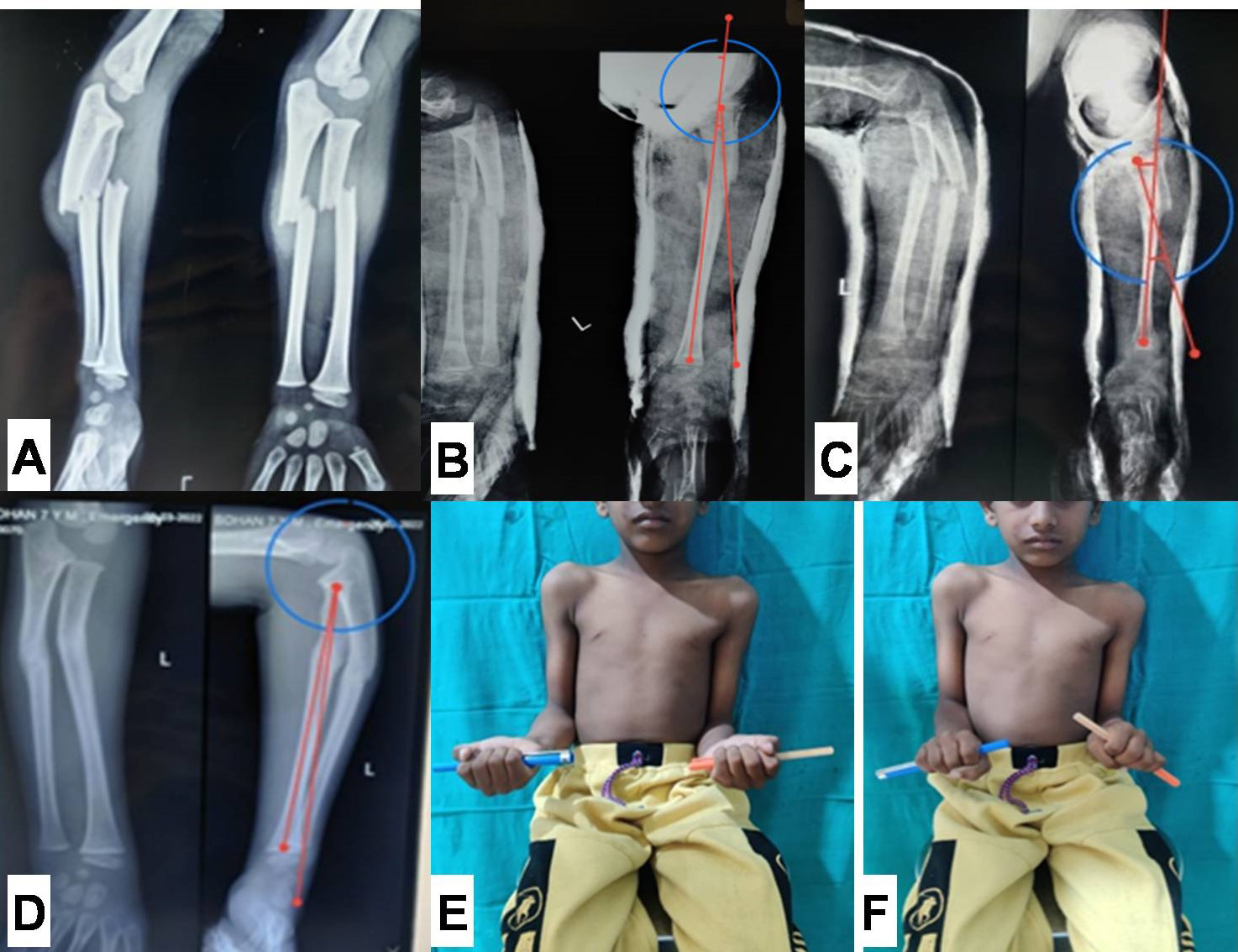
Figure 2: A: Pre-reduction plain radiograph showing both bone forearm fracture in 7 year old boy. B: Immediate Check radiograph showing an angulation of 8.6 degrees (acceptable Range). C: Radiograph at 2-weeks, showing angulation of 18.5˚ (outside range of acceptable limits). C: Radiograph showing united fracture with remodelling of angulation (3.6˚ of angulation). E & F: Clinical photograph showing full supination with terminal 10˚ of pronation restriction.
Comparison of Functional Outcome between Nonsurgically and Surgically Treated Patients at Final Follow Up
managed conservatively (coming in the reduction criteria proposed by Flynn MJ, et al. [1]. While, 5 patients (29%) had excellent functional outcome, 11 patients (62%) had fair outcome and 2 patients (9%) had poor outcome who were managed conservatively (not coming in the reduction criteria proposed by Flynn MJ, et al. [1]. However amongst the surgically treated patients, 12 patients (60%) had excellent functional outcome, 7 patients (35%) had fair outcome and one patient (5%) had poor outcome (Table 4).
- Patients had been assessed for functional outcome score based on the criteria proposed by Flynn JM, et al. [1], and they were graded accordingly. Twenty eight patients (66%) had excellent functional outcome, 13 patients (32%) had fair outcome and one patient (2%) had poor outcome who were
- Conservative
- Conservative
- Operative
- Chi-square value p-value
- (Within range of acceptable reduction)
- (Outside range of acceptable reduction)
- Functional outcome score
- Excellent
- 28 (66%)
- 5 (29%)
- 12 (60%)
- Fair
- 13 (32%)
- 11 (62%)
- 7 (35%)
- 32.58 p<0.05
- Poor
- 1 (2%)
- 2 (9%)
- 1 (5%)
- The 18 patients treated nonsurgically with loss of reduction at 2 weeks, were divided into two groups on the basis of angulation and age of the child (group 1 and 2), and were compared with the surgically treated patients.
- Group 1: Angulation of 15-18 degrees ≤ 10 years; angulation of 10-13 degrees in > 10 years. Group 2: Angulation of >18 degrees in ≤ 10 years; angulation of >13 degrees in > 10 years.
- Group 1
- Functional outcome score
- Operative
- Chi-square value p-value
- Angulation of 15-18 degrees ≤ 10 years; angulation of 10-13 degrees in > 10 years
- Excellent
- 7 (50%)
- 12 (60%)
- Fair
- 6 (42.86%)
- 7 (35%)
- 1.29 p=0.522
- Poor
- 1 (7.14%)
- 1 (5%)
Table 4: Functional outcome for all patients, treated nonsurgically (including patients within range of acceptable reduction &
Comparison of Functional Outcome between Nonsurgically Treated (with Loss of Reduction) and Surgically Treated Patients
In our study the final functional score between the group 1 (n=14) and operative group (n=20) was found to be statistically insignificant, and it was observed that there was no significant change in the final functional outcome in the patients with angulation of 15-18 degrees in ≤ 10 years of age and 10-13 degrees in > 10 years of age weather treated conservatively or operatively (Table 5). Final functional score between the group 2 (n=4) and operative group (n=20) was found to be statistically significant, and it was observed that patient had better functional outcome when treated operatively as compared to conservatively treated when angulation is > 18 degrees in ≤ 10 years of age and > 13 degrees in > 10 years of age (Table 6).
- Table 5: Comparison of functional outcome between operative group and group 1 (Angulation of 15-18 degrees ≤ 10 years; angulation of 10-13 degrees in > 10 years).
- Group 2
- Functional outcome score
- Operative
- Chi-square value p-value
- Angulation of >18 degrees in ≤ 10 years; angulation of >13 degrees in > 10 years
- Excellent
- 1 (25%)
- 12 (60%)
- Fair
- 2 (50%)
- 7 (35%)
- 30.39
- P<0.05
- Poor
- 1 (25%)
- 1 (5%)
Table 5: Comparison of functional outcome between operative group and group 2 (Angulation of >18 degrees in ≤ 10 years;
Discussion
Of late, diaphyseal forearm fractures in children have become increasingly common. Conservative treatment is usually preferred modality of treatment for uncomplicated union and good functional outcome. Potential complications included with management of such fractures are re- displacement (loss of reduction), decreased range of motion (forearm rotations), delayed union, residual deformity, and re-fracture. Of these complications, re-displacement was our main concern in the current study due to the restrictions imposed in COVID-19 lockdown, as the restrictions were a potential menace to regular follow-up and further management. Some studies showed that there is an increased interest in surgical treatment of diaphyseal forearm fractures [1, 4]. It was reported that there is an increase in the rate of complications following non-operative treatment compared with operative treatment which could be the reason that management has shifted to surgical one [8]. However, the COVID-19 global pandemic not only has profound effect on the volume and epidemiology of paediatric diaphyseal forearm fractures, but also raised a concomitant concern about follow-up and subsequent management. During the COVID-19 pandemic, there was an increased emphasis on nonsurgical strategies for managing orthopaedic injuries including the paediatric diaphyseal forearm fractures [5]. Our study findings suggested the inclination of the doctors and parents for nonsurgical management of these injuries in order to deal with the scarcity of follow-up care during the global health crisis (75% nonsurgical vs 25% surgical management of the study subjects). Furthermore, the change in trend from surgical to nonsurgical management was also reinforced by the refusal to surgery by the parents due to one or the other reason in cases of re-displacement at 2 week follow-up.
Evaluation of the patients with loss of reduction (re- displacement) at follow-up as a separate group (nonsurgically treated, not meeting the acceptability criteria), revealed remarkable findings. Restriction of forearm rotations (supination and pronation) was found to be statistically insignificant in all nonsurgically treated patients irrespective of the reduction criteria met or not. Furthermore, on sub- grouping the patients with loss of reduction into two groups on the basis of age and angulation, it was observed that there was no significant change in the final functional outcome in the patients with angulation of 15-18 degrees in ≤ 10 years of age and 10-13 degrees in > 10 years of age weather treated conservatively or operatively (p value = 0.522). However, when angulation was > 18 degrees in ≤ 10 years of age and > 13 degrees in > 10 years of age, it was observed that operated patients had statistically significant better functional outcome when compared to conservatively treated patients (p value < 0.05). On reviewing the literature, whether anatomic alignment associates well with forearm rotations is contentious. Fuller, et al. [9] established a positive relationship with residual angulation and eventual range of motion. On the other hand, reports of good forearm rotations with poor anatomic healing can be seen in literature [10]. Conversely, cases of anatomic healing with documented motion loss have been reported [10, 11]. Studies of documented mal-unions revealed that good functional outcome can be obtained in patients with motion loss up to 50 degrees, and that more symptomatic losses can be partly compensated for with shoulder movements [9, 11]. Some authors have reported little functional loss with decreases in forearm rotations of 35 to 40 degrees [10, 12]. Hogstrom H, et al. [13] reported that some patients with a limitation of ≤ 60 degrees of forearm rotations appeared to be unaware of their incapacity. In addition, it is feasible that patients with initially unsatisfactory motion may have improvement with time [14]. Although differing definitions of acceptable alignment have been delineated in the literature, many patients with residual deformity have good functional results [7]. This disparity in literature suggests that factors other than alignment may affect range of motion. In print discrepancies between residual angular deformity and final forearm rotations may be attributed to the inability to accurately document and record the radiographic mal-rotation [9, 10, 11, 15].
Literature is divided on the opinion to change over to surgical management in conservatively managed children, owing to the considerable remodelling potential, gradual improvement in forearm rotations with time and variable acceptability criteria, especially in the hands of experienced paediatric orthopaedic surgeons. Franklin CC, et al. [16] stated that, successful treatment of paediatric forearm fractures should result in painless and complication free outcomes with functional forearm rotations [17]. Caruso G, et al. [18] reported that conservative management is a safe and successful treatment choice in forearm fractures in children. Operative intervention is recommended when an acceptable reduction cannot be obtained with conservative treatment [16]. Although we offered operative intervention for patients with loss of reduction, but refusal from parents due to COVID-19 restrictions pushed us for accepting the reduction and continuing it till union. Our study demonstrated that the functional outcome was comparable with operated patients even with angulation of 15-18 degrees in ≤ 10 years and angulation of 10-13 degrees in > 10 years in nonsurgically treated patients. However, when angulation is >18 degrees in ≤ 10 years and angulation of >13 degrees in > 10 years, the functional outcome was inferior in nonsurgically treated patients when compared with operated patients. Therefore, accepting the reduction within few degrees of deviation from standard reduction criteria proposed by Noonan KJ, et al. [7], has no significant effect on forearm rotations and functional outcome.
Conclusion
Our study attempts to highlight the management of paediatric forearm diaphyseal fractures with emphasis on nonsurgical management of these injuries to deal with the scarcity of follow-up care during the global health crisis. The strengths of the study were prospective nature, a definite treatment protocol and valid evaluation tools. However, small sample size and short follow-up were the limitations of current study. The encouraging results of our conservatively treated patients, even when angulation is few degrees more than the acceptable limit, allows us to widen the acceptable limit of reduction in paediatric population, especially when the health care system is challenged by the global pandemic and its restrictions. Nevertheless if the reduction is not maintained then it is advisable to go for operative intervention as it provides better reduction, early physiotherapy and excellent range of motion. However more studies are required to confirm our findings before making them generalizable.
References
-
Flynn JM, Jones KJ, Garner MR, Goebel J (2010) Eleven years experience in the operative management of pediatric forearm fractures. J Pediatr Orthop 30(4): 313- 319.
-
Bowman EN, Mehlman CT, Lindsell CJ, Tamai J (2011) Nonoperative treatment of both-bone forearm shaft fractures in children: predictors of early radiographic failure. J Pediatr Orthop 31(1): 23-32.
-
Patel A, Li L, Anand A (2014) Systematic review: functional outcomes and complications of intramedullary nailing versus plate fixation for both-bone diaphyseal forearm fractures in children. Injury 45(8): 1135-1143.
-
Schmittenbecher P, Dietz H, Linhart W (2000) Complications amd Problems in Intramedullary Nailing of Children’s Fractures. Eur J Trauma 26: 287-293.
-
Mohamed BZ, Youseff Bashta MM, Eid TA, El Behiry AM (2022) Outcome of management of diaphyseal forearm fracture in children during coronavirus disease 2019 crisis. Menoufia Med J 35(3): 1579-1584.
-
Gustilo RB, Anderson JT (1976) Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses_._ J Bone Joint Surg Am 58(4): 453-458.
-
Noonan KJ, Price CT (1998) Forearm and distal radius fractures in children. J Am Acad Orthop Surg 6(3): 146- 156.
-
OmeroGlu H, Cassiano Neves M (2020) Tendency towards operative treatment is increasing in children’s fractures: results obtained from patient databases, causes, impact of evidence-based medicine. EFORT Open Rev 5(6): 347- 353.
-
Fuller DJ, McCullough CJ (1982) Malunited fractures of the forearm in children. J Bone Joint Surg Br 64(3): 364- 367.
-
Daruwalla JS (1979) A study of radioulnar movements following fractures of the forearm in children. Clin Orthop 139: 114-120.
-
Price CT, Scott DS, Kurzner ME, Flynn JC (1990) Malunited forearm fractures in children. J Pediatr Orthop 10: 705- 712.
-
Carey PJ, Alburger PD, Betz RR, Clancy M, Steel HH (1992) Both-bone forearm fractures in children. Orthopedics 15: 1015-1019.
-
Hogstrom H, Nilsson BE, Willner S (1976) Correction with growth following diaphyseal forearm fracture. Acta Orthop Scand 47(3): 299-303.
-
Thomas EM, Tuson KWR, Browne PSH (1975) Fractures of the radius and ulna in children. Injury 7: 120-124.
-
Voto SJ, Weiner DS, Leighley B (1990) Redisplacement after closed reduction of forearm fractures in children. J Pediatr Orthop 10(1): 79-84.
-
Franklin CC, Robinson J, Noonan K, Flynn JM (2012) Evidence-based medicine: Management of pediatric forearm fractures. Journal of Pediatric Orthopaedics 32: S131-S134.
-
Kramhoft M, Solgaard S (1989) Displaced diaphyseal forearm fractures in children: Classification and evaluation of the early radiographic prognosis. J Pediatr Orthop 9(5): 586-589.
-
Caruso G, Caldari E, Sturla FD, Caldaria A, Re DL, et al. (2021) Management of pediatric forearm fractures: What is the best therapeutic choice? A narrative review of the literature. Musculoskelet Surg 105(3): 225-234.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results