Good News! Indigenous HPV Vaccine on Shelf by this Year End what India Must do to Hasten Cervical Cancer Elimination by 2030?
In May 2018, the WHO announced a global call for action to make elimination a reality and calling for all stakeholders to unite behind this common goal. Vaccination against HPV and screening and treatment of pre-cancer lesions are cost-effective ways to prevent cervical cancer. Human papillomavirus (HPV) vaccines, introduced in many countries in the past decade, have shown promising results in decreasing HPV infection and related diseases, such as warts and precancerous lesions. However currently, vaccine’s coverage, in low- and middle-income countries including India is very low to show any impact in the next 2-3 decades. Govt. of India had launched a National Cancer Control Programme in 1975, revised its strategies in 1984-85 and again under National Health Policy 2017. While it stresses on primary prevention for Tobacco related cancers, addresses only secondary prevention of cancer of the uterine cervix, mouth, breast etc. and tertiary prevention of therapeutic services including pain relief. Cervical cancer is the fourth most common cancer among women globally, with an estimated 604 000 new cases and 342 000 deaths in 2020. About 90% of the new cases and deaths worldwide in 2020 occurred in low- and middle-income countries. India accounts for about a fifth of the global burden of cervical cancer with about 1.25 Lakh cases and 67,000 deaths every year. Cervical cancer in India ranks as the second most frequent cancer among women between 15 and 44 years of age. Most cervical cancers are associated with human papillomaviruses, a sexually transmitted disease. HPV vaccination has been attempted in the sates of Delhi, Punjab, Odisha on a pilot project mode. So far, the cost of the vaccines (US 60-80 $) has been prohibitive for an average Indian. Coupled with Poor awareness even among educated and affordable population and the cultural hurdles of vaccinating young girls for a condition that manifests after 40 years is a communication challenge. The first hurdle in India of production of affordable indigenous HPV vaccine has been achieved (5 September 2022) recently opening a big opportunity. Governments (both federal and provincial) must make all-out efforts vaccinate all eligible females of the country; we owe it Indian women! In my opinion India must introduce pan-gender vaccination programs and start tracking all HPV-related (head and neck and anal) cancers and evaluate impact of HPV every decade for the next 50 years. A Mission mode is required to cover all the eligible in the next 2-5 years paid by the government (for at least below poverty line -BPL) families and provision of education through education system and social mobilization on a large scale are the key strategies to achieve this goal. This manuscript is a review the status of Cervical cancer, screening and diagnostic efforts, HPV vaccination status and recommends the way ahead to achieve national commitment for elimination of HPV related cervical and other cancers by 2030. Materials & Methods: GOI annual reports, HPV vaccination project efforts and outputs and Program implementation plans and Campaign approaches of vaccination under NHM, Indigenous vaccine producers’ statement and DCGs clearance.
Introduction
Govt. of India had launched a National Cancer Control Programme in 1975, revised its strategies in 1984-85 and again under National Health Policy 2017. While it stresses on primary prevention for Tobacco related cancers, addresses Secondary prevention of cancer of the uterine cervix, mouth, breast etc. and Tertiary prevention of therapeutic services including pain relief on a national scale through regional cancer centres and medical colleges [1].
In May 2018, the WHO Director-General announced a global call for action to eliminate cervical cancer, underscoring renewed political will to make elimination a reality and calling for all stakeholders to unite behind this common goal. The global strategy to eliminate cervical cancer recommended i) a vision of a world where cervical cancer is eliminated as a public health problem; with a threshold of 4 per 100 000 women-years. Global leaders and national government have committed to a) vaccinate 90% of girls fully vaccinated with HPV vaccine by age 15 years b) Screen 70% of women with a high-performance test by 35 years of age and again by 45 years of age c) Among the women diagnosed with cervical disease 90% receive treatment (90% of women with precancer treated, and 90% of women with invasive cancer managed). If these targets are achieved, median cervical cancer incidence rate will fall by 42% by 2045, and by 97% by 2120, averting more than 74 million new cases of cervical cancer; and the cervical cancer deaths averted will be 300 000 by 2030, over 14 million by 2070, and over 62 million by 2120 [2].
The human papillomavirus (HPV) is currently the most common pathogen responsible for female cancers, especially cervical cancers. It is also associated with many other diseases, including cutaneous and anogenital warts, and genital and upper aerodigestive tract cancers. Cervical cancers were estimated around 604 000 new cases and 342 000 deaths in 2020. About 90% of the new cases and deaths worldwide in 2020 occurred in low- and middle-income countries [3]. Some other types of HPV can lead to cervical cancer, head and neck cancer, or cancer of the anus or penis. India, accounted for 9.4% of all cancers about a fifth of the global burden of cervical cancer and 18.3% (123,907) of new cases in 2020 [4]. Although the age-standardized incidence rate of cervical cancer decreased substantially by 39.7% (95% UI 26·5–57.3) from 1990 to 2016, it is the second leading cause of cancer deaths for females in 12 Indian states [4]. The situation is alarming in the rural areas due to ignorance about the hazards of cervical cancer and scarce healthcare resources and efforts of the existing facilities and non-availability of vaccines and screening in facilities of sub-district level facilities [4, 5]. The Disability Adjusted Life Years (DALY) rate for cervical cancer in 2016 was highest in Karnataka, followed by Tamil Nadu, Chhattisgarh, Madhya Pradesh, and Maharashtra [6]. The estimated risk of cervical cancer is calculated to be approximately 1 in 53 Indian women during their lifetime as compared with 1 in 100 women in developed nations. In India, cervical cancer is the most common cancer accounting for 25.9% of new cancer cases and 23.3% of all cancer related deaths. Statistically, yearly approximately 90,000 new cases of cervical cancer are noted. Indian women face a 2.5% cumulative lifetime risk and 1.4% cumulative death risk from cervical cancer. At any given time, about 6.6% of women in the general population are estimated to harbour HPV infection. HPV serotypes 16 and 18 account for nearly 76.7% of cervical cancer in India. Poor prognosis due to late diagnosis is common, in India and in similar resource-constrained settings around the world, where women present with advanced stages of Human Papilloma Virus (HPV) caused cervical cancer.
The Hospital based Cancer Registry in India reported a total of 44300 (30% of GC & 3.3% of AC) cases of Cervical cancers in 2021 out of a total of 148338 Gynaecological Cancer cases and grand total of 1332207 all sites’ cancers [5].
Epidemiology
Agent
Human Papillomavirus (HPV) is the causative virus. There are over 100 different kinds of HPV, but some kinds of HPV can also cause cancer of the cervix, vagina, vulva, or anus and some of HPV cause problems like genital warts. There are about 14 high-risk HPV types including HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68. High-risk HPV strains include HPV 16 and 18, which cause about 70% of cervical cancers. Other high-risk human papillomaviruses include 31, 33, 45, 52, 58, and a few others. Low-risk HPV strains, such as HPV 6 and 11, cause about 90% of genital warts, which look like bumps and rarely develop into cancer [7].
Host
The Cervical cancer in India affects women between 15 and 44 years of age, with higher risk among women with multiple sexual partners or a partner exposed to multiple women. The threat starts with the beginning of active sexual life. In the only host that has been studied extensively humans especially women more than 100 HPV types have been described based on the isolation of complete genomes; a larger number is presumed to exist based on the detection of sub genomic amplicons.
An Indian study of 607 participants enrolled between January 2014 and June 2016, who were subjected to L1-PCR, sequencing, and E6/E7 nested multiplex type- specific PCR for HPV detection and genotyping. Cytological distribution of 440 cases included invasive cervical carcinoma or ICC (n = 210), inflammatory smear (n = 162), normal cytology (n = 68). The study reported an overall prevalence of HPV infection of (359/595) 60.33%. Prevalence of HPV infection was 93.80% (197/210) in invasive cervical cancer (ICC) cases, 54.32% (88/162) in inflammatory smear and 19.11% (13/68) in normal cervical cytology. The most prevalent genotype was HPV16 (87.28%) followed by HPV18 (24.56%) and HPV 51(3.46%). The overall prevalence of single type was 76.58% and highest (78.9%) among ICC cases. The most frequent genotype combination after HPV16 + 18(9.4%) was HPV16 + 66 + 68(2.7%) which was frequently observed in inflammatory cytology. Age > 45years, parity ≥3, low socio-economic condition, rural residential area, and post menopause state were significantly associated with HPV infection in a study in Odisha [8]. Multiple infections did not have a significant association with any of the clinicopathological variables (like stage, LN metastasis, cell type) except tumour size ≥ 2cm in ICC cases. The impact of 2v, 4v, and 9v vaccines in preventing cervical cancer in Odisha were 89.99, 91.65, and 92.16% respectively.
Another study that collected demographic, epidemiologic and clinical information of women of aged group 20–60 years with gynaecological abnormalities attending the gynaecology and cancer OPD at a tertiary care health centre reported that majority of the study participants were young married women and did not have any formal education (85.5%). Mean (SD) age at the time of first pregnancy among the study subjects was 16.8 (2.7) years. Majority of the study participants were below poverty line (88.2%). A total of 68.6% of the study subjects had an HPV infection. Among those that had an HPV infection, majority had HPV 16 infection (95.4%). In the remaining 4.6%, HPV 18 was present. Findings show that with increasing age, HPV prevalence increases. Also, early age at marriage, lack of education, increased parity, early age at first pregnancy, poor sanitation, use of tobacco and belonging to below poverty line were significant risk factors for HPV infection [6].
Transmission
HPV is mainly transmitted through sexual contact and most people are infected with HPV shortly after the onset of sexual activity. The human papillomavirus infects by entering our body through a cut, scrape, or tear in our skin. We get it from skin-to-skin contact, or vaginal, anal, or oral sex. A women can pass HPV to her baby if she has genital warts during pregnancy. In rare cases, this can cause a noncancerous growth in baby’s larynx (voice box). More than 90% of them clear the infection eventually Figure 1.
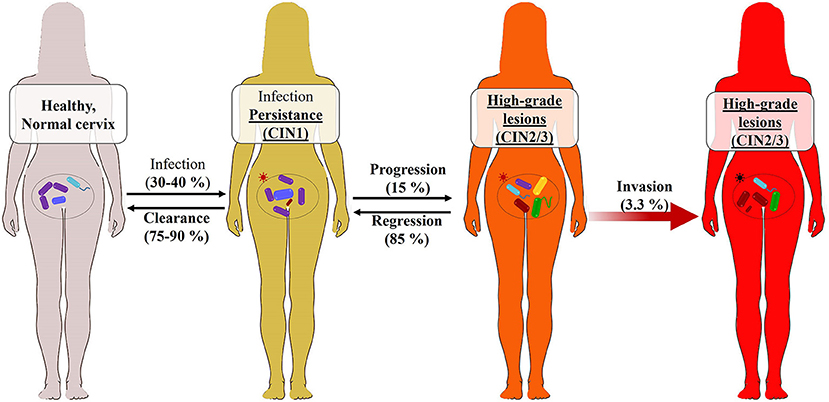
Source: https://loop.frontiersin.org/people/819629/ overview Figure 1: Risk Factors: Following factors increase the risk of HPV infections.
1. Damaged skin like - cut a lot or have holes are more likely to get common warts. 2. Direct contact touching someone’s warts or surfaces warts have touched. 3. Number of sexual partners The more sexual partners you have, or sex with someone who has many partners, increases risk. 4. Age Children are more likely to get common warts and Genital warts are more common in adolescents and young adults. 5. Weak immune system Conditions such as HIV or AIDS or are on treatment (cortisone therapy in Covid 19 infections) that weakens immune system. 6. Women living with HIV are 6 times more likely to develop cervical cancer compared to women without HIV.
- Symptoms of cervical cancer: The symptoms observed include i) Irregular menstruation with spotting or bleeding, ii) post-menopausal bleeding, iii) Spotting or bleeding after sex, iv) Spotting or bleeding after sex in post-menopausal women v) Persistent foul- smelling white discharge/discharge which is blood- stained, vi) Persistent back ache which cannot be cured by over-the-counter drugs and vii) Loss of control over urine and motion passing.
- The diagnosis: HPV is diagnosed by 1. Vinegar solution test: This test uses a vinegar (acetic acid) solution application on the lesions that will turn white. 2. Pap test: A swab is sued to collect samples from cervix or vagina. The samples are examined in a lab microscopically for abnormal cells, that lead to cancer. 3. DNA test: Every woman over 30, must be subjected to this test along with a Pap test. If the DNA of the cells of cervix have the HPV type that can lead to cancer, diagnosis is confirmed.
Prevention
Vaccination against HPV and screening and treatment of pre-cancer lesions are the cost-effective ways to prevent cervical cancer. Human papillomavirus (HPV) vaccines, introduced in many countries in the past decade, have shown promising results in decreasing HPV infection and related diseases, such as warts and precancerous lesions. Currently, more efforts must be put into increasing the vaccine’s coverage, especially in low- and middle-income countries. Provision of education on HPV and vaccination is one of the most important methods to achieve this.
In India, bivalent and quadrivalent HPV vaccines were licensed in 2008 and a non-valent vaccine was licensed in 2018. The Indian Academy of Paediatrics Committee on Immunization (IAPCOI) recommended that HPV vaccines be given as a two-dose regimen, six months apart for girls below the age of 14 years for those who can afford it [9]. Vaccination was advised to females as young as 9 years as well as in those aged 13–26 years who have not previously completed vaccination. Demonstration projects initiated in Andhra Pradesh and Gujarat in 2009 introduced HPV vaccination in public health services in India. Following a few deaths in these projects, although subsequently deemed unrelated to vaccination, HPV vaccination in research projects was suspended. Since 2016, the successful introduction of government-sponsored opportunistic HPV vaccination programmes in Delhi, Punjab, and Sikkim (with high coverage and safety), are in vogue [10].
The Current KAP Status of HPV Vaccine is Very Low as Seen from my Own Small Study
My interview of MPH scholars admitted to master’s in public health course in a provincial government run university since 2018, out of 100 scholars (68 girls and 32 boys),
- Most (90%) had heard of HPV vaccine & its potential to prevent Cervical cancer (CC)
- Only 13 candidates (11 girls and 2 boys) had heard of CC in their known circle
- 23 (19 girls 74 boys) knew that HPV vaccine is imported
- Nobody knew the cost of HPV vaccine
- None of 68 girls had taken or explored the possibility of the vaccine A study of the 17,729 vaccinated girls, 4348 (25%) received three doses on days 1, 60, 180 or later, 4979 (28%) received two doses on days 1 and 180 or later, 3452 (19%) received two doses on days 1 and 60, and 4950 (28%) received one dose, inferred that a single dose of quadrivalent HPV vaccine is immunogenic and provides lasting protection against HPV 16 and 18 infections similar to the three- and two-dose vaccine schedules, although the study suffered some limitations [11].
In another study by Niraja Bhatla Immunogenicity and vaccine targeted HPV infection outcomes were compared between 1795 girls aged 15-18 years receiving two (1-180 days) and 1515 girls of same age receiving three (1-60-180 days) doses. Immunogenicity outcomes in 15–18-year- old two-dose recipients were also compared with the 10–14-year-old three-dose (N = 2833) and two-dose (N = 3184) recipients. The 15–18-year-old two-dose recipients had non-inferior L1-binding antibody titres at seven months against vaccine-targeted HPV types compared to three- dose recipients at 15-18 years and three-dose recipients at 10-14 years of age. Neutralizing antibody titres at 18 months in 15–18-year-old two-dose recipients were non- inferior to same age three-dose recipients for all except HPV 18. The titres were inferior to those in the 10–14-year-old three-dose recipients for all targeted types. Frequency of incident infections from vaccine-targeted HPV types in the 15–18-year-old two-dose recipients was like the three dose recipients. None of the girls receiving two or three doses had persistent infection from vaccine-targeted types. These findings support that two doses of HPV vaccine can be extended to girls aged 15-18 years [12].
Based on 9672 girls in Punjab and 24446 girls in Sikkim it was observed that 28/9672 (0.3%) girls in Punjab and 118/24446 (0.5%) in Sikkim reported adverse reactions like Headache (50), dizziness (36), nausea (25), fainting (16), vomiting (5) and others (6) [12].
Till date three vaccines-Cervarix (GSK), Gardasil (Merck & Co0, and Gardasil-9 (Merck & Co) are available in India, and all are imported to protect against HPV. Though they’re available to boys and girls as young as 9 and adults up to age 26 India has allowed their use only for girls in public health programs. All three protect against HPV 16 and 18. Gardasil and Gardasil-9 are also effective against HPV 6 and 11, which cause most genital warts. Gardasil-9 also covers against the high-risk strains 31, 33, 45, 52, and 58.
As prophylactic, vaccines will be effective pre-exposure to virus, the target population for vaccination will be 9–10-year-old pre-pubertal girls, but this may raise cultural and social issues, that need to be addressed.
Current Status of Cervical Cancer Efforts in India
During the year 2021-22, a total of 4.66 million persons got screened through opportunistic screening in over 640 NCD clinics, and 5148 sub-district NCD clinics across the country. About 58,000 cancer cases were identified in the screening. The number of cancer cases increased from around 11385 in 2014-15, to 145430 in 2018-19 and then declined to 77293 (2019-20) and 58602 (2020-21), due to Covid 19 Pandemic. Based on the cancer registry data it is estimated that there will be about 800,000 new cancers cases in India every year [12]. At any given point there is likely to be 3 times this load that about 240,000 cases [13].
Based on a review of 2011-16 of the 28 population- based cancer registries (PBCR) the projected cancer burden in India for 2021 was 26.7 million, DALYs AMI and expected to increase to 29.8 million in 2025. The highest burden was in the north (2408 DALYsAMI per 100,000) and north-eastern (2177 DALYsAMI per 100,000) regions of the country and higher among males. Cancer Cervix contributed to 4.3% of the burden, seventh among the seven leading cancer sites among combined population and second among women- lung (10.6%), breast (10.5%), oesophagus (5.8%), mouth (5.7%), stomach (5.2%), and liver (4.6%) [14]. Real time availability of cancer incidence is lacking by 2–3 years and underreporting of deaths with inaccuracy in reporting of cancer specific deaths in the Civil Registration System has its effects on estimation of adjusted mortality Incidence ratio. PBCRs cover approximately 10% of total population, and their distribution and coverage are not uniform across all the states. Nearly 24 cancer sites added to more than 50% of total cancer DALYs at 35–59 years, the highest from cancer of cervix uteri and breast (63.5% each). The most common causes of cancer DALYs among females were breast (232.7 per 100,000), cervix uteri (98.6 per 100,000), ovary (78.9 per 100,000), lung (74.1 per 100,000) and gall bladder (58.3 per 100,000) cancers [14].
Cervical cancer screening program guidelines recommend Cervical cytology (Pap) smear is proposed for 3 free smears per lifetime each woman, the first time at age 55 or more. A woman with an inadequate smear should be re- screened. If the second smear is also inadequate, the patient must be referred to a known competent screening service.
Cervical cancer screening program guidelines recommend Cervical cytology (Pap) smear is proposed for 3 free smears per lifetime each woman, the first time at age 55 or more. A woman with an inadequate smear should be re- screened. If the second smear is also inadequate, the patient must be referred to a known competent screening service. 1. Women aged 30 years or older must be screened three times in succession, utilising cervical cytological (Pap) smears targeting three (3) smears per lifetime, with a 10-year interval between each smear, commencing at not earlier than age 30 years. 2. Follow up/Referral advise criteria includes i) a client with normal smear to be informed of 3. next smear date. ii) a client with Low-grade SIL and atypical squamous cells (ASCUS) goes for repeat smear in 12 months’ time and if the diagnosis remains the same or worsens, the patient is e referred to a colposcopy clinic. If negative on the second smear, the client will fall into the normal screening cycle. iii) Clients with High grade SIL and/or atypical endocervical (glandular) cells (AGUS) in the first screening are refer to a colposcopy clinic. If negative on colposcopy and cytology, the client can be discharged. If positive, treat. 4. Any patient with a macroscopically suspicious lesion, whatever the cytological result may be, must be referred for colposcopy [15].
HPV Vaccination Status
Two international pharmaceutical firms, Merck, and GlaxoSmithKline have developed vaccines against HPV that were introduced in the United States in 2009. Globally among adults aged 18−26, women receiving one or more doses of human papillomavirus (HPV) vaccine has increased from 22.1% in 2013 to 39.9% in 2018 [16]. The percentage of adults aged 18−26 who received the recommended number of doses of HPV vaccine increased from 13.8% in 2013 to 21.5% in 2018. Currently, the estimated global market share by volume is 23 % for bivalent, 52 % for tetravalent, and 25% for nonvalent HPV vaccines. From 2013 to 2019, UNICEF procured 30.9 million doses of bivalent and tetravalent HPV vaccines for both Gavi-supported countries and self-financing MICs. In 2019, UNICEF procured twelve million doses, which represents a market share of approximately 27% of the global volume. The project demand was about 50 million doses that fell short by two thirds due to Covid 19 pandemic. India did not request for HPV vaccine through GAVI support so far as there was not national program, whereas Bhutan (since 2010), Sri Lanka (2017) and Bangladesh (2022) in south Asia have been importing and using [17]. Following the outbreak of COVID-19, vaccine shipments and other critical deliveries have been heavily impacted due to the dramatic decline in available flights and actual use in all countries due to competing priority.
Indian Situation
One can buy the HPV vaccine at some high street pharmacies, travel clinics and high-end hospitals. Most clinics only offer the HPV vaccine up to and including age 45. Indian HPV Vaccine Market Analysis Report 2021 reports a slae of 3.5 billion doses in 2019 going up to 4 billion in 2020, 45. Billion in 2021 and 5 billion in 2022.
The same year (2009) India launched a two-year ‘demonstration’ project on the vaccines-run by the ICMR, the state governments of Andhra Pradesh and Gujarat, and US- based non-governmental organisation PATH International — involving about 32,000 girls aged ten to 14 years old. The trials came under the spotlight after the alleged deaths of four girls in March 2010 as well as some of the vaccinated girls developing adverse reactions like headache, stomach disorders and early onset of menstruation. Currently exceptionally few people have taken in the private sector.
In India HPV vaccine wastage made more news than it’s uses. HPV vaccination was first started in Delhi in November 2016, the Shahdara branch of Delhi State Cancer Institute, which is the only government institution providing the vaccine for free to adolescent girls in the age group of 11- 15 years. Around 8,000 vials of the human papillomavirus vaccine (HPV) were wasted in the last year due to no takers as per a report in February 2022 [18]. Initially the demand was poor, due to hesitance and lack of awareness, an approach through schools helped mobilizing children had helped vaccinating about 4000 children. About half of them are coming for booster doses.
Cold Response to Expert Opinion
Karnataka’s only govt cancer hospital backs giving cervical cancer vaccine to students: Kidwai Memorial Institute of Oncology Cancer Research and Training Centre, the only government cancer hospital in Karnataka, sees nearly 1500 cases of cervical cancer each year, most of whom come in the late stages. The director of the institute recommended the government take up immunisation of 30 lakh odd female adolescent girls between the ages of 9 and 15 years against cervical cancer in early 2021. Each one of them was advised to be given two doses with a gap of six months [13]. The program is yet to take off. The process of introduction of a new vaccine and it’s successful implementation to reach desired level of coverage is depicted in the Figure 2.
Policy Development for Human Papillomavirus Vaccine Introduction in Low-Resource Settings
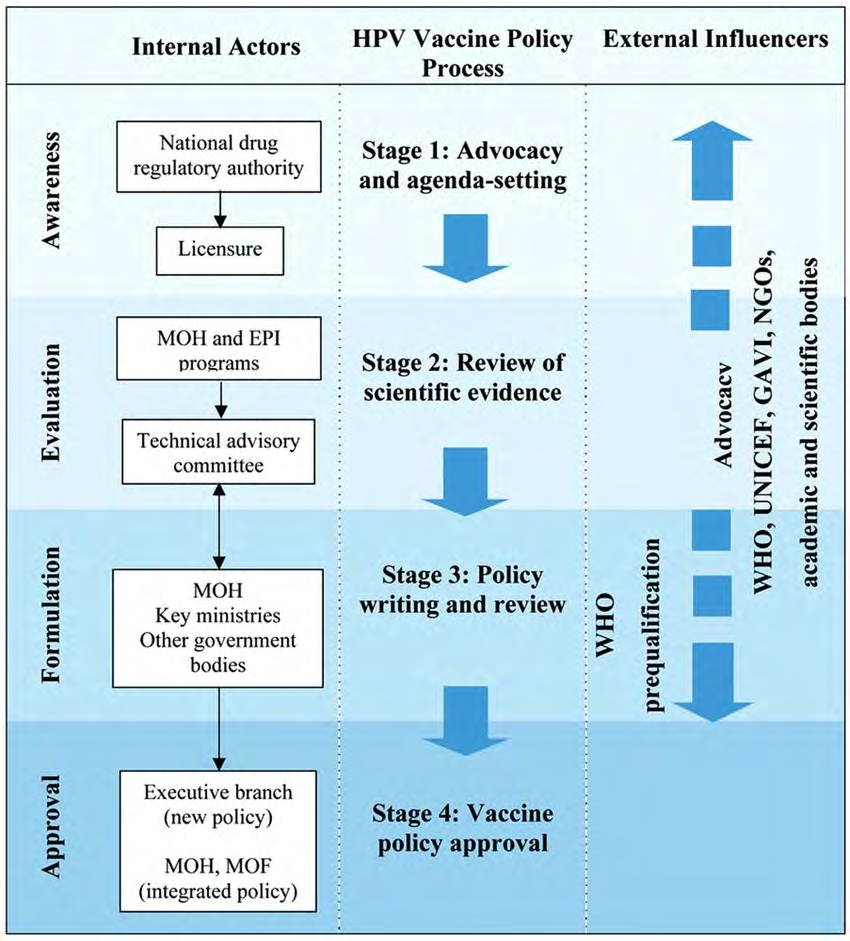
Source: fig1_228375198, https://www.researchgate.net/figure. Figure 2: Illustration of HPV Vaccine Policy Processes in India.
Indigenous HPV Vaccination Production- A Milestone Achieved
India’s first indigenously developed quadrivalent Human Papilloma Virus (HPV) vaccine for the prevention of cervical cancer was launched in early September 2022, around Ganesh Chaturthi, a deity of hurdle removals. The Drugs Controller General of India (DCGI) had granted market authorisation to Serum Institute of India (SII) in August 2022 to manufacture an indigenously developed vaccine against cervical cancer. The qHPV vaccine CERVAVAC has demonstrated robust antibody response, nearly 1,000 times higher than the baseline against all targeted HPV types and in all dose and age groups. The Cervavac works against HPV Type 16 &19 that cause cervical cancers and type 6 & 11 that cause genital warts in India. Cervavac is likely to be priced between INR 200-400, in consultation with Government of India.
The manufacturer reports that this vaccine can give 100 percent protection if given to those who have not been sexually active, between the ages of 11 years and 26 (or even as late as 30) years. For those between 11 and 15 years, two doses must be given and for those between 15 and 26 years, three doses must be given, although the protection may not be as significant. As the HPV infection takes between 5 and 25 years, to turn into cancer, it can be tracked and caught early through pap smear screening and then treated. It is expected that the SII’s Cervavac - a quadrivalent human papillomavirus (qHPV) vaccine - will cost less than options available from foreign drug makers, making it more affordable for Indian households. The product is expected to hit the shelves by November, this year. Currently available vaccines cost between 2000-3500 per dose and to obtain a complete regimen of HPV vaccines in India, one must spend at least Rs 5,000 to Rs 8,000. A qHPV vaccine is available from Merck Sharp and Dohme (Gardasil), and a bivalent HPV vaccine is available from GSK (Cervarix). The cost for one vial of Gardasil is Rs 3,927 and for one vial of Cervarix, the cost is Rs 2,640. It is necessary to administer the injection in two or three doses spaced several months apart.
According to the Chairperson of the National Technical Advisory Group on Immunisation (NTAGI) Indigenous vaccine launching is an exciting experience. NTAGI hopes that this much-awaited vaccine will be included in the National Immunisation programme for 9-14-year-old girls, soon.
India’s experience of expanding routine immunization since 1985, Pules polio vaccination for eradication of Polio and the most recent efforts and delivery of Covid 19 vaccine to over 2140 million doses, in the process fully vaccinating nearly 950 million people covering 68.5% of eligible people gives a great hope of the potential of Indian health system to quickly cover the eligible girls of 9-14 years over a period of next 2 years, only if the Government of India commits for it.
Issues Need Clarifying
Target Population and Number of Doses: India with a population growth rate of 1% annually is slowly approaching to become most populous country in the world. Going by estimated projection from world bank, the population of India is projected at 1393.4 million (1,393,409,038) as of July 1, 2021 and likely to be 1421.3 million in mid-2023, the fiscal year when one can expect HPV vaccination to begin, given the fact that vaccine is expected hit the shelf by November December 2022 [19]. In 2021 25.78% of the population was in 0- 14 years, 67.45% between 15-65 and 6.78% over 65 years [20, 21]. As per UNICEF report.
While NTAGI suggests girls of 9-14 years, the manufacturer recommends 2 cohorts of both boys and girls i) 11-15 years- 2 doses at an interval 6 months ii) 15-26/30 years 3 doses (Table 1).
| Female | Male | Total | |
|---|---|---|---|
| NTAGI (9-14) | 5.1%= 72.5 million | 5.5%= 78.2 million | 150.7 million |
| Manufacturers Guide (11-14) | 3.44%= 48.9 million | 3.76%= 53.44 million | 102.34 million |
| ----do------- (15-30) | 12.5%= 177.7 million | 14%= 199 million | 376.7 million |
Table 1: Total projected Population- 1421.3 million. The target population and Vaccine requirements.
Our efforts of Covid 19, has proved the potential of the country has evidenced that we can cover all eligible population (approx. 1335 million) as recommended by the manufacturer. However, given the cost involved (INR 400,434 million), the government is unlikely to take up the challenge. The modest approach of covering only the girls of 9-14 years as suggested by NTAGI would mean procuring 145 million doses of the HPV vaccine costing about 43,500 million Indian Rupees. In my opinion there should not be any hesitation in doing so. In the subsequent years we can plan to take up immunization of new entrant in the age group of (about 1.7% of total population) and unmarried (not expose to sexual life already) may be covered in a phased manner. This would mean most of the rural girls get excluded and women in 15- 30 years in cities and towns amounting to roughly 1/3 of the total female population (approx. 200 million) in that age may have to be covered Figure 3.
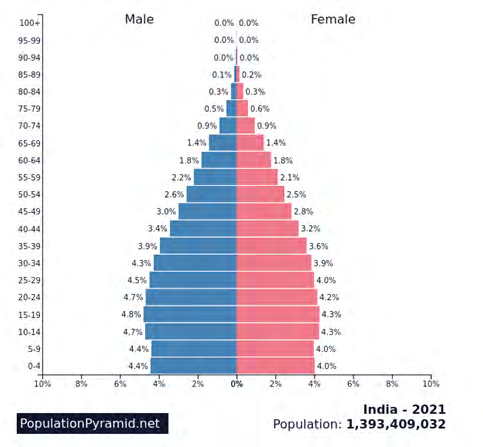
If pan-gender coverage is accepted the cost will double. Figure 3: Population Pyramid 2021.
To be realistic the Government must bear the cost of vaccination only for girls of BPL families, which reduce the overall cost to just one third of the calculated cost.
FBased on the age groups and immunization schedule India adopts vaccine doses required would be:
| Vaccination Strategy adopted | Target population | No of doses | Vaccine doses required | Cost @ INR 300/dose |
|---|---|---|---|---|
| NTAGI- only girls | 72.5 million | 2 | 145 million | 43500 million |
| NTAGI- Pan-gender | 150.7 million | 2 | 301.4 million | 90440 million |
| Manufacturers guide- 11-14- girls only | 48.9 million | 2 | 97.8 million | 29340 million |
| Manufacturers guide- 11-14- pan-gender | 102.34 million | 2 | 204.68 million | 61,404 million |
| Manufacturers guide- 15-30 women | 177.7 million | 3 | 533.1 million | 159,930 million |
| Manufacturers guide- 15-30 pan gender | 376.7 million | 3 | 1130.1 million | 339,030 million |
Note: The cost of one dose of vaccine is assumed as INR 300 (syringes cost INR 250 + other contingency-INR 50).
Summary
• Opportunities 1. The national Government is committed to achieve Cervical Cancer elimination by 2030
2. Indigenous vaccine will be available by November 2022 reducing the cost and minimizing the hostels of importation 3. NTAGI has accepted in principle and advised Govt. to include in the national immunization schedule
4. Covid 19 vaccination has empowered the health system to plan and execute to go beyond childhood immunization 5. Most of the eligible aged children are accessible through schools • Challenges Based on authors experience of over 45 years in immunization, the biggest challenge will be of Vaccine hesitancy. Despite the acuteness and case fatality of Covid 19 the full vaccinated coverage is hovering around 70%. Even among health workers, exposed to infection the fully vaccinated coverage has not gone beyond 80% in most of the states. 1. Initially the vaccination may have to be done under the guidance of a qualified medical office in each PHC or UHC area and be ready for taking care of any adverse reactions. 2. Accessing out of schoolgirls may throw a bit of challenge, but not unsurmountable
References
-
National cancer control programme.
-
(2020) Global strategy to accelerate the elimination of cervical cancer as a public health problem, WHO.
-
Sung H (2021) GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71: 209-249.
-
WHO (2022) Cervical cancer.
-
(2021) Clinicopathological profile of cancers in India, ICMR. A report of HBCR 2021, ICMR, MOH & FW.
-
Mehrotra R, Yadav K (2022) Cervical Cancer: Formulation and Implementation of Govt of India Guidelines for Screening and Management, Indian Journal of Gynaecologic Oncology 20(1): 4.
-
Kapoor CS (2020) Contact Prevalence of HPV infection in reproductive aged female in Delhi NCR region. 8(2): 612-615.
-
Johnson TC (2022) HPV.
-
Senapati R (2017) HPV Genotypes distribution in Indian women with and without cervical carcinoma: Implication for HPV vaccination program in Odisha, Eastern India. BMC Infect Dis 17: 30.
-
Sankaranarayanan R (2019) Current Status of human papillomavirus vaccination in India’s cervical cancer prevention efforts. Lancet Oncol 20(11): e637-e644.
-
Sankaranarayanan R (2018) Can a single dose of human papillomavirus (HPV) vaccine prevent cervical cancer? Early findings from an Indian study. Vaccines 36(32 Pt A): 4783-4791.
-
Bhatla N (2018) Are are two doses of human papillomavirus vaccine sufficient for girls aged 15- 18 years? Results from a cohort study in India. Papillomavirus Res pp: 163-171.
-
Annual Report (2022) Ministry of Health and Family Welfare.
-
Kulothungan V (2022) Burden of cancers in India - estimates of cancer crude incidence, YLLs, YLDs and DALYs for 2021 and 2025 based on National Cancer Registry Program. BMC Cancer 527.
-
John Kombe A (2021) Epidemiology and Burden of Human Papillomavirus and Related Diseases, Molecular Pathogenesis, and Vaccine Evaluation. Front public health 8: 552028.
-
(2021) Karnataka’s only govt cancer hospital backs giving cervical cancer vaccine to students. Indian Express Bengaluru.
-
(2020) Human Papillomavirus Vaccine Supply and Demand Update, UNICEF Supply Division.
-
(2022) 2-year expiry- 8,000 cervical cancer vaccines wasted in Delhi, Somrita Ghosh / TNN.
-
(2011) Population of India.
-
(2022) India: Age distribution from 2011 to 2021.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda