Measurement of Medication Adherence to Intranasal Corticosteroid in Allergic Rhinitis
Objectives: To assess the impact on patient adherence to intranasal corticosteroid spray by using medication adherence chart and development of potential strategies to reduce non-compliance. Methodology: This prospective cohort study was carried out on 102 outpatients in a tertiary care hospital, Kerala state for one year in the age group of 12 and above, these patients were categorised as case and control where case group were provided with administration chart and counselling. On the review date, we monitored the administration chart and reviewed the patient quality of life and all participants were asked to fill the questionnaire regarding the factors that may have influenced their adherence to treatment. Each factor that may have affected adherence to the prescribed medication is evaluated according to the MARS score and all variables were assessed. Results: Among 102 patients, the reasons for nonadherence were measured, among that forgetfulness, due to cost of spray, fear of persistent use of medication for lifelong were most predominant factor. According to MARS score, there were statistically significant association exist between medication adherence before and after intervention (p <0.001). Conclusion: Patient’s usage and adherence with intranasal corticosteroids are sparse in the treatment of allergic rhinitis. Therefore, based on our results, patients must be given proper education and to help patients overcome these barriers by interventional aids which can promote the proper use of intranasal corticosteroids and prevent remission.
Introduction
Allergic rhinitis (AR) is a common condition. AR is a chronic inflammatory disease that affects the upper respiratory tract and have the symptoms including sneezing, itching, nasal congestion and rhinorrhea. There two types of rhinitis which include seasonal which is caused by airborne pollens or perennial caused by indoor allergens such as mites, house dust, fungal spores [1]. Intranasal steroids are first line therapy for patients with more severe symptoms [2]. Intranasal corticosteroids relieve sneezing, rhinorrhea, pruritis, and nasal congestion with minimal side effects. They reduce inflammation by blocking mediator release, suppressing neutrophil chemotaxis, causing mild vasoconstriction, and inhibiting mast cell mediated, late phase reactions. These agents are excellent choice for perennial rhinitis and can be useful in seasonal rhinitis especially if begun before the advancement of symptoms. Adherence to treatment is essential for optimizing health outcomes in nearly any disease.
Haynes ST, et al. defined adherence as “the extent to which a person’s behaviour coincides with medical or health advise” [3]. Nonadherence is associated with worsening of disease and increased morbidity. Rate of adherence is usually reported as the percentage of the prescribed doses of the medication actually taken by the patient over a specified period. Adherence rates are typically higher among patients with acute conditions, as compared against those with chronic conditions. According to the World health organization (WHO) nonadherence to the medical regimen consists a major clinical problem in the management of patient with chronic illness. Medication adherence to the prescribed medication is a neglected issue in the treatment of allergic rhinitis, leading to poor treatment outcomes. Physicians just focus on the treatment plan to the patient but the issue related to the compliance is never known. This nonadherence may lead to the remission of the condition and need to review for the same condition without any improvement of the symptoms. The decision to take medication is under the patient’s control, and application of interventions to this aspect have shown greater results. Therefore, physicians should become familiar with the concept of adherence in clinical practice and the factors affecting it, which remain underestimated and poorly studied. The present study focuses not only on identifying nonadherent patients in an outpatient setting, but also on gathering patient-related factors, especially personality traits, since human behaviour must be taken into account when evaluating adherence. Although current practice guidelines recognize that INCSs are the most effective agents available for the treatment of allergic rhinitis, a large online survey found that only 30% of patients in the USA with severe nasal congestion were actually receiving INCS therapy [4]. The main aim of the corticosteroids therapy is to maximize efficacy, minimize potential systemic side effects and to improve patient adherence. Factors that will help to improve the adherence to intranasal corticosteroids are dosing regimens, patient preference and cost effectiveness. The role of counselling in the outpatient basis is a crucial step. Many studies have shown that the interventions made has shown positive outcomes in the particular department in terms of pharmaceutical delivery system.
Individualization of the treatment for AR, providing counselling to the caregiver or the patient are essential for providing best patient care. The reason for nonadherence can be addressed through the counselling like false expectation, safety of the medication, cost etc. can improve adherence. Patient misunderstanding with the risks and benefits of therapy and proper use of INS are major barrier to the effective treatment of allergic rhinitis. It is important that clinicians educate patients on the benefits of medication. It helps people take their medication appropriately would be a better achievement to avoid remission, antibiotic resistance and preventable resistance. The aim of this paper is to assess the impact on patient adherence to intranasal corticosteroid spray by using medication adherence chart. Strategies to improve the patient adherence to control noncompliance and measure medication adherence.
Methodology
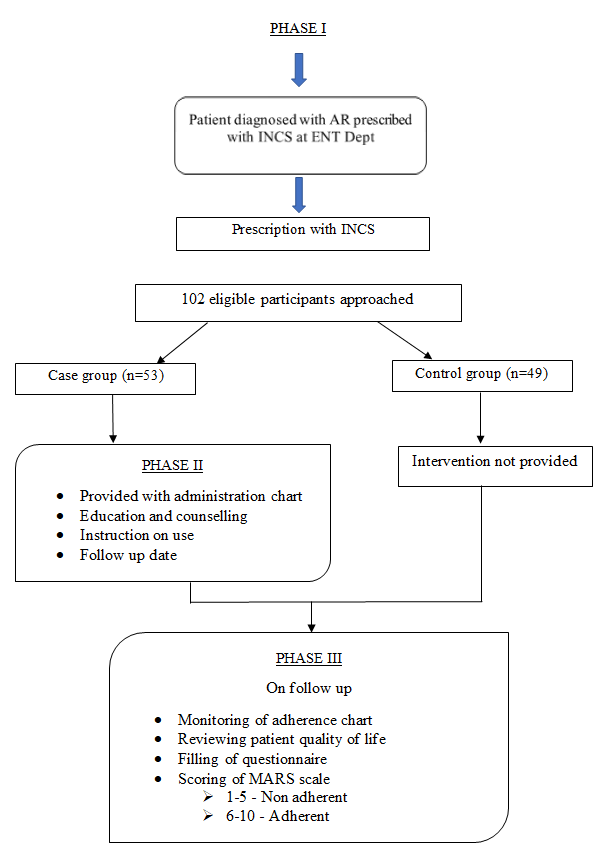
A prospective cohort study was conducted on the outpatient in the ENT department where we enrolled 102 patients (men and woman) who were prescribed with intranasal corticosteroids spray for the allergic rhinitis. The study was carried out in three phases. After the approval from the ethical board as per letter no. KAS/IEC/PharmD 2019-08 and formal consent for assessing the patient’s medical records and outpatient prescription from the ENT department, patients were selected based on inclusion and exclusion criteria. Relevant clinical data like demography, age, sex MRD number and history of the patient were included in the data collection form. Total of 102 patients were collected from September 1st 2020 to March 2021 from the department of ENT, after the detailed clinical history and examination of the patients, diagnosed with moderate to severe allergic rhinitis were enrolled in the study. The selected patients were divided into 2 groups (case and control) by simple randomization method. In the second phase the case group patients were provided with pharmacological care mainly through direct patient counselling along with a drug administration chart and instructions on the use of fluticasone furoate spray at a dose of 27.5µg per day, administered two sprays per nostril twice daily for 1 months from the date of consultation. The case group patients were counselled on the medications and the use of the medication, importance of the patient compliance to the therapy for effective outcome. The follow up date was provided and their data was recorded in the data collection form. The control group were deprived of any pharmaceutical care till the end of the study and they were provided with usual treatment guidelines by the physician. But they were followed up for further data collection and measurement of medication adherence using MARS Scale. In the post intervention phase, all the cases and control group patients were followed up after 1 month and both the groups were reassessed their medication adherence using the MARS Questionnaire which is a 10-item questionnaire regarding the factors which may influence their adherence to the treatment by calculating the scores and monitoring the administration chart and reviewing patient’s quality of life.
Descriptive and inferential statistical analyses were carried out in the present study. Results on categorical measurement were presented in number (%). Level of significance was fixed at p=0.05 and any value less than or equal to 0.05 was considered to be statistically significant. Chi square analysis was used to find the significance of study parameters on Outline of the Study categorical scale. The Statistical software IBM SPSS statistics 20.0 (IBM Corporation, Armonk, NY, USA) was used for the analyses of the data and Microsoft word and Excel were used to generate graphs, tables etc. The factors which affect the adherence to the treatment were then evaluated and all the variables were analyzed statistically.
Results
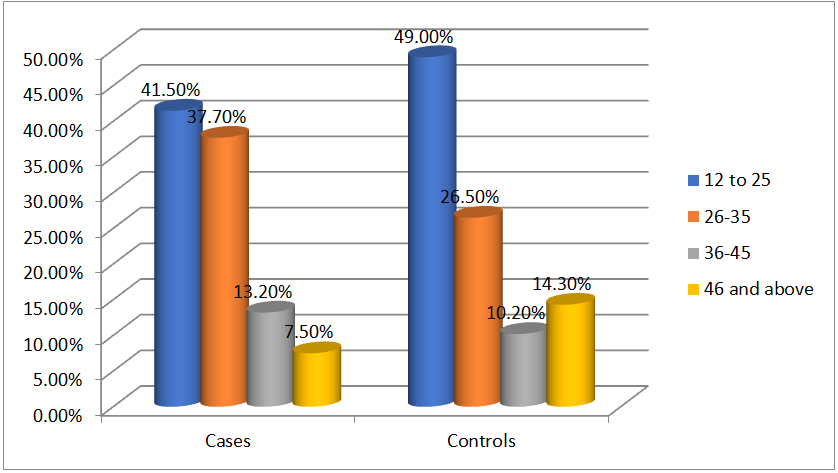
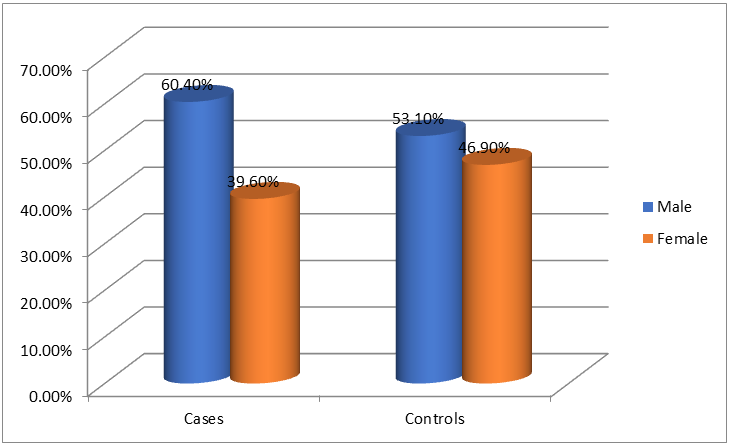
In this study of 102 patients on intranasal corticosteroids selected from the outpatient department of ENT, 53 subjects were allotted to cases and 49 to the control group. Table 1 features the sociodemographic characteristics of the selected patients. Adults aged between 26-35 (41.5%) were mostly prescribed with INCS compared to other age groups. While for the controls, age group 12-25 (49%) were higher followed by 26-35(26.5%) and 46 and above (14.3%). Male patients were predominant among the cases (60.4%) as well as among the controls (53.1%). Employed participants constituted 47.2% of the cases and only 24.5 % of the controls. Patients with known family history for allergic rhinitis was significantly less in both the groups (p<0.05).
| Characteristics | Case n (%) | Control n (%) |
|---|---|---|
| Age | ||
| Dec-25 | 20 (37.7) | 24 (49) |
| 26-35 | 22 (41.5) | 13 (26.5) |
| 36-45 | 6 (11.3) | 5 (10.2) |
| 46 and above | 5 (9.4) | 7 (14.3) |
| Gender | ||
| Male | 32 (60.4) | 26 (53.1) |
| Female | 21 (39.6) | 23 (46.9) |
| Work status | ||
| Employed | 25 (47.2) | 12 (24.5) |
| Unemployed | 28 (52.8) | 37 (75.5) |
| Family history | ||
| Known family history | 24 (45.3) | 18 (36.7) |
| No known family history | 29 (54.7) | 31 (63.3) |
Table 1: Participant socio-demographics (N=102).
| Results N=49 (%) | |
|---|---|
| Forgetfulness | n=45 (91.83) |
| Decision to omit | n=17 (34.7) |
| Emotional factors | n=13 (26.5) |
| Due to cost of spray | n=30 (61.2) |
| Fear of persist of medication for lifelong | n=20 (40.8) |
Table 2: Participant socio-demographics (N=102).
The reasons for nonadherence were measured among the controls (n=49), of which forgetfulness (95.91%), cost of spray (61.2%), fear of persistence of medication for lifelong (40.8%) were the most predominant factors (Table 2).
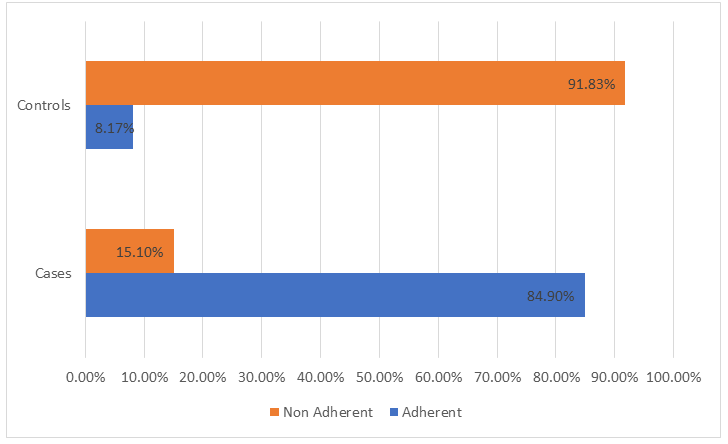
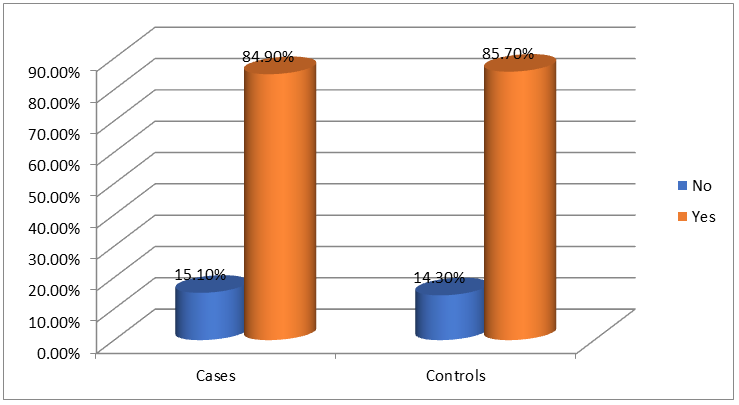
The age shows a correlation between the adherence level before and after the intervention. Higher adherence was shown by the patients aged between 12-25 (41.5%) followed by 26- 35 (37.7%) while cases above 36 years was less adherent. Hence it is evident that as age advances the level of adherence decreases even with the intervention (Figure 1). Among cases and controls, higher adherence was shown by males than females (Figure 2). Amidst these 102 patients, 45(84.90%) showed positive outcome to the intervention provided and lead to the adherence to medication consumption in the case group. Based on the compliance with the intervention, there is statistically improvement in the medication adherence before and after the intervention (p <0.001) (Figure 3). Assessment of the interventions delivered has resulted in the promoting the medication adherence to 84.90% which shows a statistically significant improvement after the pharmaceutical care. Follow up evaluation was also carried out for all the participants to assess the response behavior of individuals to therapy, of which 7(15.10%) among the cases were uncontactable and considered to be failed from the service provided (Figure 4).
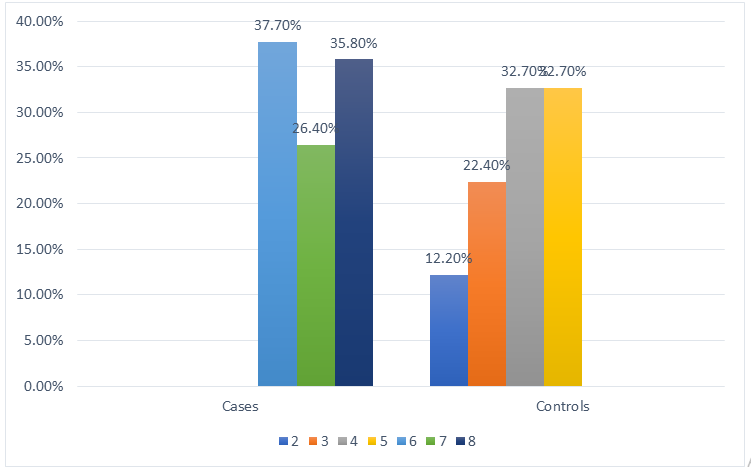
According to the MARS score, with intervention, 53 patients in case group showed 20(37.7%) higher adherence score of 6 than the following 19(35.8%) score of 8, and 14(26.4%) score of 7. Among the non-adherent group of 49 patients, the lowest adherence score of 2 were shown by 6(12.2%) of patients followed by 11(22.4%) by the score of 3 and 16(32.7%) of score of 4 and 5 (Figure 5).
Discussion
The importance of adherence to medical therapy is an incontestable element that may affect the treatment outcome. It is undoubtful that non-adherence will cause prolonged treatment duration, dissatisfaction of patient, low quality of life and unnecessary financial burden. This study assesses the importance of the patient counselling in increasing the adherence to the use of intranasal corticosteroids which has given an 84.9% outcome. 102 patients were enrolled in the prospective cohort study, where 56.9% were males and 43.1% were females, the predominance of the male gender may be due to majority of patients were males who visited the ENT department during the study period.
Our study used the initiative of MARS score for the evaluation pertaining to beget adherence. Accordingly, 53 patients were adherent to the effect of intranasal corticosteroids used in the treatment of allergic rhinitis, MARS score as 6 (37.70%), 7(26.40%), 8(35.80%) respectively which is concordant with the I Kalkan K, et al. [5]. The difference in adherence rate could be due to medical care and drugs, better care services and patient awareness about medication adherence [6]. One of the major reasons for such variable rates of nonadherence reported in different studies is that there is no standard, universally accepted definition of adherence due to which patients may report adherence according to their own personal definitions rather than conventional medical concepts of non-adherence [7, 8].
The adherence level of case group, which include age group 26-35 (41.5%) were higher when compared to other age groups followed by 12-25 (37.7%). The minority was seen under the age group 36-45(11.3%) and 46 and above (9.4%). For control group, age group 12-25 (49%) were higher than the other age group followed by 26-35(26.5%) and 46 and above (14.3%). The results portrayed that 49% of people in the adolescent age group of 12-25 years possess low adherence. It is undoubtful that patient counselling has improved the adherence in the treatment of allergic rhinitis in adolescent group. The result was similar to that of Hammersley V, et al. 2014 [9]. Comparatively middle-aged patients (26-35yrs) shows more adherence than adolescent and geriatric patients.
The study aims to shed light upon the adherence of patients on the basis of employed or unemployed, the result reveals that most of the unemployed, provided with patient counselling has greater adherence to the treatment of allergic rhinitis. The employment effect has influenced medication adherence due to the busy work schedules, which often force patients to omit doses. Hence inconvenience is experienced outside the premises of their residency. Patients employed (47.2%) has low adherence as compared to unemployed (52.8%) patients. This study supports this statement as inconvenience of taking medicine outside home was the second most reported reason of intentional nonadherence. The result is also similar to another study conducted by Mathew A, et al. [10] which has shown that busy lifestyle is an important barrier to medication adherence to patient population.
It also goes through the familial history of the patients enrolled in the study, the result shows that the adherence does not have much relevance in the treatment of allergic rhinitis. Those patients provided with counselling and medication chart have high adherence value compared to those control group. There are hardly a few studies which are conducted on this area.
This study also focused on associating the medication prescribed along with intranasal corticosteroids. Steroids (78%) and oral antihistamines (75%) are prescribed outcome along with intranasal corticosteroids to increase the treatment outcome. It improves the patient’s quality of life and wellbeing, which result adherence to the treatment of allergic rhinitis. The crucial part of the study focuses to enhance an intervention which was known through effective response from patient counselling, medication charts, and also by conducting activities where patients were educated and taught to use intranasal spray.
The case group has been provided with all intervention which has an 84.9% adherence to the treatment. Inadequate knowledge of administration of intranasal spray results in non-adherence, which can be resolved through patient counselling, medication chart and the key diagram showing the way to use the intranasal spray. This result was concordant to the result of Rollema C, et al. [11].
The respective study has come across the various reason for non-adherence, the result of control group reveals forgetfulness (95.91%), decision to omit dose (34.7%), emotional factors (26%), due to cost of spray (61.2%), fear of persist of medication for lifelong (40.8%) is the major factors for the non-adherence. This result is similar to various studies carried out and supporting study by Ocak E et al. [12]. Forgetfulness and cost of the nasal spray are the two major reason for non-adherence, patient get relief from the symptoms within few days of administration of medication, which tend them to skip the unintentionally. Discontinuation of the INCS dose without completely administering the course of INCS cause the remission of allergic rhinitis. While some skip the dose due to the fear of persist of medication for life long (40.8%).
The study includes the reviewing of the patient progress within a time period of 1 month. In Case group, all patient included in the case group brought back the medication chart from which we obtain the time of administration of doses and the missed dose. No such interventions are familiar in another studies, which help to increase the adherence up to 84.90%.
Our study calculates the adherence and non-adherence using the MARS scale, which scale from 1 to 10. The current study is the second to test whether MARS score is correlated with the outcome of AR treatment. The patient interview which results in low MARS score 1 to 5 is non-adherent and those scores 6 to 10 is adherent to treatment. In case group scores between 6 to 10, the resulted score for 6,7 and 8 include 37.7%, 26.4%, 35.8% respectively. In control group, the MARS score is between 1 to 5, 12.2% (score 2), 22.4%, 32.7% (score 5), 32.7% (score 5). This result is concordant with Baccioglu KA, et al. [5]. The MARS questionnaire includes 10 questions which is answered by each patient resulting in the MARS scoring in accordance to the answers for the questionnaire. Skipping of dose due to forgetfulness is the major reason for non-adherence. This study also indicates that usage of this self-report questionnaire can help the health care practitioners to identify the suboptimal adherence in AR patients, especially those who could benefit from counselling [5].
An adherence intervention is one in which a change in behavior is sought to increase adherence with medical or health provider advice [13]. We were able to implement this intervention such as administration chart which is cost effective, easily implemented and education on INCS may improve the adherence rate in some patients hereafter.
This study has some limitations such as the sample size, the possibility of interactions between the factors and the follow up period. To increase our knowledge in this area and in order to validate our results, multi-centered studies with large samples must be done to understand the dimensions of adherence and requires different interventions. Self- reporting was the only method employed in this study which is subjective in nature and may have under estimated the status of non-adherence. In our study, asking patients directly but nonjudgmentally about their adherence while on counselling and follow up time and we detect those who admit to relapse in their treatment.
As there are several studies regarding the adherence to the intranasal corticosteroids in allergic rhinitis, such studies focus on the reasons for the adherence by direct methods and indirect methods on a specific population. There is a knowledge gap exist in the Indian population that could be bridged by better patient education. This study explains that such interventions generate direct benefit for the patient and this could improve adherence rate.
Conclusion
The term adherence has an active role with a prescriber, and non-adherence encompasses the diverse reasons for patients not following a treatment recommendation. It can be both intentional and unintentional which leads to either underuse or overuse of prescription medications. The study found that usage and adherence with intranasal corticosteroids in the management of allergic rhinitis have shown low adherence rate at the ENT department of tertiary care hospital, which has led to disease progression and poor health outcome.
This study demonstrated that providing pharmaceutical care by counselling and adherence chart to the patients diagnosed with allergic rhinitis has demonstrated greater sustainability of adherence rate than with the patients without the pharmaceutical care. The study encompasses that male gender, age, employment status, and patient related factors as predictors of medication adherence to the intranasal corticosteroids spray. From our study we can conclude that major reasons for non-adherence is mostly forgetfulness, high cost of spray and a fear of persistence of medication for lifelong respectively.
The administration chart that we developed has a positive impact on adherence rate, the hospital should encourage the use of this practice in every department so that it would improve the quality of life for patients with chronic conditions. The current study also measured the medication adherence using validated MARS scores to evaluate the outcome of AR treatment before and after intervention. Therefore, based on our results, clinical pharmacist can help patients with proper education to overcome these barriers to adherence and we demonstrated that by interventional aids, we can promote the proper use of intranasal corticosteroids, self-care and prevent remission.
Acknowledgement
The authors acknowledge KIMS Al Shifa hospital, Perinthalmanna, doctors, nurses, for their help in delivering the intervention and the facilities, and the patients for volunteering to take part in the trial.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Meltzer EO (2016) Allergic Rhinitis: Burden of Illness, Quality of Life, Comorbidities, and Control. Immunol Allergy Clin North Am 36(2): 235-248.
-
Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, et al. (2008) Allergic Rhinitis and its impact on asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA (2)LEN and AllerGen). Allergy 63(S86): 8-160.
-
Horwitz RI, Horwitz SM (1993) Adherence to treatment and health outcomes. Arch Intern Med 153(16): 1863- 1868.
-
Shedden A (2005) Impact of nasal congestion on quality of life and work productivity in allergic rhinitis: findings from a large online survey. Treat Respir Med 4(6): 439- 446.
-
Koca Kalkan, Baccioglu KA, Kalpaklioglu AF (2013) Allergic Rhinitis: Can we identify nonadherence to therapy and its predictors easily in daily practice?. J Investig Allergol Clin Immunol 23(5): 315-322.
-
Yiannakopoulou ECH, Papadopulos JS, Cokkinos DV, Mountokalakis TD (2005) Adherence to antihypertensive treatment: A critical factor for blood pressure control. Eur J Cardiovas Prev Rehabil 12: 243-249.
-
Lemay J, Waheedi M, Sharqawi AS, Bayoud T (2018) Medication adherence in chronic illness: do beliefs about medications play a role? Patient Preference and Adherence 12: 1687-1698.
-
Zhang Y, Li X, Mao L, Zhang M, Li K, et al. (2018) Factors affecting medication adherence in community-managed patients with hypertension based on the principal component analysis: evidence from Xinjiang, China. Patient Preference and Adherence 12: 803-812.
-
Hammersley VS, Elton RA, Walker S, Christian HH, Sheikh A (2014) Adolescent seasonal allergic rhinitis and the impact of healthcare professional training: cluster randomised controlled trail of a complex intervention in primary care. NPJ Primary Care Respiratory Medicine 24: 14012.
-
Mathew AC, Aneesa MV, Rahman A, Suresh D, Suriyaprakash TNK, et al. (2020) Assessment of medication adherence patterns and various causes of non-adherence in long term therapies in a tertiary care hospital, Research J Pharm and Tech 13(5): 2420-2426.
-
Rollema C, Roon VEM, Schilder AGM, Tjalling WV (2019) Evaluation of instructions in patient information leaflets for the use of intranasal corticosteroid sprays: an observational study. BMJ Open 9(1): e026710.
-
Ocak E, Acar B, Kocaoz D (2017) Medical adherence to intranasal corticosteroids in adult patients. Braz J Otorhinolaryngol 83(5): 558-562.
-
McDonald HP, Garg AX, Haynes RB (2002) Interventions to enhance patient adherence to medication prescriptions: scientific review. JAMA 288(22): 2868-2879.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda