Desinfection Policy and Infections Associated with Healthcare in Neurologic Patients
Introduction: The problems surrounding healthcare associated infections is a necessity of governments and in particular for each health center, which better guides prevention actions, control and continuous adjustment of disinfection policy according to hospital infection rates. Objectives: To demonstrate the trend of HAIs and key factors that influence their control, emphasizing the continuous adjustment of disinfection policies over a period of five years, establishing a forecast for the 2020-2022 triennium. Methods: a descriptive, longitudinal and retrospective study of the HAIs was carried out at the Institute of Neurology and Neurosurgery of Cuba during the 2015-2019 five-year period, according to the disinfection policy and the actions carried out to raise the quality of the HAIs control program, calculating values forecasts through the least squares method. Results: during 2015-2019 rates of HAIs between 3.76 and 6.42 were maintained, with a prognostic estimate for the triennium 2020-2022 of a rate between 1.60 and 2.93, with a strong downward trend, maintaining the current mechanical and environmental disinfection policy established. Bacterium colonizations related to assisted mechanical ventilation prevailed in 34% of the patients and urinary tract infections in 25%, varying these data per year with a clear decrease of up to 18 percentage points according to the HAIs type. Conclusions: it is possible to implement a prospective in-hospital sepsis surveillance system in neurological patients, to increase the quality of the care process, establish prognoses and evaluate the impact of the disinfection policies used.
Introduction
Healthcare-associated infections (HAI) are defined as a localized or systemic process, the result of the adverse reaction to the presence of an infectious agent or its toxins; which was not present or incubated at the time of admission to a health institution. The corresponding clinical manifestations can manifest within 48 to 72 hours after admission and even within 10 days after the patient has been discharged; also including occupational infections contracted by health personnel [1, 2, 3, 4].
HAI are the most frequent adverse event during health care, no institution or country can claim that it has solved this problem; its true global burden is not yet known exactly due to the difficulty of collecting reliable data; most countries lack a system for its surveillance; and those who have it are confronted with the complexity and lack of uniformity of the criteria for diagnosing them [3].
In North America, data from Canada indicate that about 220,000 hospital infections are contracted annually, resulting in 8,000 deaths related to that cause. In the United States, they are among the leading causes of death in the country, it is estimated that they cause up to 99,000 deaths per year [4]. In Latin America, despite the fact that HAI are a major cause of morbidity and mortality, the economic and care burden produced by these infections is unknown. Some countries such as Uruguay, Argentina and Chile have adequate monitoring of HAI in their services, with institutional and national data; however, the objectives, indicators, definitions and methodologies vary between them [5]. In Cuba, despite having a national system for the prevention and control of HAI, they represent a health problem. The epidemiological surveillance of the HAI in its latest report reflects an overall rate that ranged from 2.6 to 3.4 per 100 graduates, with an annual average of 25,000 infected over a 10-year period [6]. These conditions cost the country more than three million pesos per year and their mortality represents between 1 and 3% of the patients admitted [7].
The few studies in Cuba that address this issue and related survival, compare healthy subjects with those who have infections, without knowing exactly the variability of the costs of managing AAS according to the specific characteristics of the patients, microorganisms and the need for intensive care due to the infectious process [8, 9, 10]. The additional concern to this problem is that, accepting that HAI are an adverse event, 30% of them are preventable [11, 12]. The problem surrounding HAI is a need of governments and in particular of each health center, so our goal is to evaluate the effectiveness of the disinfection policy used for 5 years in a neurological care center.
Methods
A longitudinal and retrospective descriptive study of the HAI was carried out at the Institute of Neurology and Neurosurgery of Cuba during the five-year period 2015- 2019 to evaluate the effectiveness of the disinfection policy according to the modifications made in the disinfection methods according to the hygienic health situation of the five-year period. The main purpose was, based on the known data, to establish the forecasts and trends for the 2020- 2022 triennium of some indicators such as the number of infected cases and global rates of in-hospital sepsis, in addition to evaluating the effectiveness of the disinfection policy implemented at the center. Some indicators of the AAS prevention and control program were analyzed, such as the total number of samples studied by Microbiology, their positivity and the most frequent causal agents. The behavior of these indicators in the five years studied, the prognostic values of infected cases and the rate of HAI from 2020 to 2022 were described. To obtain the primary data, the reports of nosocomial infections in the Department of Medical Statistics and the reports of the Infections Committee, the reports of the hygienic health status of the center during the period and the interventions carried out were reviewed.
The following variables were analyzed:
- Total expenditures per year in the institution
- Total income from services
- Total number of septic patients, number of infections and their location in addition to isolated germs in the post-surgical period.
The records of the Infections Committee were reviewed with the aim of obtaining data relating to hospital microbiology (total samples studied, positivity and type of agent).
Statistical Processing of the Data
Taking the primary data All the data was recorded in a form prepared for this purpose and the surveys processed in a computerized way through the Statistic program; Microsoft Excel was used to make the charts.
As for the forecasts, the linear regression equation was used and the quadratic minimums method, with which the future value is predicted, starting from the linear trend and using the existing values of the straight line, after having obtained the regression coefficient for the variable studied (cases infected by services). The results are presented in tabular and graphical form and percentages are used for qualitative variables; absolute numbers, percentages, rates, arithmetic mean and standard deviation for quantitative variables.
Main typologies of HAI [13].
There are four main types of HAI, all associated with invasive or surgical procedures. They are:
- Urinary tract infection associated with catheter use (ITU-CA)
- Pneumonia associated with fan use (NAV)
- Surgical site infection (ISQ)
- Catheter-associated bloodstream infection (STI-CVC) Disinfection of surfaces by chlorine, alcohol, and other chemicals, such as surfanius and stambimed, was maintained, in addition to propelynglicon, used by vaporizations, after the general mechanical disinfection of the premises, associating environmental disinfection with ozone.
During the installation of the ozone equipment for environmental disinfection, the areas that carried out the greatest number of procedures in the care process were selected: Surgical unit with its three operating rooms and surrounding areas, recovery room and the Intensive Care Unit with all its premises (two rooms and one central room, sterile material storage area and nursing office). Areas with difficulty in environmental hygiene due to humidity and fungal growth were included (Department of Field of View of the Neurophthalmology office and the sterile material warehouse of the sterilization department).
An ASP ozonator, model SP-MINI, was installed in the Surgical Unit, for the production of 2 grams of ozone and capacity to cover a maximum volume of 1600 m3, sufficient to cover the area corresponding to the Surgical Unit and the Intensive Care Unit (ICU). The SP-MINI stays on 24 hours a day. It was configured to alternate 45-minute ozone generation cycles, with 15-minute downtime cycles.
Due to the distant and isolated location of the Ophthalmology Service and the complex structural barriers to overcome to reach the Sterilization Center, an ASP ozonator was placed in each of these services; the sterilization ozonator was a Z6000 Turbo model for the production of 75 mg of ozone per hour, and in ophthalmology, a Z3000 During their operation, they alternate ozone generation cycles, with cycles of inactivity (15 minutes without generation for 45 minutes of generation). The ozone generated is spread directly to the environment by the equipment [14].
The microbiological control was carried out by affecting the air sampled on a culture medium of Agar soybean tripticase and Agar saboreaud determined with Chloramphenicol, depending on whether bacteria or fungi are intended to be evaluated. Subsequently, incubation is carried out at an appropriate temperature and finally, the colony count is carried out, expressing the result in colony- forming units per cubic meter (ufc/m3). The volume of air sampled in each unit is equivalent to 100 liters.
All the media used have references according to the batch used, as well as expiration date and quality control certificate.
The system is described by the INSHT and adapted to the requirements of “Regulations for medicines and European Community Vol IV”. Standard AFNOR G 07 - 172, draft European standard CEN/TC 243/WG2, the culture medium is in accordance with AFNOR G 07 - 172; accredited method INTE-ISO/IEC 17025:2005.
The ozone measurement was carried out by the composition of a series of measurements of ozone inmission levels at different points of the premises, according to the provisions of UNE 400-201-94 Ozone generators. Air treatment Chemical safety.
Evaluations of germ count measurements were carried out before installing the system and then every six months.
Analysis of the Information
For device-associated infections, the incidence rates per 1000 device days in each type of infection (pneumonia associated with assisted mechanical breathing, bloodstream infection associated with central catheter and symptomatic infection of the urinary tract associated with urinary catheter), The percentages of device utilization by type of device (fan, central catheter, urinary catheter) and by type of care unit applying the following formulas: Number of new cases of device-associated infections in the intensive care unit.
Ethical Considerations
Given that collective information was collected and analyzed and that the results are intended to generate actions that contribute to the prevention and control of infections, the study was classified as a risk-free investigation and no informed consent was required in accordance with the scientific, technical and administrative standards for health research of the Ministry of Health of the Republic of Cuba. The handling of the data was adjusted to strict confidentiality parameters in accordance with current laws.
Results
| Parameters | 2015 | 2016 | 2017 | 2018 | 2019 | Mean | Standard deviation |
|---|---|---|---|---|---|---|---|
| Infected cases | 74 | 81 | 52 | 54 | 44 | 57,91 | 12,88 |
| Total number of infections | 96 | 103 | 62 | 64 | 59 | 67,66 | 13,43 |
| Infection rate | 6,42 | 5,93 | 3,76 | 3,84 | 3,85 | 4,50 | 1,07 |
| Deceased | 24 | 43 | 32 | 34 | 17 | 27,11 | 8,17 |
| Infected deceased | 6 | 9 | 6 | 13 | 3 | 5,85 | 3,14 |
| Samples taken | 153 | 126 | 71 | 75 | 79 | 91,66,15,088 | 30,16,17,676 |
| Positive samples taken | 103 | 118 | 70 | 74 | 76 | 84,54,45,229 | 17,32,01,974 |
Table 1: Parameters related to HAI in the Institute of Neurology and Neurosurgery during the period 2015-2019.
Source: Reports of hospital movement of medical records by year, medical records, registration of cases by services and analysis of the HAI control committee of the INN (2015-2019). Table 1: Parameters related to HAI in the Institute of Neurology and Neurosurgery during the period 2015-2019.
The cases infected in the INN during the years from 2015 to 2019 were counted between 44 and 81 cases, corresponding to the years 2016 and 2019 respectively. The infection rate in 2015 was 6.42%, stabilizing below 4% from 2017. The deaths in 2018 were 13 for only three infected patients to die in 2019, of the total number of deaths, compared to 2018, which, out of 34 deaths in total, infected were 13. The samples taken during the quinquennium reported had high positivity, an example of which in 2017 of 71 taken 70 were positive, in 2018 of 75; 74 were positive and in 2019 of 79; 76 were positive.
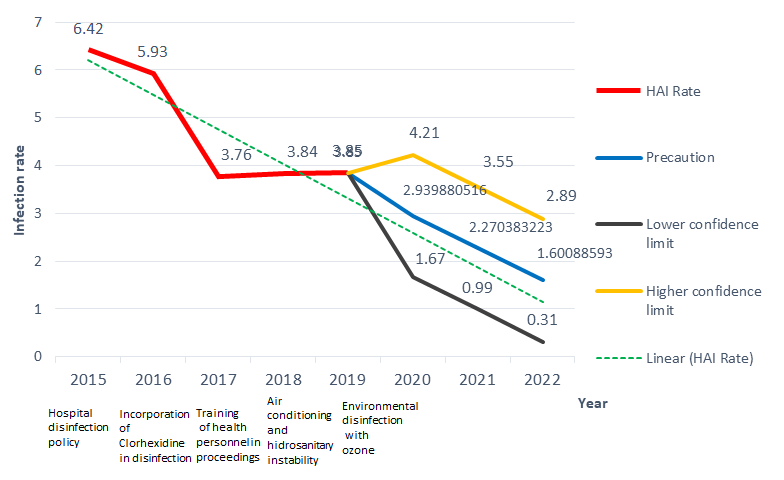
Source: Analysis report of the HAI control committee. Institute of Neurology and Neurosurgery by year of study 2015-2019. Figure 1: Hospital infection rate and prognosis according to the disinfection policy used.
It shows the trend in the infection rate in the INN, associated with the disinfection policy implemented and the modifications incorporated each year. During 2016, chlorhexidine was incorporated into the sanitization of patients prior to nursing and surgical procedures, in addition to having used it in mouthwash.
In 2017, training is initiated to respond to the training needs identified during the supervision carried out, and the deficiencies detected during the observation of the procedures in the services. During 2018, there were several alterations in the operation of centralized climate equipment and the hydrosanitary network, which forced the use of stored water, with the risk that this entailed.
In 2019, ozone equipment for environmental disinfection was installed in the most at-risk hospital areas and where the largest number of procedures were carried out.
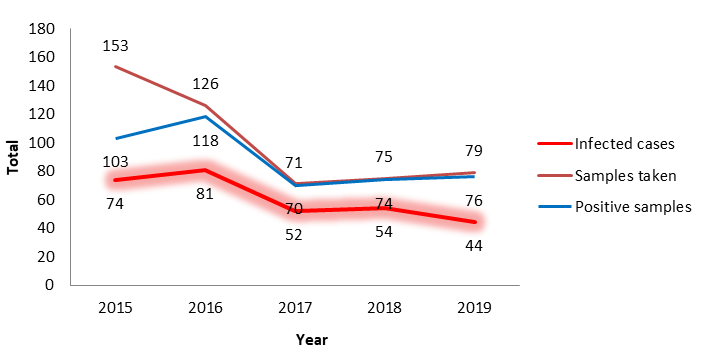
Source: Case records. Microbiological reports, analysis reports of the behavior of the HAI of the INN by year of the 2015-2019. Figure 2: Distribution of infected cases, samples taken and their positivity.
The infected cases, the total number of samples taken and those that were positive during the period 2015-2019 are represented. In 2015, 74 patients were infected and 153 samples were taken, of them 103 positive, in 2016 there were more infected cases (81) fewer samples were taken and the positivity was greater, which was maintained in 2017, 2018 and 2019 where the samples taken had a high correlation with the positive samples and correspond to almost all infected cases.
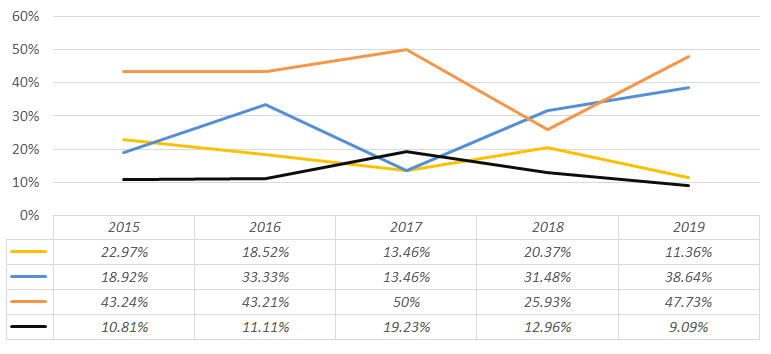
Source: Case records. Microbiological reports, behavioral analysis reports of the HAI of the INN by year of the 2015-2019 study. Figure 3: Percentage of the main microorganisms isolated in infections associated with health care.
The microorganisms that predominated during the study period were distributed by year: 2015: Staphylococcus coagulase positive in 4.2% of infected cases, followed by E. Coli at 22.9% 2016: Staphylococcus coagulase positive was maintained at 43.2% followed by Enterobacter at 33.3% 2017: Staphylococcus coagulase positive predominated in 50% of cases followed by Pseudomona aeruginosa in 19.2% 2018: Enterobacter with 31.5% and positive staphylococcus coagulase rose to second place with 25.9% 2019: staphylococcus coagulase positive again with 47.7% followed by Enterobacter with 38.6%
Discussion
The Institute of Neurology and Neurosurgery (INN) of Cuba was founded in 1966, and is currently the leading center of neurosciences in the country. The areas dedicated to care are distributed in clinical and surgical services for domestic and foreign patients of adult and pediatric age. It has a total of 72 beds distributed in Stroke Unit, Endovascular Therapy, Intensive Care, Neurosurgical and Neurological Care Services.
The measurement of epidemiological indicators, every day, becomes more important in the quality of care for the hospitalized patient, so that any hospital that exhibits stable work should not allow the overall rate of in-hospital infections in hospitalized patients to exceed 7% [15].
Our results show strong evidence of having maintained infection rates over a period of 5 years at values comparable to international standards, similar to that of countries with efficient in-hospital infection control programs. The disinfection policy is updated annually; comparing the results obtained each year with its previous period, and incorporating modifications to the disinfection policy according to the result of the analysis. The results were evaluated according to:
- Rates of hospital infection
- Isolated germs in microbiological samples taken from patients, professionals and other hospital workers.
- The results of the studies carried out in the environment by the surface sampling method with special emphasis on the Intensive Care Unit and operating rooms, because they are the areas where the greatest number of invasive procedures are carried out in the center.
The modifications that were introduced in the disinfection policy during the period studied were: the incorporation of Chlorhexidine in skin disinfection and mouthwashes in ventilated ones after regular cleaning, training for nurses in sampling for Microbiology and the use of Ozone to disinfect the environment. Regarding the use of Chlorhexidine, in the United States of America (USA), Darouiche and colleagues compared in 849 clean-contaminated surgeries the preparation of skin using an applicator of Chlorhexidine 2% on an alcoholic basis versus the application of soapy solution and then tincture of povidone iodized 10%. A significant difference was found in favor of chlorhexidine in the risk of superficial infection (4.2 vs 8.6%, p = 0.008 RR 0.48 CI 95% 0.28-0.84) and deep surgical site (1 vs 3%, p = 0.05, RR 0.33 CI 95% 0.11-1.01) at 30 days [16].
During 2018, the hygienic health situation of the center was affected by humidity and consequent growth of fungi on the walls of certain services and instability in the operation of the centralized air conditioning system. This epidemiological panorama led to the search for an environmental disinfection method, so in 2019 ozonation equipment was installed to disinfect the hospital environment in the areas with the highest number of infected cases and where the environmental status due to fungus growth was compromised.
Very favorable results were observed at 6 months in the control of HAI evidenced in the count of colony-forming units by area, before and after the use of ambient ozone, varying from an unacceptable environment to a very clean environment, a decrease of 66.7% in the number of deaths compared to the previous year and without incidence of adverse effects according to Lara and collaborators [14].
The environment of health care facilities contains a diverse population of microorganisms, but only a few are virulent enough to cause disease. Because of this, the role of the environment in the development of IAAS has been of growing interest to the scientific community, evidenced in the Guidelines for the Control of Environmental Infections published in 2003 by the Center for Disease Control, hereinafter CDC and updated in 2019 [17].
90% of the IAAS are caused by Staphylococcus aureus, Streptococcus sp., Acinetobacter Sp., Staphylococcus coagulasa negative, Pseudomonas aeruginosa, Escherichia coli, Proteus mirabilis, Salmonella sp. and Kleb. This varies depending on the site of infection and geographical region [18].
We present gradual control of the positivity of microbiological samples to non-fermenting bacilli, with a gradual decrease of Pseudomona aeruginosa as the only exponent of this group present in the samples taken in the five-year period. These are frequent etiological agents of hospital-acquired infections and opportunistic pathogens in immunocompromised patients, exposed to invasive actions. The increase in IAAS has led to an increase in multidrug- resistant organisms, which hinders treatment, increases mortality and the cost of health care [19, 20, 21, 22, 23, 24]. Proper disinfection of surfaces, along with proper hand hygiene, is recommended to prevent the transfer of pathogens between health workers, and from these to patients [24, 25]. Visits represent a source of underdiagnosed contagion that can be avoided with education or prohibition of hospital access to visitors who manifest respiratory symptoms [26, 27].
Limitations of the Study
Carrying out the study in a single center, needing to extrapolate it to other hospitals.
Do not have the results of bacterial resistance in addition to the variability in the hygienic and sanitary conditions of the center, which do not allow the establishment of stable parameters of environmental quality.)
Conclusion
Our experience shows that it is possible to implement and adapt a prospective surveillance system for in-hospital sepsis in neurological patients, being necessary to extrapolate this experience to other centers with a similar function and manage to implement an automated surveillance system for IAAS, in direct relation to disinfection policies according to each center.
Conflicts of Interest
The authors declare that there are no conflicts of interest.
References
-
Klevens RM, Edwards JR, Richards CL, Horan TC, Gaynes RP, et al. (2007) Estimating Health Care-Associated Infections and Deaths in U.S. Hospitals, 2002. Public Health Rep 122(2): 160-166.
-
Ministerio de Salud (MINSA) Lime General Directorate of People’s Health. Guidelines for the surveillance, prevention and control of infections associated with health care. MINSA.
-
World Health Organization (2013) WHO Global burden of infections associated with health care.
-
Health Quality Ontario (2020) Portable Ultraviolet Light Surface-Disinfecting Devices for Prevention of Hospital- Acquired Infections: A Health Technology Assessment. Ont Health Technol Assess Ser 18(1): 1-73.
-
Organización Panamericana de la Salud (2011) Guía de evaluación rápida de programas hospitalarios en prevención y control de las infecciones asociadas a la atención de salud [Internet]. Washington, D.C, USA, pp: 1-28.
-
Cuba Salud (2018) [citado 12 ene 2021].
-
Arango Díaz A, López Berrío S, Vera Núñez D, Castellanos Sánchez E, Rodríguez Sanabria PH, et al. (2021) Epidemiology of healthcare-associated infections. Acta Med Centro 12(3): 262-272.
-
Ortiz Mayorga J, Pineda Rodríguez I, Dennis R, Porras A (2019) Costos atribuidos a las infecciones asociadas con la atención en salud en un hospital de Colombia, 2011- 2015. Bioméd 39(1): 102-112.
-
European Centre for Disease Prevention and Control (2019) Healthcare-associated infections: surgical site infections. In: ECDC. Annual epidemiological report for 2017. Stockholm: ECDC.
-
Aguilera Calzadilla Y, Díaz Morales Y, Guerra Martínez M, Sánchez Álvarez ML, Martínez Frometa M (2019) Aislamientos de Acinetobacter spp. en infecciones asociadas a la asistencia sanitaria. Rev Cubana Med Militar 48(3): 505-518.
-
Manual Latinoamericano de Guías Basadas en la Evidencia (2020) Estrategias para la Prevención de la infección Asociada a la Atención en Salud-ESPHAI- Surgical Infection Society Latin America. pp: 184.
-
Gudiol F, Limón E, Fondevilla E, Argimon J, Almirante B, et al. (2012) The development and successful implementation of the VINCat Program. Enferm Infecc Microbiol Clin 30(S3): 3-6.
-
Olaechea PM, Insauti J, Banco A, Luque P (2010) Epidemiology and impact of nosocomial infections. Med Intensiva 34(4): 256-267.
-
Lara Fernández GE, Ariosa Acuña CM, Borroto Rodríguez V, Puerta Armas A, Ortiz Hernández R, et al. (2020) Ozono como método de desinfección del ambiente hospitalario. Acta Médica Costarricense 62(2): 72-78.
-
Rivero LlonchI L, Álvarez Sánchez A, Ballesté López I, Villarreal Acosta A, Galbán Hernández O (2009) Tendencias y pronósticos de las infecciones hospitalarias y sus gastos asociados. Rev Cubana Obstet y Ginecol 35(4): 150‐156.
-
Diomedi A, Chacón E, Delpiano L, Hervé B, Jemenao MI, et al. (2017) Antiseptics and disinfectants: aiming at rational use. Recommendations of the Advisory Committee on Healthcare Associated Infections. Sociedad Chilena de Infectología. Rev Chil Infectol 34(2): 156-174.
-
Sehulster LM, Chinn RYW, Arduino MJ, Carpenter J, Donlan R, et al. (2003) Guidelines for environmental infection control in health-care facilities. Recommendations from CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC).
-
Mondelo García C (2018) Auditar y mejorar la profilaxis antibiótica quirúrgica. Universidad de Granada pp: 175.
-
González Abad MJ, Alonso Sanz M (2019) Vigilancia de multirresistentes: Enterococcus spp. resistente a vancomicina. An Pediatr (Barc) 91(4): 267-268.
-
Bradley CR, Ayliffe GAJ (2018) Hospital infections in Birmingham, England, in the 19th and 20th centuries. J Infect Prev 19(5): 240-243.
-
Peters A, Otter J, Moldovan A, Parneix P, Voss A, et al. (2018) Keeping hospitals clean and safe without breaking the bank; summary of the Healthcare Cleaning forum 2018. Antimicrob Resist Infect 7: 132.
-
Centers for Disease Control and Prevention (2019) Infection Control in Healthcare Personnel: Infrastructure and Routine Practices for Occupational Infection Prevention and Control Services.
-
Gutiérrez V, Cerda J, Le Corre N, Medina R, Ferrés M (2019) Caracterización clínica y epidemiológica de infección asociada a atención en salud por virus influenza en pacientes críticos. Rev Chilena Infectol 36(3): 274-282.
-
European Centre for Disease Prevention and Control (2017) Assessment of infection control, hospital hygiene capacity and training needs in the European Union, 2014. Stockholm: ECDC, pp: 1-44.
-
Pérez Faraldo B, González Isla F (2017) Infecciones por bacilos gramnegativos no fermentadores: agentes etiológicos de infecciones asociadas a la atención sanitaria. CCM 21(4): 1197-200.
-
Asensio Martín MJ, Hernández Bernal M, Yus Teruel S, Minvielle A (2018) Infecciones en el paciente crítico. Medicine 12(52): 3085-3096.
-
Davey P, Marwick CA, Scott CL, Charani E, McNeil K, et al. (2017) Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Sys Rev 2(2): CD003543.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda