Management of Lung cancer Along with Bronchial Asthma through Ayurveda Stand Alone: A Case Report
Lung cancer remains one of the leading causes of cancer-related morbidity and mortality worldwide, with adenocarcinoma, squamous cell carcinoma (SCC), and neuroendocrine malignancies such as small cell lung carcinoma (SCLC) being the most prevalent subtypes. Despite advancements in conventional therapies—including surgery, chemotherapy, radiotherapy, targeted therapy, and immunotherapy—the overall prognosis and survival rates have not improved satisfactorily in many cases. This highlights the need for alternative or complementary therapeutic approaches, such as Ayurvedic interventions. Case Report: A 70-year-old male patient with a history of bronchial asthma and a 25-year history of tobacco (bidi) use presented with persistent symptoms of dry cough, severe left-sided chest and back pain (Parshvshoola), dyspnea (Shwashakrichchhita), significant weight loss (approximately 8 kg over one year), generalized weakness (Daurbalya), and loss of appetite (Aruchi). The patient reported experiencing these symptoms for three years before seeking treatment. Upon evaluation in the cancer outpatient department (OPD) of NIA Hospital, Jaipur, the patient was diagnosed with lung adenocarcinoma. Ayurvedic management was initiated, incorporating formulations such as Arbud Har Kashaya and Swarna Vasant Malti Rasa, among others, in a structured protocol. Results: Post-treatment radiological assessment demonstrated a reduction in tumor dimensions from 43 × 41 × 40 mm to 38 × 37× 38 mm, along with symptomatic improvement in appetite, pain, and respiratory distress. This case underscores the potential role of Ayurvedic therapy in the management of lung adenocarcinoma, even in the absence of conventional oncological treatments. Conclusion: This case highlights the successful application of Ayurvedic treatment protocols in managing lung adenocarcinoma, suggesting a promising integrative approach for patients unable or unwilling to undergo standard therapies. Further clinical studies are warranted to validate the efficacy of Ayurvedic interventions in oncology.
Prajapati M¹, Paijwar P²*, Sharma A³, Porte SM⁴ and Singh M⁵
¹National Institute of Ayurveda, India ²Department of Rachana Sharir, Faculty of Ayurveda, India ³National Institute of Ayurveda, India ⁴Cancer Consultant Unit, National Institute of Ayurveda, India ⁵National Institute of Ayurveda, India Keywords: Arbud; Ayurveda; Granthi; Adenoma Carcinoma of Lung Disease
Abbreviations
SCLC: Small-Cell Lung Cancer; NSCLC: Non-Small Cell Lung Cancers; ALK: Anaplastic Lymphoma Kinase.
Introduction
Lung cancer, a malignancy originating in the lungs, remains the leading cause of cancer-related mortality globally and is projected to retain this position for the foreseeable future. The lungs, vital organs responsible for oxygen intake during inhalation and carbon dioxide release during exhalation, are highly susceptible to malignant transformations. According to the Globacon report 2018, lung cancer accounted for approximately 2.1 million new cases (11.6% of all cancers) and 1.8 million deaths (18.4% of all cancer-related fatalities) worldwide. In India, the same report documented 67,795 new cases of lung cancer (5.9% of all cancers) and 63,475 deaths (8.1% of all cancer-related deaths), with a higher prevalence among males (48,698 cases, 8.5%) [1, 2]. Lung cancer is broadly categorized into two main types based on cellular origin: Small Cell Lung Cancer (SCLC) and Non-Small Cell Lung Cancer (NSCLC). NSCLC is further subdivided into adenocarcinoma, squamous cell carcinoma (SCC), and large cell carcinoma, among others. The 2015 World Health Organization (WHO) classification also recognizes neuroendocrine tumors, including SCLC, large cell neuroendocrine carcinoma (LCNEC), and carcinoid tumors, as significant subtypes [3].
Carcinoid tumors arise from well-differentiated neuroendocrine cells, while SCLC originates from poorly differentiated neuroendocrine cells, characterized by rapid metastasis, limited therapeutic response, and poor prognosis. Squamous cell carcinoma and SCLC are predominantly central in location and strongly associated with smoking, particularly among males. In contrast, adenocarcinoma, the most prevalent lung cancer subtype, tends to arise peripherally, is more common in women and non-smokers, and often harbors targetable genetic mutations such as Epidermal Growth Factor Receptor (EGFR), Anaplastic Lymphoma Kinase (ALK), BRAF, and ROS1 rearrangements [4].
This paper explores the epidemiological trends, molecular classification, and clinical challenges associated with lung cancer, with a specific focus on adenocarcinoma, emphasizing the importance of developing effective therapeutic strategies to improve patient outcomes.
India is the second largest consumer and the third largest producer of tobacco globally. Approximately 28.6% of the Indian population uses tobacco products, with a higher prevalence among men (42.4%) compared to women (14.2%), amounting to an estimated 267 million users nationwide. Tobacco consumption is a significant contributor to lung cancer, which accounts for 5.9% of all cancers and 8.1% of all cancer-related deaths in India. Among lung cancer patients, the prevalence of smoking is estimated to be nearly 80% [5].
In Ayurvedic literature, conditions such as Shotha, Granthi, Arbuda, Apachi, Gulma, and Vidradhi exhibit clinical manifestations comparable to modern descriptions of neoplasms or tumors. According to Charaka Samhita and Sushruta Samhita, swelling (Shotha) is identified as the initial symptom of such conditions. Neoplasms in Ayurveda are categorized as inflammatory or non-inflammatory swellings, referred to as Granthi (small neoplasm) or Arbuda (major neoplasm). Acharya Sushruta describes neoplasms as round, fixed, mildly painful, large, broad-based, slowly progressive, and non suppurative swellings caused by the vitiation of Doshas and their impact on body tissues [6]. Acharya Vagbhata further delineates that Arbuda is larger than Granthi and can develop into a tumor over time [7].
Unlike the reductionist approach of modern medicine, Ayurveda adopts a holistic framework, addressing the interconnectedness of life, health, and disease. Although lung cancer is not explicitly described in Ayurvedic texts, its clinical presentation aligns with conditions affecting the Pranavaha Srotas (respiratory system) [8]. Consequently, diagnosis and management can be approached using foundational Ayurvedic principles.
This article presents a case report on the successful management of non-small cell lung carcinoma (NSCLC) through standalone Ayurvedic treatment, highlighting its potential as a complementary or alternative therapeutic modality.
Case Presentation
Patient History
A 70 year old male presented to the Cancer Outpatient Department (OPD) at NIA Hospital, Jaipur, in October 2018, with a history of bronchial asthma and a 25-year history of tobacco (Bidi) addiction. His chief complaints included a persistent dry cough, severe left-sided chest and back pain (Parshvshoola), difficulty in breathing (Shwashakrichchhita), and symptoms persisting for the past three years. Additionally, the patient reported unintentional weight loss of approximately 8 kg over one year, generalized weakness (Daurbalya), and loss of appetite (Aruchi). There was no relevant family history or prior significant medical history.
Clinical Examination
On systemic examination, there was no evidence of icterus, cyanosis, clubbing, or pallor. The cardiovascular and central nervous systems were within normal limits. However, respiratory system examination revealed rhonchi sounds in the upper left lung and wheezing sounds in the lower right lung. Vital signs included a blood pressure of 120/80 mmHg and a pulse rate of 78 beats per minute. The patient’s height was 170 cm, body weight was 51 kg, and his body mass index (BMI) was calculated at 17.6 kg/m², indicating undernutrition.
Radiological Findings
Contrast-enhanced computed tomography (CECT) of the thorax revealed: • A soft tissue density mass measuring approximately 43 × 41 × 40 mm with contrast enhancement and spiculated margins in the lower lobe of the left lung, closely abutting the major fissure with a peripheral desmoplastic reaction suggestive of a neoplastic lesion.
• Enlarged pretracheal, paratracheal, subcarinal, and aortopulmonary (AP) window lymph nodes, with the largest node measuring 20×10 mm.
Histopathological Findings
Biopsy of the lesion confirmed the diagnosis of lung adenocarcinoma.
Therapeutic Interventions
Ayurvedic treatment was initiated on December 11, 2018. At the time of treatment initiation, the patient reported occasional cough with white sputum, constipation, and persistent difficulty in breathing. Further observations and outcomes related to the therapeutic interventions documented in subsequent follow-ups (Table 1).
| Sl.No | Medicine | Dose | 11-12-2018 | 21/01/2019 | |
|---|---|---|---|---|---|
| 1 | Arbud Har Kashaya | 5gm | With water, 40 ml BD, Before Food | + | + |
| 2 | Swarna Basant Malati Rasa Abhrak Bhasma Shringh Bhasma Heerak Bhasma | 125mg 125mg 125mg 5mg | With Honey | + | - |
| 3 | Pushkar moolchoorna Laxmi vilaas Rasa Swash Kuthar Rasa Sitopladichoorna Yastimadhuchoorna Tankan Bhasma | 5gm 125mg 125mg 2gm 2gm 2gm | With Honey | + | + Same as but removed Laxmivilas Rasa & Shwash Kuthar Rasa & Tankan Bhasma. Bhasma dose given 250 mg |
| 4 | Chitrak Haritki Avaleh | 5gm | With milk + Pippali | + | + 1 Pippali& 2.5 gm, Haridra Churna |
| 5 | Tab. Anacarcin | 1 BD | With milk | - | - |
Table 1: Observations and outcomes related to the therapeutic interventions documented in subsequent follow-ups
Diagnostic Assessment
The primary diagnostic tool utilized to monitor the disease status was a contrast-enhanced computed tomography (CECT) scan of the thorax (Table 2). This imaging modality was employed to evaluate the patient’s disease condition both prior to and following the initiation of treatment, providing critical insights into the progression or regression of the pathological changes (Figure 1).
| Sl No. | Date | Computed tomography (CECT) scan of the thorax |
|---|---|---|
| 1 | 18-10- 2018 | The imaging study revealed a soft tissue density mass measuring approximately 43 × 41 × 40 mm in the lower lobe of the left lung. The mass demonstrated contrast enhancement with spiculated margins and was located in close proximity to the major fissure, accompanied by a peripheral desmoplastic reaction suggestive of a neoplastic process. Additionally, enlarged lymph nodes were noted in the pretracheal, paratracheal, subcarinal, and aortopulmonary (AP) window regions, with the largest lymph node measuring 20 × 10 mm. |
| 2 | 22-05- 2019 | The imaging study demonstrated a heterogeneous, enhancing lobulated mass lesion measuring approximately 38 × 37 × 38 mm in the lower lobe of the left lung. The lesion extended beyond the major fissure, raising suspicion for mitotic carcinoma of the lung. Two calcified pulmonary nodules were identified in the right upper and lower lobes. Ground-glass haziness was observed in the apical segment of the right upper lobe. Additionally, minimal para-septal thickening and prevascular lymphadenopathy were noted. Bilateral paratracheal, sub-aortic, para-aortic, sub-carinal, and hilar lymph nodes were detected, with the largest lymph node measuring approximately 10 × 8 mm. |
Table 2: Computed tomography (CECT) scan of the thorax.
Result
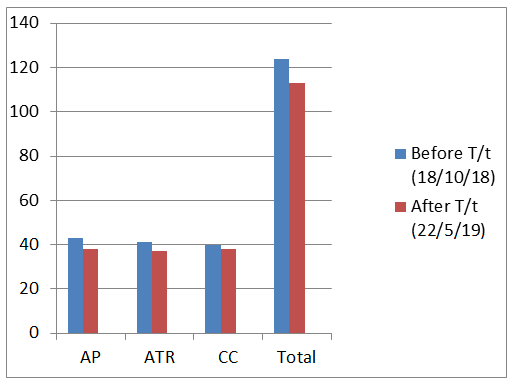
| S.no. | CECT Thorax | Before treatment | After treatment (22/05/19) |
|---|---|---|---|
| (18/10/18) | |||
| 1 | AP (Anteroposterior) | 43 mm | 38 mm |
| 2 | TR (Transverse) | 41 mm | 37 mm |
| 3 | CC (Craniocaudal) | 40 mm | 38 mm |
| 4 | TOTAL | 124 mm | 113 mm |
Table 3: Disease condition of the patient before and after treatment.
Discussion
Lung cancer, particularly adenocarcinoma, remains a leading cause of cancer-related mortality worldwide, with tobacco smoking recognized as a major etiological factor. This case report details the clinical course of a 70-year-old male diagnosed with adenocarcinoma of the lung, who was managed using an Ayurvedic treatment protocol. The patient had a significant history of bronchial asthma and 25 years of tobacco use and presented with symptoms including dry cough, chest pain, dyspnea, and general weakness. Diagnostic evaluations, including a CECT thorax scan, revealed a significant mass in the left lung, with biopsy confirming adenocarcinoma.
Conventional lung cancer treatments typically involve chemotherapy, radiotherapy, and surgical intervention. In this case, however, the patient underwent Ayurvedic management as an alternative approach. The treatment protocol included herbal formulations such as Arbud Har Kashay, Swarna Vasant Malti Ras, Abhrak Bhasma, and Pushkar Mool Choorna, formulated based on Ayurvedic principles. These interventions align with the Ayurvedic concept of Pranavaha Srotas dysfunction, which relates to disorders of the respiratory pathways, including conditions comparable to lung cancer.
A noteworthy observation in this case was the reduction in tumor size following Ayurvedic intervention. Serial CECT scans documented a decrease in the mass dimensions from 43 × 41 × 40 mm to 38 × 37 × 38 mm. This regression occurred without the application of standard oncological therapies, suggesting a potential influence of the Ayurvedic regimen on disease progression. Additionally, improvements in systemic symptoms, including appetite and general weakness, were reported, indicating enhanced quality of life.
While these outcomes are encouraging, this case represents an isolated clinical scenario and should be interpreted with caution. The absence of conventional cancer therapies limits the ability to generalize these findings or definitively attribute tumor regression to Ayurvedic treatment. Moreover, the mechanisms through which the Ayurvedic formulations exerted their effects remain speculative and warrant further investigation.
This report highlights the potential role of traditional medicine in cancer management, particularly in resource- constrained settings where access to modern therapies may be limited. However, rigorous scientific evaluation, including controlled clinical trials, is essential to validate the efficacy and safety of Ayurvedic treatments for lung cancer. Integrating traditional knowledge with modern oncological research could pave the way for more comprehensive and holistic treatment strategies, potentially benefiting patients worldwide.
Conclusion
Ayurvedic medicine holds significant potential for the diagnosis and management of both known (Ukta) and unknown (Anukta) diseases, including cancer, through the application of its fundamental principles. In this case, a patient with adenocarcinoma of the lung was successfully treated using an Ayurvedic approach without the use of conventional therapies. This outcome suggests that Ayurvedic interventions may offer a viable complementary treatment option in cancer care, particularly in settings where access to standard oncological treatments is limited. Further research is necessary to confirm the efficacy of Ayurvedic protocols in cancer management and to explore the underlying mechanisms of action. References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, et al. (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 68(6): 394- 424.
2. Fitzmaurice CH, Abate D, Abbasi N, Abbastabar H, Abd- Allah F, et al. (2019) Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life- Years for 29 Cancer Groups, 1990 to 2017: a Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol 5(12): 1749-1768.
3. Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Austin JHM, et al. (2015) The 2015 World Health Organization classification of lung tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J Thorac Oncol 10(9): 1243-1260.
4. Denisenko TV, Budkevich IN, Zhivotovsky B (2018) Cell death-based treatment of lung adenocarcinoma. Cell Death Dis 9(2): 117.
5. Owen DH, Ismaila N, Freeman-Daily J, Roof L, Singh N, et al. (2024) Therapy for Stage IV Non–Small Cell Lung Cancer With Driver Alterations: ASCO Living Guideline, Version 2024.1. Journal of Clinical Oncology 42(20): e44-e59.
6. Shashtri KA. Sushrut Samhita. Chaukhamba Sanskrita Sansthan, Chikitsa Sthana, India, 1: 18.
7. Tripathi B (2022) Astanga Hridya. Chaukhambha Sanskrit Pratishthan, Uttartantra, India, 30: 84.
8. Tripathi B (2022) Astanga Hridya. Chaukhambha Sanskrit Pratishthan, Nidanasthana, India, 4.
9. Rastantra Sar Evam Siddha Yoga Samgraha. Pratham Khanda Kharaleeya Rasayan, 34: 185.
10. Tripathi B (2022) Charaka Samhita. Chaukhambha Sanskrit Pratishthan, Vimanasthana, India, 5.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results