A Prototype for Covid Risk Assessment: Designing a Chatbot for Users to Determine Personalized Risk of Severe Outcome
This paper overviews the creation of a COVID Risk Assessment (CRA) Chatbot prototype designed to support recommendations for individuals based on the assessment of their COVID-related risk profile. Among rapidly emerging digital technologies, AI-enabled chatbots have the potential to offer real-time interaction with users via immediate responses, notifications, and reminders; interestingly, these intelligent agents can also be designed to offer personalized advice based on specific user characteristics and may even be scaled to interface with many users concurrently. Drawing from prior research, we designed a CRA-chatbot prototype to incorporate a variety of parameters affecting the severity of COVID-19 systems. These factors include the number of vaccine doses, the date of last vaccination, previous COVID-19 infection history, age, and risk factors such as disease history. Broadly, the prototype is envisioned to take the users’ input with their personalized risk assessment of severe symptoms to further educate them; in so doing, suggestions for treatments, additional serological testing, and supplementary vaccine doses can then be made. We conclude that, within the current learning health system environments, AI-enabled chatbots are digital health tools well-suited for empowering personalized COVID-19 education and related knowledge dissemination.
Introduction
In a post-COVID pandemic world, many of us are still reeling from the ongoing impacts of the COVID-19 pandemic which began in March 2020. While measures implementing lockdowns and mask requirements have lapsed in many places, case numbers remain at a relatively high level, indicating an ongoing need to monitor population immunogenicity and risk factors for severe disease [1, 2]. In Canada, only about 50% of the population has received three doses of a COVID-19 vaccine, with even less (13%) receiving a fourth [3]. While 82% of the population has completed the basic two-dose primary series, emerging variants of concern and waning immunogenicity from vaccination and early pandemic infection indicate that continued outreach is necessitated to maintain booster administration rates and overall awareness of one’s risk status. Messaging regarding vaccine administration timelines and recommendations has been difficult to interpret for many Canadians, warranting the implementation of new information delivery methods more suited to individual usability.
Online platforms have been touted to be convenient for widespread and schedule-sensitive user access, within both private and public spaces [4]. Recent evidence has demonstrated the effectiveness of such digital tools in addressing healthcare concerns. One of the more widely studied applications of digital tools in healthcare delivery has been in digital therapeutics, which uses digital information gathering or intervention tools to assist in the diagnosis and management of mental health conditions such as bipolar disorder or schizophrenia [5]. Digital intervention strategies have also been proposed to promote healthy behavior in a more general sense, particularly in the domains of nutrition, exercise, and drug and alcohol use [5, 6]. Mobile health (mHealth) apps have also been advocated to assist in behavior change regarding childhood vaccination, although outcomes have been somewhat mixed [7].
Overall, current models of digital health intervention technologies appear promising, although ensuring effective and meaningful engagement with such tools requires a clear identification of goals and ongoing feedback and development [6]. Specifically, frameworks proposed to help shape digital therapeutics tool development have indicated the need for a clear outline of the tool’s aim and scope, a more informed view of meaningful user engagement with respect to tool utilization, and supportive implementation of new policies and strategies to strengthen user engagement with the continuing, and possibly expanded, use of the advocated digital tool over time [8].
An example of a Digital Health tool suitable for education and knowledge dissemination is the use of chatbots. AI chatbots are intelligent agents used for conducting online exchanges via text or text-to-speech, in lieu of providing direct contact with a live human agent. Released in 1966, ELIZA was the first chatbot used in healthcare, mimicking the anticipated replies of a psychotherapist via pattern- matching and response selection [9]. However, ELIZA had limited knowledge and communication abilities. Today, AI-enabled chatbots offer diagnosis of symptoms, mental healthcare consultation, nutritional facts, and tracking. For example, in 2020, WhatsApp teamed up with the World Health Organization (WHO) to make a chatbot service that answers users’ questions about Covid-19 [10]. Among the most value-adding features of using chatbots in healthcare, especially with sensitive and mental health issues, include instantaneous access to critical information, awareness and tracking of the users’ behavior, anxiety, and weight changes to encourage the development of better habits, personalization, and anonymity [11, 12]. AI-enabled chatbots offer personalization which remains completely dependent on the specific application use case. Chatbots can gauge patient behavior by utilizing tools such as facial recognition. Chatbots offer real-time interaction via immediate responses, notifications, and reminders. Chatbots can additionally be scaled to interact with numerous users at the same time.
The paper is structured as follows. First, the scientific literature that provides the theoretical underpinning used to develop the foundation of rules for the CRA-chatbot risk stratification such as immunogenicity, vaccine efficacy, and waning immunity is reviewed with a brief look at health and wellness chatbots. Next, we explore the framework for designing the CRA-chatbot prototype, specifically, how various key parameters for risk assessment we have identified may be integrated as part of the prototype features. Finally, we highlight the benefits and limitations of our approach prior to drawing concluding remarks on the future potential development and growth of such AI-enabled chatbot systems.
Background
In this section, we highlight the accumulated evidence on how our immune system responds to a COVID-19 infection and identify the important considerations for determining disease severity and immunity. We then close the section with a brief look at health and wellness chatbots.
The Immune System
As humans, we live in a world compromised by various pathogenic and non-pathogenic microbes and a collection of allergenic or toxic substances that may affect homeostasis. In defending against such influences biologically, we have evolved a complex series of organs, tissues, and cells that comprise what is known as the immune system [13]. Environmental microbes that may cause harm contain a variety of pathogenic mechanisms to infiltrate and persist in the human body. As such, the immune system has a variety of defensive mechanisms that address various avenues of opportunity for microbes to adversely affect health. A key feature of the immune system is the recognition of the self, versus non-self, based on the identification of cellular markers which usually consist of distinctive surface proteins or toxic substances [13, 14]. This form of identification and discrimination is fundamental in eliminating threats while preventing damage to healthy body tissues. Recognition falls into two general categories, instinctive responses dependent on the host’s genetic code that respond to pathogens in the host’s body (innate immune system), and immune responses that are dynamic and rearrange antigen-binding molecules with targeted specificity towards foreign material introduced to the body (adaptive immune response). The innate immune system is the first responder to impending threats and reacts very quickly [14]. It is followed by the adaptive system which requires the proliferation of its limited supply of highly specific cells to mount a tangible response. The adaptive immune system can produce cells that persist for an extremely long duration within the host’s body in a latent state that can later be re-activated rapidly when encountering the specific antigen again [13, 14]. This can be referred to as immune system memory and allows for a more efficient response to repeated infection and infiltration by pathogens, thus reducing complications in the future.
The Role of Antibodies
Antibodies are a critical piece of the immune system that mediate antigen-specific immunity in response to a range of different pathogens. B-cells (B-type lymphocytes) are the key component responsible for the proliferation of antibodies [15]. B-cells start development in the bone marrow, mature in the spleen, and are later stored in lymph nodes. These cells can produce pathogen-killing antibody proteins or host antibodies as transmembrane protein receptors on their cell surface [13, 16]. Antibodies can neutralize pathogens in a variety of ways, they can directly neutralize a toxin by attaching to their surface, they can mark pathogens to illicit other immune responses from cells such as macrophages, and they can activate proteins that assist immune response in secondary ways (proteins that cluster together pathogens or that signal downstream immune responses). More specifically referred to as immunoglobulins, they are produced within B-cells of the immune system [15]. They contain a constant region of DNA that is maintained across the various subtypes (isotypes) of immunoglobulins. Two identical heavy chains and two identical light chains vary depending on the subclass of antibody, each possessing a different function (IgA, IgG, IgD, IgE, IgM). Antibodies also possess variable regions which is the reason why the immune response can be so diverse as the unique process of cutting, splicing, and changing these regions allows for countless combinations of these regions [16]. The variation in these changing areas allows antibodies to attach to a variety of pathogens.
Immunological Memory & the Role of Vaccines
Another important role B-cells serve is in the function of immunological memory. What this means is that secondary infection of a previously encountered microbe leads to a more efficient immune response to said pathogen [17]. This is the result of leftover B-cells still in circulation with antibody receptors for the repeated antigen and B-cells that are still capable of producing those antigens being left behind. It makes the immune response more efficient in that it doesn’t have to produce immature B-cells in the hopes of producing the correct antibody, and it has an active leftover reserve of functioning cells. Vaccines fundamentally exploit the adaptive immune system and its ability to retain immune memory [17]. Exposing one’s body to lower concentrations of microbes, heat-killed microbes, and inactive microbes presents an opportunity to build up B-cells with the proper antibody combinations. This allows for a subsequent improved reaction if contact is made with the intact microbe. Preparing a host’s body for a subsequent infection may prevent life-threatening damage, chronic health problems, or may reduce infection symptoms.
COVID-19 Vaccine-Conferred Immunogenicity
Recent evidence has demonstrated that the efficacy of COVID-19 vaccines does begin to wane after a certain point [18]. An analysis of the literature indicates a decline beginning anywhere from 3-6 months post-vaccination. A study examining healthcare providers conducted in Belgium indicated a significant decline in antibodies at the 3-month mark for those who had been both seronegative (not displaying any antibodies for COVID-19) and seropositive before an initial mRNA vaccination series [19]. This study also indicated a peak of antibody response between 2 and 6 weeks for seropositive participants, and 4 and 6 weeks for those seronegative, which has been supported by other estimates [20]. Despite the decline at the 3-month mark, all participants still had a strong antibody response. Another study examining healthcare workers provided evidence of a rapid decrease in antibody titers between the third and sixth month following vaccination, with relatively high vaccine efficacy still present at the 6-month mark [21].
A recently conducted meta-analysis indicated that in general, antibody titers from vaccination show a marked decrease after the 6-month post-vaccination period [2], with the rate and amount of decline varying based on a few different parameters. This has been backed up by multiple publications, with a relatively consistent, gradual decrease in both IgG-specific and neutralizing antibody levels being reported across the first 6 months post-vaccination [22, 23, 24, 25]. These results were consistent for those receiving either an mRNA-based vaccine (BNT162b2 aka the BioNTech, Pfizer vaccine) or an adenoviral vector-based vaccine (ChAdOx1 nCoV-19 aka the Oxford, AstraZeneca vaccine).
There has been increasing support for the utilization of booster doses no further than 6 months after the primary series [20]. Booster doses have been shown to decrease rates of infection and severe illness as compared to the normal two-dose regimen [26]. A study examining COVID-19 trends during the Omicron variant surge indicated that those boosted with the BioNTech, Pfizer vaccine, or Moderna vaccine demonstrated increased protection, even though it was still noted to wane over time [27].
Current research collectively indicates that vaccination protects against severe disease [28], additionally indicating that this protection does not decay along with the decline in protection against COVID-19 infection. Initial boosters have been indicated to contribute to prolonged protection against severe disease in COVID-19 for as far as 3 months post-boost [29].
Impact of COVID-19 Infection-Conferred Immunity
Evidence has demonstrated that protection from COVID-19 lasts longer for those who have been both vaccinated and previously infected with COVID-19, as compared to those who have only been vaccinated (respectively, approximately 2 years vs 1 year). This data provides support for the chatbot recommendation delaying boosters for those who have recently been infected with COVID-19.
This observation has further been supported by additional evidence from a study conducted in the UK which indicated that antibody titers were much stronger at the year mark among those who had been previously infected with COVID-19 compared to those who had only received the two-dose vaccine series [23]. The Hall et al. study also indicated only a moderate decrease in IgG and neutralizing antibody levels at 8-10 months post-infection. In a study of elderly people, those previously infected showed as strong an immune response after one dose of the BioNTech, Pfizer vaccine as the uninfected control group showed after two doses [30]. This has been demonstrated on a general population level as well, with evidence that previous COVID-19 infections complemented and boosted overall immune response after vaccination [31, 32]. The impact of the previous infection was modulated by the variant of infection, however, with infection from the initial or Beta waves of the pandemic being less protective against the Delta wave [31]. This highlights the individuality of immune response, as well as the implications for strain-specific booster efficacy down the line.
Notwithstanding, it should be noted that infection- conferred immunity, in those vaccinated and unvaccinated, still displays a pattern of waning over time, albeit typically slower than for vaccination alone [32]. Overall, these data suggest that infection does provide increased protection, providing support for prolonged intervals between vaccination for those previously infected.
Antibody Testing Parameters
Antibody testing, to be used alongside typical PCR testing, can assist in the diagnosis of COVID-19 [33]. Serological testing can indicate whether the person carries antibodies to COVID-19. Serological testing can also be done on a more generalized basis to indicate those more susceptible to COVID-19 (presenting with fewer or no antibodies) and prioritize vaccination distribution [34]. It can be used to make other observations about population health, such as monitoring vaccine efficacy, infection trends, long-term immunogenicity, and specific data about antibody activity over time [35].
COVID-19 Serological Testing
There are 3 types of serology (blood) tests that can provide you with valuable information about protection levels. T-cell tests, quantitative antibody tests, and qualitative antibody tests. T-cells are a type of white blood cell that can be elicited to destroy infected cells and stimulate antibody production in B-cells [35]. After a COVID-19 infection, a small number of T-cells with receptors previously equipped for an antigen remain in the blood like the immunological memory displayed by B-cells. Even so, T-cell tests are very expensive to perform which provides limited application in wide-scale public health operations.
Quantitative and qualitative antibody testing measures the presence of antibodies developed in response to a COVID-19 infection or vaccination. The quantitative test shows the number of COVID-19 antibodies in one’s system; it is, however, difficult to establish the amount present which offers one protection from a range of severity of infections. Typically, with COVID-19 infections, quantitative tests look primarily for IgM and IgG subtype types if they distinguish between the two. Reports of antibody quantity use titers as the form of measurement [35]. The qualitative test illustrates the presence or absence of COVID-19 antibodies in one’s system. It is a simple yes, or no, and does not differentiate between infection-induced antibodies or antibodies created by the vaccine. This binary distinction is why the qualitative measurement of COVID-19 antibodies, as provided by the antibody test kit, is used as a primary parameter of the CRA- Chatbot.
Disease History & Immunocompromisation
Immune deficiencies may be classified into rare primary types and common secondary types. Primary types are caused by genetic anomalies that are unique and apparent at birth. Examples include DiGeorge syndrome, Fanconi’s anemia, and Selective IgA Deficiency. Secondary types are caused by external factors such as chronic infections (HIV, COPD, CHF) or immunosuppressive medication [13]. In 2021, many countries issued worldwide recommendations for increased COVID-19 vaccine protection for individuals with immunocompromised conditions which included subpopulations like the elderly aged 70 years and up [36].
Immunocompromised individuals are generally defined as those with diagnosed conditions in which their immune system is suppressed. This includes conditions such as chronic disease states, active cancers, primary and secondary immunodeficiencies, advanced HIV infections, and the use of immunosuppressive medications like steroids [16]. The immunocompromised are more susceptible to vaccine-preventable infections and present with more severe symptoms and outcomes. As a result, B-cell number/function can be affected and result in recurrent bacterial infections, or T-cell number/function may be affected leading to recurrent fungal and viral infections.
Health & Wellness Chatbots
In recent years chatbot use for health-related purposes has increased considerably, from supporting clinicians with clinical interviews and diagnosis to aiding consumers in self-managing chronic conditions. Briefly, AI chatbots for supporting health and wellness services include providing medical information, scheduling medical appointments, collecting patient data, handling insurance inquiries, providing mental health assistance, and requesting prescription refills. During the novel Coronavirus pandemic, institutions such as the Center for Disease Control (CDC) and the WHO have begun utilizing chatbots to share information, suggest behavior, and offer emotional support; the CDC names their chatbot “Clara”. Chatbots have varied widely in their responses to questions about physical health, suicide, intimate partner violence, substance abuse, and other sensitive conversations. While promising, the use of AI chatbots may also pose safety risks.
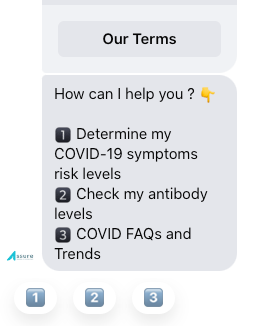
The CRA-chatbot prototype discussed in the rest of this paper (Figure 1) was developed to help individuals conduct a personalized risk assessment based on their unique health factors. COVID-19 can affect anyone, and the disease can cause symptoms ranging from mild to very severe. Certain individuals are more likely to have severe illness outcomes due to their unique characteristics or medical conditions which increase their risk. These are commonly known as “risk factors’’ which are the foundation of the CRA-chatbot risk assessment parameters. Essentially, the prototype is envisioned as a conversation agent to provide users with valuable information regarding the risk for severe symptoms, access to antiviral medications, and how to use rapid antibody testing to assess one’s immune status. This prototype utilizes key data points including vaccine doses and dates, COVID-19 infection status, antibody test kit, disease history, and age to determine the user’s risk levels for severe outcomes. The key benefit of using such a prototype is to educate an individual about their COVID-19 Symptoms Risk Index (CSRI); indeed, knowing the risk of developing the spectrum of COVID-19 symptoms based on personalized input can help individuals make more informed and timely decisions, ultimately saving lives.
Framework for Designing a Risk Index Model
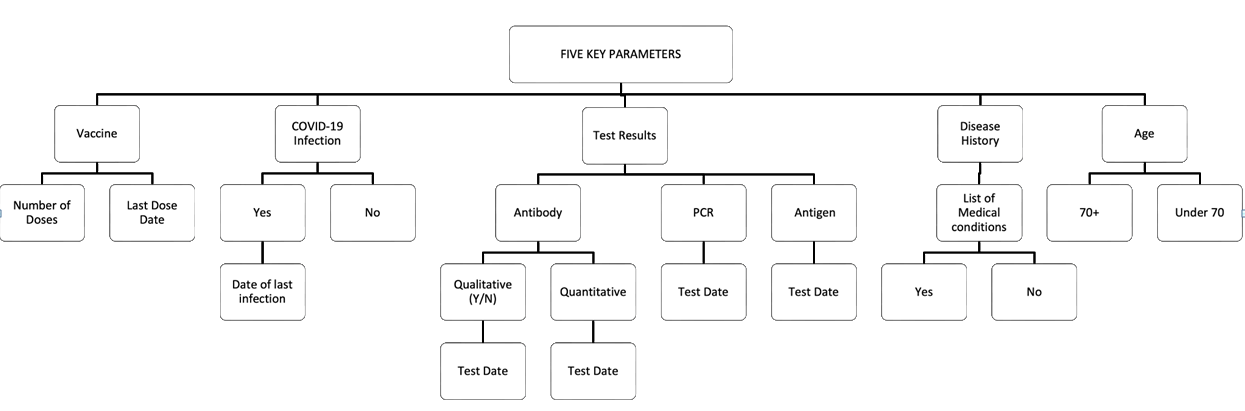
Research has unveiled multiple risk factors leading to COVID-19 (C-19). The C-19 Symptom Risk Index (CSRI) model uses five key elements to calculate risk stratification. These include vaccine doses and dates, prior C-19 infection, positive testing using antigen, PCR, NAAT, or antibody presence detection, age, and underlying medical conditions. Based on the available scientific evidence, an individual may be categorized into three distinct risk classes illustrated in Table 1.
Each risk class has associated severities of groups of symptoms and outcomes that an infected individual can expect to experience. The low-risk class tends to be asymptomatic or has mild symptoms that include sneezing, runny nose, sore throat, and headaches. The moderate-risk class involves flu-like symptoms like fever, chills, joint pain, hoarse voice, and altered or loss of senses like smell and taste. The high-risk class comprises severe symptoms such as a persistent cough, joint and muscle pain, chills, fever, dizziness, gastrointestinal symptoms (nausea, diarrhea, abdominal pain), and respiratory symptoms (pneumonia and ARDS) that could require hospitalization. In using this CSRI class system, anyone can easily understand their expected symptoms and the risk of severe symptoms, how and when to access antiviral medications, when to get a booster vaccine, and the status of their immune system against C-19. With knowledge of how one’s body is reacting to C-19, one is empowered to prevent severe outcomes by taking the necessary steps to ensure a symptom-free lifestyle.
| C19 Immune Status Index | High | Moderate | Low | |
|---|---|---|---|---|
| Outcome | Hospitalization | Severe symptoms | Flu-like symptoms | Asymptomatic or mild symptoms |
| Examples of Symptoms | Fever | Pneumonia | Chills | Runny nose |
| Chills | Persistent cough | Fever | Sneezing | |
| Dizziness | Acute Respiratory Distress Syndrome (ARDS) | Joint pain | Sore throat | |
| Joint pain | Muti-organ failure | Hoarse voice | Headache | |
| Muscle pain | Gastrointestinal symptoms (nausea, diarrhea, abdominal pain) | New loss of or altered sense of smell | ||
| Septic shock | ||||
| Death |
Table 1: Classes of C-19 Symptom Risk Factors.
Implementing the Risk Index Model into a CRA- Chatbot
The C-19 pandemic puts in stark relief the potential for chatbots to help save lives. Chatbots have unique affordances, which may mitigate short and long-term disease burdens during infectious disease pandemics. As chatbots provide a single answer to most questions, these digital tools can present concise information from credible sources, which may be less overwhelming than social media, or web search engines’ long list of results. This matters as fake news spreads online both faster and further than accurate news. Chatbots are uniquely suited for symptom screening in a pandemic because people with stigmatized conditions often avoid seeking health care and in-person education. This simply means that people may be more forthcoming with chatbots than with other humans, providing more unbiased, timelier, and more accurate personal triage and population- level infection rate estimates.
Pandemics differ from other national disasters in three ways. First, individual actions can significantly worsen outcomes in a pandemic, given that a single person may infect many others depending on behavior. Second, the fear of infecting others, especially loved ones or healthcare workers, makes infectious diseases more insidious through disease- related stigma. Additionally, medical and public health experts must inform what chatbots say, and how they say it. Translating medical information into advice for the public requires expertise and evaluation to prevent unintended consequences. Without proper design, deployment, and ongoing monitoring, chatbots may confuse rather than help us.
Although healthcare chatbots are conceivably very useful, research reveals that they are not meeting users’ expectations, particularly when it comes to trust, handling complex conditions, and usability. Based on the results of a recent study [37], consumers do not entirely trust chatbots. They were weary of relying on unfamiliar brands and had concerns about inaccurate diagnoses. Others said they would prefer to conduct follow-up research before they would trust the diagnosis and information provided. Additionally, some participants complained of spelling errors and links to content that seemed untrustworthy. Another takeaway is that chatbots have room for improvement when it comes to complex conditions. Overall, the report notes that although healthcare chatbots hold promise there is still a long way to go before they win over consumers. Taking the aforenoted factors into consideration for our design, we discovered the complexity of trying to implement all the rules identified in the research. The initial design was too complicated and a normalization exercise was conducted to reduce the complexity of having a cumbersome interface for the users. The rules were simplified to the following lower-level factors as illustrated by Figure 2.
Chatbot Integration of Vaccination History
The CRA-Chatbot uses C-19 vaccine efficacy models which state that vaccine efficacy declines between 6 months to a year. The chatbot uses a 6-month cutoff to indicate waning vaccine efficacy and a 12-month cutoff to indicate absent vaccine efficacy. It combines the number of vaccine doses and the time of the last vaccine to determine the users’ current vaccine efficacy state. This is an important chatbot parameter that is factored into the CSRI response of Low, Moderate, or High. The higher the number of vaccine doses and the shorter the duration of time from the last vaccination, the lesser the chance of severe symptoms.
The user is prompted to select the number of vaccine doses acquired. This numerical input is translated as a set of cut-off parameters for the CSRI class responses. If the user’s vaccine dosage number is 1 or less, then the chatbot will generate a CSRI response of Moderate or High. A vaccine dosage number of two or greater results in fewer symptoms, so the chatbot places the user in a CSRI of Moderate. The user is then asked to input the date of their last vaccine dose which the chatbot uses to place them either above or below the absolute 12-month time frame cut-off where antibodies are near undetectable [36]. If the user’s response lies below the 12-month cut-off, then the chatbot will generate a CSRI response of Low to Moderate. If the user’s response lies above the 12-month cut-off, then the chatbot will generate a CSRI response of Moderate to High. Without adequate protection against C-19 from the time of the last vaccination, the user has a higher risk of experiencing more severe symptoms.
Chatbot Integration of C-19 Infection Status
The CRA-Chatbot uses the user’s C-19 infection status and the date of the last C-19 infection to estimate their current antibody levels. The user is asked if they have had a PCR or antigen-confirmed C-19 infection. If the response is a yes then the user is prompted to input the date of the last C-19 infection. If the yes response and date fall within 6 months of the current date, then the chatbot will generate a lower CSRI class response. A yes response is confirmed by the presence of circulating antibodies which produce a positive antibody response from a testing kit. A yes response with a date falling beyond 6 months of the current date or a no response will generate a higher CSRI class response.
Chatbot Integration of Antibody Test Kit
The CRA-Chatbot uses the results of a qualitative C-19 antibody test to determine the presence or absence of C-19 antibodies in the user’s immune system. The user will select a yes or no response when prompted by the chatbot. A yes response indicates active immunity against C-19 antibodies and confirms active vaccine efficacy or antibodies from a previous C-19 infection. A no response indicates waning immunity with a need for a booster shot. These data, when combined with the vaccination history data, validate the given response with the real-time status of circulating C-19 antibodies. It provides easy-to-understand evidence to users of their current immune status which fosters trust in the chatbot results. If the user does not have a qualitative C-19 antibody test kit, a recommendation for an antibody test kit is made available.
Chatbot Integration of Disease History
The user’s disease history is an integral part of the parameters built into this chatbot. By selecting common conditions that contribute to an immunocompromised state, the CRA-Chatbot makes it easy to determine the user’s general immune status. The common pre-existing medical conditions the chatbot considers are any diagnosed immunocompromised state like obesity or HIV infection, Diabetes (Type 1 and 2), chronic diseases (Chronic Liver Disease, COPD, Renal failure), cardiovascular diseases (Congestive Heart Failure, Atrial Fibrillation), Dementia, and Malignant cancers [36]. The diagnosis of any of the mentioned medical conditions indicates a weakened immune system which produces low quantities of antibody levels.
The user is prompted to select a yes or no response to a list of the above-mentioned medical conditions by the chatbot. A yes response places the user in the High-risk class of the CSRI as a reflection of their immunocompromised state. A no response lowers the user’s chances of receiving a High-risk class response from the chatbot.
Chatbot Integration of Age
The user is prompted to select their age from a range of age distributions. The CRA-Chatbot incorporates this concept of immunocompromisation to any user above the age of 70. This particular demographic has immune systems that wane over time [36], slowing their response to C-19. This raises their risk of developing severe outcomes and prompts the chatbot to produce a response of Moderate-risk and above.
Discussion
The CRA-Chatbot begins with the most important user input; their age; to group them into their demographic niche (above the age of 70 and below the age of 70). Any user with an age response greater than 70 years, is classified as a High-risk class individual. Thus, anyone over the age of 70 is considered immunocompromised, as immunity wanes over time, so their response to a C-19 infection is delayed allowing for more severe outcomes. Following this logic, the next important parameter addressed by the chatbot is the presence of pre-existing medical conditions. If the user’s response is a yes, then they are classified as a High-risk class individual due to their immunocompromised state regardless of their age. The chatbot proceeds to collect information about the number of vaccine doses and their dates, antibody test results, and the presence and date or absence of a prior C-19 infection to generate a Low to Moderate risk class result. This response range is mainly determined by the user’s vaccination history and the chatbot uses every combination of possibilities and timelines to determine the appropriate response based on the data presented. By simplifying the potential responses by using binary inputs and time ranges, the chatbot can eliminate potential response errors because every potential combination of the four parameters has been programmed and run proofread. Fewer than 60 unique responses have been generated using our chatbot and each response has been proofed against the set parameters and validated with the appropriate CSRI class responses.
The CSRI Utilization for Behavior Change
The CSRI uses vaccine doses and dates, prior C-19 infection, antibody presence detection, age, and underlying medical conditions to place the individual’s immune system against C-19 into three distinct risk classes. Each risk class has associated severities of groups of symptoms and outcomes that the individual can expect to experience. The Low-risk class is defined as asymptomatic or with mild symptoms that include sneezing, runny nose, sore throat, and headaches. The Moderate-risk class involves flu-like symptoms like fever, chills, joint pain, hoarse voice, and altered or loss of senses like smell and taste. The High-risk class comprises severe symptoms like a persistent cough, joint and muscle pain, chills, fever, dizziness, gastrointestinal symptoms (nausea, diarrhea, abdominal pain), and respiratory symptoms (pneumonia and ARDS) that could require hospitalization. In using this CSRI class system, anyone can easily understand their expected symptoms and the risk of severe symptoms, how and when to access antiviral medications, when to get a booster vaccine, and the status of their immune system against C-19. With knowledge of how one’s body is reacting to C-19, the opportunity exists to change behavior and prevent severe outcomes by taking the necessary steps to ensure a symptom-free lifestyle. With the knowledge provided by the tool, individuals have the opportunity to modify their behavior in the following ways: prequalify for antiviral treatments, postpone their vaccine dose, seek a vaccine dose, perform more frequent testing, increase safety measures (masking, social distancing) or feel relieved, and do nothing.
Treatment Options
All individuals should receive targeted interventions such as treatments including chronic disease management, precautions to reduce exposure, vaccine doses, and effective pharmaceutical therapy. Increasing C-19 vaccination coverage is a public health priority. There are now treatments for C-19, both USA FDA and Health Canada approved the antiviral pill for use against C-19 in January 2022, but with a large supply of these pills available, experts say there is a lack of awareness among the public about who qualifies and how to access them. The key problem that exists is that when you are infected, you only have a 5-day window from symptom onset to begin treatment, and you need a prescription for which you must provide evidence of a positive C-19 test (antigen or PCR). Early diagnosis is key, but many people think they have a common cold and by the time they find out otherwise, it may be too late for treatment. Therefore, it is important for people who are at higher risk to be prepared. The C-19 Risk Assessment tool will guide individuals to be prepared by knowing their risk of severe symptoms so they can seek treatment within the 5-day window [37, 38, 39].
Future Research & Limitations
The new research initiative, Digital Health, Disrupter Analysis, County Readiness, and Technology Forecasts 2018- 2023, found that the adoption of chatbots will ramp up in the future due to citizens becoming more comfortable using chatbots to discuss their healthcare needs. Additionally, prior research suggests that chatbots will become an essential component of healthcare providers’ customer experience strategies. Shortages of medical practitioners to support aging populations could impact chatbot usage, for example, the German government expects that it will need 3 million more nurses by 2060. Increased sophistication of conversational AI platforms leading to a greater percentage of enquirers being completed entirely via AI chatbots, freeing up the medical staff line and saving countries’ healthcare systems around 3.7 billion dollars by 2023.
Today, healthcare leaders need to develop strategic initiatives that utilize digital health behavior tools to ensure that the information collected is transferred to a person’s medical record and other applications, such as appointment scheduling or for those dispensing prescriptions. This means that providers of medical records and line of business applications will need to make their existing systems interoperable with digital technologies such as chatbots. Chatbots can transform how patients engage with their healthcare organization, taking the pressure off overstretched staff and resources. However, this approach requires investment in security, integration, and promotion to ensure greater trust in chatbot use, and that resulting time-saving and benefits are not lost.
The WHO director-general recently called for innovative pandemic responses. Towards this aim, chatbots are already being developed to contribute to the fight against C-19. If designed effectively, AI chatbots may help prevent misinformation, aid in symptom detection, engage in infection–limiting behaviors, and lessen the mental health burden of the pandemic response. In a pandemic, no groups of people remain unaffected for long. Together, patients, healthcare workers, academics, technology companies, and governments can ensure that well-designed chatbots generate the appropriate responses.
Within the current learning health system environments, greater effort is required to increase the awareness of when, where, and how to receive antiviral treatments. The current drawback of treatments in Ontario is that treatment must be initiated within 5 days of symptom onset to be effective. However, individuals require both a positive test result and a doctor’s prescription, making that 5-day window a challenge. More testing should be made readily available outside of the hospital setting such as home and remote testing, to aid in shortening the 5-day window. Tools such as the CRA-Chatbot can support the patient journey and aid in the development of an action plan based on the resulting recommendations.
It was perceived that a personalized vaccine scheduler would be a useful feature, to help individuals determine when they can take their next dose. In reality, the fluidity of the different public health rules on provincial levels and the complexity of scenarios such as types of vaccines and novel C-19 variants made the code too complicated and unmanageable. More complex algorithms will be implemented to include provincial vaccination timeline mandates and the effects and symptoms of new C-19 variants.
Conclusion
The CRA-Chatbot utilizes binary responses and time restrictions as inputted from the user to generate one of three CSRI class responses; Low, Moderate, and High. The framework of this chatbot prototype is built around five key parameters that collate to generate a CSRI class response, along with recommendations. These five parameters are vaccine doses and dates, C-19 infection status, antibody test kit results, disease history, and age.
The ultimate objective over the duration of the C-19 pandemic is to provide the best protection from severe disease, hospitalization, and death with the lowest number of doses of available C-19 vaccines; the best way to approach this is for individuals to take the vaccine only when it is needed, on a personalized basis, instead of the blanket age range. Learning from past experiences, the best chance to manage C-19 globally is to make vaccines and treatments available for everyone, everywhere, especially those who are at high risk. Continuing efforts should also be initiated to attain vaccine equity, which would reduce the chances of deadly variants.
References
-
Dimeglio C, Herin F, Da-Silva I, Porcheron M, Martin- Blondel G, et al. (2022) Post-Vaccination Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Antibody Kinetics and Protection Duration. Clinical Infectious Diseases 75(1): e924-e925.
-
Notarte KI, Guerrero‐Arguero I, Velasco JV, Ver AT, Santos de Oliveira MH, et al. (2022). Characterization of the significant decline in humoral immune response six months post‐SARS‐CoV‐2 mRNA vaccination: A systematic review. Journal of Medical Virology 94(7): 2939-2961.
-
Public Health Agency of Canada (2022) Canadian COVID-19 vaccination coverage report.
-
Olla, Tan (2022) Digital Health Care: Perspectives, Applications, and Cases. In: 1st (Edn.)_,_ Jones & Bartlett (Ed.), pp: 350.
-
Marsch LA (2021) Digital health data-driven approaches to understand human behavior. Neuropsychopharmacology 46(1): 191-196.
-
Milne-Ives M, Homer S, Andrade J, Meinert E (2022) Associations Between Behavior Change Techniques and Engagement With Mobile Health Apps: Protocol for a Systematic Review. JMIR research protocols 11(3): e35172.
-
De Cock C, Van Velthoven M, Milne Ives M, Mooney M, Meinert E (2020) Use of Apps to Promote Childhood Vaccination: Systematic Review. JMIR mHealth and uHealth 8(5): e17371.
-
Strauss G, Flannery JE, Vierra E, Koepsell X, Berglund E, et al. (2022) Meaningful engagement: A crossfunctional framework for digital therapeutics. Frontiers in digital health 4: 890081.
-
Weizenbaum J (1966) ELIZA-a computer program for the study of natural language communication between man and machine. Communications of the ACM 9(1): 36-45.
-
Walwema J (2021) The WHO health alert: Communicating a global pandemic with WhatsApp. Journal of Business and Technical Communication 35(1): 35-40.
-
Bhirud N, Tataale S, Randive S, Nahar S (2019) A literature review on chatbots in healthcare domain. International journal of scientific & technology research 8(7): 225-231.
-
Miner AS, Laranjo L, Kocaballi AB (2020) Chatbots in the fight against the COVID-19 pandemic. NPJ digital medicine 3(1): 1-4.
-
Chaplin DD (2010) Overview of the immune response. Journal of allergy and clinical immunol_o_gy 125(2): S3- S23.
-
Delves PJ, Roitt IM (2000) The immune system. New England journal of medicine 343(1): 37-49.
-
Hoffman W, Lakkis FG, Chalasani G (2016) B cells, antibodies, and more. Clinical Journal of the American Society of Nephrology 11(1): 137-154.
-
Nicholson LB (2016) The immune system. Essays in biochemistry 60(3): 275-301.
-
Janeway CA, Travers P, Walport M (2001) Immunobiology: The Immune System in Health and Disease. 5th edition. New York: Garland Science. Immunological memory.
-
Lo Sasso B, Giglio RV, Vidali M, Scazzone C, Bivona G, et al. (2021) Evaluation of Anti-SARS-Cov-2 S-RBD IgG Antibodies after COVID-19 mRNA BNT162b2 Vaccine. Diagnostics (Basel, Switzerland) 11(7): 1135.
-
Favresse J, Bayart JL, Mullier F, Elsen M, Eucher C, et al. (2021) Antibody titres decline 3-month post-vaccination with BNT162b2. Emerging microbes & infections 10(1): 1495-1498.
-
Ireland G, Whitaker H, Ladhani SN, Baawuah F, Subbarao S, et al. (2022) Serological responses to COVID-19 Comirnaty booster vaccine, London, United Kingdom, September to December 2021. Eurosurveillance 27(1): 2101114.
-
Bonnet B, Chabrolles H, Archimbaud C, Brebion A, Cosme J, et al. (2022) Decline of humoral and cellular immune responses against SARS-CoV-2 6 Months after Full BNT162b2 vaccination in hospital healthcare workers. Frontiers in immunology pp: 784.
-
Bayart JL, Douxfils J, Gillot C, David C, Mullier F, et al. (2021) Waning of IgG, total and neutralizing antibodies 6 months post-vaccination with BNT162b2 in healthcare workers. Vaccines 9(10): 1092.
-
Hall V, Foulkes S, Insalata F, Kirwan P, Saei A, et al. (2022) Protection against SARS-CoV-2 after Covid-19 vaccination and previous infection. New England Journal of Medicine 386(13): 1207-1220.
-
Levin EG, Lustig Y, Cohen C, Fluss R, Indenbaum V, et al. (2021) Waning immune humoral response to BNT162b2 Covid-19 vaccine over 6 months. New England Journal of Medicine 385(24): e84.
-
Terpos E, Karalis V, Ntanasis-Stathopoulos I, Gavriatopoulou M, Gumeni S, et al. (2021) Robust neutralizing antibody responses 6 months post- vaccination with BNT162b2: a prospective study in 308 healthy individuals. Life 11(10): 1077.
-
Bar On YM, Goldberg Y, Mandel M, Bodenheimer O, Freedman L, et al. (2021) Protection of BNT162b2 vaccine booster against Covid-19 in Israel. New england journal of medicine 385(15): 1393-1400.
-
Chenchula S, Karunakaran P, Sharma S, Chavan M (2022) Current evidence on efficacy of COVID‐19 booster dose vaccination against the Omicron variant: A systematic review. Journal of Medical Virology 94(7): 2969-2976.
-
Krause PR, Fleming TR, Peto R, Longini IM, Figueroa JP, et al. (2021) Considerations in boosting COVID-19 vaccine immune responses. The Lancet 398(10308): 1377-1380.
-
Alidjinou EK, Demaret J, Corroyer-Simovic B, Labreuche J, Goffard A, et al. (2022) Immunogenicity of BNT162b2 vaccine booster against SARS-CoV-2 Delta and Omicron variants in nursing home residents: A prospective observational study in older adults aged from 68 to 98 years. The Lancet Regional Health-Europe 17: 100385.
-
Seiffert P, Konka A, Kasperczyk J, Kawa J, Lejawa M, et al. (2022) Immunogenicity of the BNT162b2 mRNA COVID-19 vaccine in older residents of a long-term care facility: relation with age, frailty and prior infection status. Biogerontology 23(1): 53-64.
-
Keeton R, Richardson SI, Moyo Gwete T, Hermanus T, Tincho MB, et al. (2021) Prior infection with SARS-CoV-2 boosts and broadens Ad26. COV2. S immunogenicity in a variant-dependent manner. Cell host & microbe 29(11): 1611-1619.
-
Peterhoff D, Einhauser S, Beileke S, Niller HH, GüntherF, et al. (2022) Comparative Immunogenicity of COVID-19 Vaccines in a Population-Based Cohort Study with SARS- CoV-2-Infected and Uninfected Participants. Vaccines 10(2): 324.
-
Tantuoyir MM, Rezaei N (2021) Serological tests for COVID‐19: Potential opportunities. Cell biology international 45(4): 740-748.
-
Fujimoto AB, Keskinocak P, Yildirim I (2021) Significance of SARS-CoV-2 specific antibody testing during COVID-19 vaccine allocation. Vaccine 39(35): 5055-5063.
-
Zhou Y, Zhang L, Xie YH, Wu J (2022) Advancements in detection of SARS-CoV-2 infection for confronting COVID-19 pandemics. Laboratory investigation 102(1): 4-13.
-
(2022) National Center for Immunization and Respiratory Diseases, Division of Viral Diseases. People with certain medical conditions. Centers for Disease Control and Prevention.
-
Fan X (2021) Utilization of Self-Diagnosis Health Chatbots in Real-World Settings: Case StudyJ Med Internet Res 23(1): e19928.
-
Almalki M, Azeez F (2020) Health Chatbots for Fighting COVID-19: a Scoping Review. Acta informatica medica 28(4): 241-247.
-
Di Fusco M, Lin J, Vaghela S, Lingohr-Smith M, Nguyen JL, et al. (2022) COVID-19 vaccine effectiveness among immunocompromised populations: a targeted literature review of real-world studies. Expert review of vaccines 21(4): 435-451.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda