Isolated Sustentaculum Tali Fracture in Polytrauma Patient
Introduction: An isolated sustentaculum tali fracture is a rare manifestation of orthopaedic injury involving the supporting bone of the middle calcaneal facet. Globally, the incidence is estimated to be less than 1% of all calcaneus fractures. Presentation of Case: We reported a 21-year-old man with multiple injury including; comminuted displaced fracture of zygomatic maxillary area at the left orbit, left distal radius fracture, right femur segmental fracture and isolated left calcaneus sustentaculum tali fracture. An open reduction and internal fixation procedure was performed to fix the isolated sustentaculum tali fracture using cannulated cancellous screw. The subjective postoperative evaluation showed that the patient responded well and gradually returned to daily routine activities without pain or instability. Discussion and Conclusion: Surgical approach using the cannulated cancellous screw to establish a firm fixation of sustentaculum tali fracture fragment into calcaneus bone showed excellent result with good healing.
Abbreviations
ORIF: Open Reduction Internal Fixation; CRIF: Closed Reduction Internal Fixation.
Introduction
Fracture of the sustentaculum tali of the calcaneus is relatively uncommon injury that can occur as a result of trauma or high-energy forces applied to the foot and ankle [1]. Solitary fractures of the sustentaculum tali without additional calcaneal injuries occur in less than 1% of all calcaneal fractures due to the strong trabecular structure and thick cortical bone, and are therefore frequently disregarded [2, 3, 4, 5, 6]. It frequently associated with foot fractures, midtarsal dislocations, or subtalar dislocations. There are not many published series, and the majority of articles only contain case reports [1, 7]. Patients consistently express pain that is distal and anterior to the medial malleolus, and that is made worse by passive motion of the flexor hallucis longus tendon. Clinically, an ecchymosis region is visible above the sustentaculum [8]. The appropriate surgical therapeutic strategy for sustentaculum tali fractures is still up for debate [9]. Additionally, improper management shows the potential for long-term problems that could result in chronic disability and impair the patient’s quality of life [10].
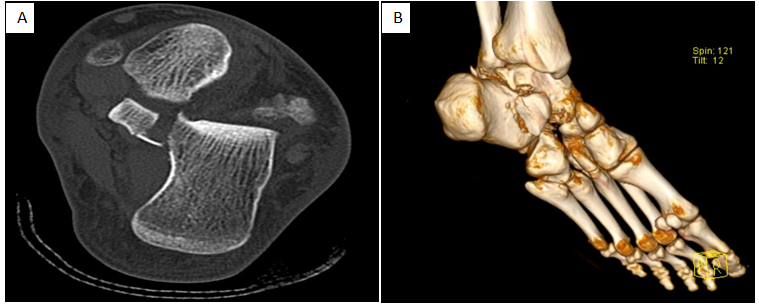
21 years old male medically free was referred from another hospital by red crescent after sustaining a motor vehicle accident with rollover. On assessment, he was Conscious, alert and Oriented. Glasgow comma scale 15/15. Patient has multiple injury including, comminuted displaced fracture of zygomatic maxillary area at the left orbit, left distal radius fracture, right femur segmental fracture and left calcaneus sustentaculum tali fracture. CT chest showed right-sided pneumothorax where chest tube was inserted. The patient underwent Maxillofacial fracture open reduction internal fixation (ORIF), right segmental femur fracture (ORIF) with retrograde nailing, and left distal radius closed reduction internal fixation (CRIF) with Kirschner wire. Finally, he underwent a left calcaneus sustentaculum tali fracture (ORIF).
Surgical Intervention
Patient was in Supine position under spinal anesthesia, tourniquet applied for 300 mm/hg. The center of the incision was 2 cm beneath the medial malleolus and 2 cm proximal to the navicular for about 5 cm in length, following the neurovascular structures. For superficial dissection, the posterior tibial tendon, the neurovascular bundle and the flexor hallucis tendon identified. The interval between the neurovascular bundle, specifically the posterior tibial nerve and the flexor hallucis tendon, which is retracted distally. Retinaculum incised and the sustentaculum tali felt underneath it.
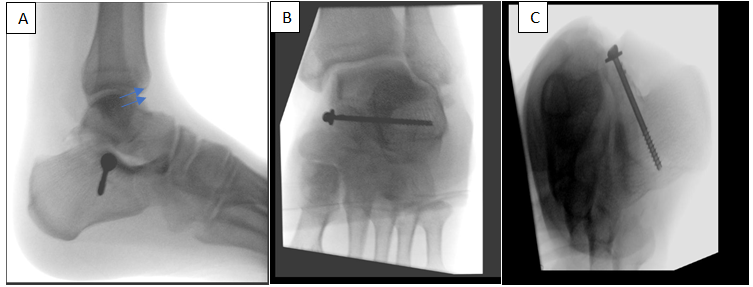
It is immediately above the flexor hallucis tendon. For deep dissection, The sustentaculum tali is a bony prominence which is obvious once one is beneath the medial neurovascular structures. Fracture reduced indirectly with help of image intensifier (C-ARM) and held in place by k-wire, then another k-wire for cannulated screw size 4.5 mm was used, drilling done and 4.5mm partially threaded cannulated screw with washer was inserted.
Finally, wound irrigation and closure layer by layer after hemostasis. Dressing and backslap below knee were applied. The procedure went uneventfully (Figures 1-3).

Discussion
Isolated fracture of the sustentaculum tali is an infrequent injury. Rarity of this injury makes it the central problem to diagnose and establish right management approach [9, 10]. On a functional level, the symptoms are easily classified as pain locally around the medial malleolus, with a history of trauma [11]. Moreover, most of these patients also lost the ability to walk normally [12]. On physical examination, point tenderness with possible skin changes over the medial malleolus [12]. In our unique situation, the unyielding lack of stability could potentially be linked to the displaced fracture, whether accompanied by the complex issue of ruptures in the talocalcaneal ligaments on either side. A three-dimensional CT scan offers a superb, top-notch reconstruction image that aids in diagnosing anatomical components [13]. A surgical approach through the medial incision by utilization of cannulated cancellous screw fixation is the preferred method due to the inherent obstruction of the fracture line by the intact calcaneal tuberosity as compared with employing the lateral approach [13]. McReynolds, renowned for pioneering the medial approach for ORIF of sustentaculum tali fracture, lends credence to this rationale [14]. Additionally, Durr et al. substantiate the efficacy of this approach with statistically significant results in clinical outcomes, gauged by the mean AOFAS Ankle and Hindfoot scale. Furthermore, the implementation of the medial technique facilitates enhanced direct visual perception through a small incision, leading to a heightened restoration of the calcaneus’ biomechanical capabilities. This, in turn, mitigates the likelihood of post-traumatic arthritis, culminating in an approach of unparalleled dependability [15]. Alternatively, in contrast, Gitajn et al. claimed that the decision to utilize surgical methods, such as medial or lateral approaches, is frequently influenced by the surgeon’s familiarity with these techniques, as the indications for their implementation remain limited in available literature [12, 16]. Utilizing a cannulated screw is imperative, with precise placement of approximately 40 mm in length, commencing 15 mm below the posterior facet of the subtalar joints [17]. This meticulous approach guarantees a robust fixation of the fracture, effectively restoring the fracture fragments to their anatomical alignment, rectifying the Bohler angle and hind leg varus, as well as alleviating subtalar joint dislocation [18]. In present comparative analyses pertaining to the use of a screw versus a plate, no discernible variation in biomechanical results was observed [19]. The consequences of insufficient care for fractures of the sustentaculum tali can be classified into two categories: early and late complications. Early complications typically include tarsal tunnel syndrome and damage to the flexor hallucis longus tendon, while post-traumatic arthritis is a frequently observed late complication [20, 21].
To our knowledge, the case represents the first case in our hospital to present with isolated sustentaculum tali fracture in addition to polytrauma he suffered as orthopedic and non-orthopedic injuries. What makes it unique also is high-energy trauma with a rotational mechanism. Thankfully, the orthopedic surgeon was able to successfully treat the patient, resulting in a highly favorable outcome. While it is recommended that the patient be monitored for at least a 6months post-treatment, it would be beneficial to conduct further research with a more extensive follow-up period to better evaluate the optimal surgical approach.
References
-
Gatha M, Pedersen B, Buckley R (2008) Fractures of the sustentaculum tali of the calcaneus: a case report. Foot & ankle international 29(2): 237-240.
-
Germann CA, Perron AD, Miller MD, Powell SM, Brady WJ, et al. (2004) Orthopedic pitfalls in the ED: calcaneal fractures. The American journal of emergency medicine 22(7): 607-611.
-
Dürr C, Zwipp H, Rammelt S (2013) Frakturen des Sustentaculum tali. Operative Orthopädie und Traumatologie 25: 569-578.
-
Marks R, Antoniades S, Myerson M (1996) Injury to the sustentaculum tali. The Foot 6(4): 182-187.
-
Myerson MS, Berger BI (1995) Nonunion of a fracture of the sustentaculum tali causing a tarsal tunnel syndrome: a case report. Foot & Ankle International 16(11): 740-742.
-
Rammelt S, Winkler J, Grass R, Zwipp H (2006) Reconstruction after talar fractures. Foot and Ankle Clinics 11(1): 61-84.
-
Zaraa M, Jerbi I, Mahjoub S, Sehli H, Mbarek M (2017) Irreducible subtalar dislocation caused by sustentaculum tali incarceration. Journal of Orthopaedic Case Reports 7(1): 58-60.
-
Al-Ashhab ME, Elgazzar AS (2018) Treatment for displaced sustentaculum tali fractures. The Foot 35: 70- 74.
-
Razik A, Harris M, Trompeter A (2018) Calcaneal fractures: Where are we now? Strategies in Trauma and Limb Reconstruction 13: 1-11.
-
Radley JM, Nicolaou DA (2019) Bilateral isolated fracture of the sustentaculum tali: A Case Report JBJS Case Connect. 9(2): 1-5.
-
Agha RA, Borrelli MR, Farwana R, Koshy K, Fowler A, et al. (2018) Orgill, For the SCARE Group, The SCARE 2018 statement: updating consensus Surgical Case Report (SCARE) guidelines. Int. J. Surg. 60: 132-136.
-
Della Rocca GJ, Nork SE, Barei DP, Taitsman LA, Benirschke SK (2009) Fractures of the sustentaculum tali injury characteristics and surgical technique for reduction. Foot Ankle Int 30(11): 1037-1041.
-
Rao F (2021) Application of magnetic resonance imaging in evaluating ankle motion injury. Rev. Bras. Med. Esporte 27(3): 253-256.
-
McReynolds IS (1982) The case for operative treatment of fractures of the os calcis. In: Leach RE,. Houaglund FT, Riseborough EJ (Eds.), Controversies in Orthopaedic Surgery, Philadelphia, Saunders.
-
Durr C, Zwipp H, Rammelt S (2013) Fracture of the sustentaculum tali. Oper Orthop Traumatol 25: 569- 578.
-
Gitajn IL, Abousayed M, Toussaint RJ, Ting B, Jin J, et al. (2014) Anatomic alignment and integrity of the sustentaculum tali in intra-articular calcaneal fractures: Is the Sustentaculum Tali Truly Constant?. J Bone Joint Surg Am 96(12): 1000-1005.
-
Phisitkul P, Sullivan JP, Goetz JE, Marsh JL (2013) Maximizing safety in screw placement for posterior facet fixation in calcaneus fractures: a cadaveric radio- anatomical study. Foot Ankle Int 34(9): 1279-1285.
-
Basa CD, Sariekiz E, Kacmaz IE, Er A, Zhamilov V, et al. (2020) Definition of sustentacular screw length based on computed tomography measurements for calcaneus intraarticular fracture surgery. J DEU Med 34(3): 203- 207.
-
Qiang MF, Singh RK, Chen YX, Zhang K, Jia XY, et al. (2019) Computational biomechanical analysis of postoperative calcaneal fractures with different placement of the sustentaculum screw. Orthop Surg 12(2): 661-667.
-
Mu H, Xiangyang X, Gang B (2014) Isolated fractures of the sustentaculum tali: injury characteristics and surgical technique for reduction management. J Foot Ankle Surg (Asia-Pacific) 1(2): 48-51.
-
Moonot P, Sharma G, Kadakia AR (2021) Mal-union of sustentaculum tali fracture with talo-calcaneal coalition leading to tarsal tunnel syndrome: a case report.The Foot 47: 101797.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results