Quality in Health Services and its Challenge in the Ecuadorian Reality
This article constitutes a bibliographic review of the different components that make up quality in health services, analyzed from different perspectives, such as the role played by the human factor and its training in a humanistic, competent, and timely treatment at all levels of attention. Characterizing the existing structure in Ecuador is carried out to ensure the quality of health services. The elaboration and application of clinical practice guides stand out as standardized instruments of best medical practices. It is concluded: that the fragmentation, segmentation, and inequity in health services in the South American region and Ecuador, as well as deficiencies in quality control bodies, limit the comprehensive management and efficiency of public health, and peculiarly in the decisive role that the first level of attention must play.
Introduction
The quality of health services has a particular and, at the same time, very extensive connotation about other types of services due to the breadth of these services, and that half-satisfaction on the part of the client or patient is not accepted. They demanded the most significant effort from these institutions to respond to all expected expectations.
The number of elements that make up these services has conditioned different definitions of quality in health care, trying to address scientific-technical components, human performance, and even the physical state of the buildings, making it very difficult to integrate the entire procedure. In a single definition, especially if one considers that the perception of quality differs between the patient and that planned by the directors of the different health institutions. In the report expressed by Tápanes, et al. [1], aspects such as diligence, effectiveness in procedures, and proper use of means for diagnosis are also implicit, considering that a quality service... “implies giving an effective response to the health problems or situations … through the application of necessary standards, procedures and diagnostic-therapeutic protocols, as well as the verification of the medical instruments and means used”.
On the other hand, some concepts can be seen from a strategic vision such as the one proposed by the Pan American Health Organization (PAHO), where the conception of quality is extended to other perspectives, considering that it represents “satisfying health needs of people, families, and communities based on best practices, ethics, and scientific knowledge, contributing to equity and well-being, leaving no one behind, which implies particular attention to diversity and people and populations in a situation of vulnerability” [2].
Adding to the concept of quality, the component of equity conceived by PAHO, it can be seen that this aspiration then faces the existing segmentation of these services in the Latin American region, where the problem of poverty and, in particular, poverty extreme, lead to inequities in access to health care for a large part of the population. The figures described by the Economic Commission for Latin America and the Caribbean (ECLAC) reveal that as of 2018, the poverty and extreme poverty rates reflect a respective increase of 27.8% and 7.8% in 2014 to 30.2% and 10.2% in 2017, being significantly higher in people living in rural areas, and specific sectors of the population such as children, adolescents, and young people, indigenous peoples, the Afro- descendant population, women of legal age. Reproductive health, and people with lower levels of education. These figures represent 184 and 62 million people, respectively [3].
Achieving more significant equity in access to health services, as an aspiration of PAHO, is greatly limited by these economic realities that undoubtedly make it difficult for millions of people to access these services due to territorial inequalities in terms of availability of the same and that extend to other aspects related to the availability of essential services such as water supply, sanitation, or adequate nutrition, derived from low purchasing power.
A report analyzing 2013-2014 shows that more than 1.2 million deaths could have been avoided in the Region of the Americas if the health systems had offered accessible, timely, and reliable services. Quality [2]. Some surveys reveal that 30% of people in the region of the Americas still lack access to care, and of those who receive it, less than 40% rate the quality as good [2]. This demonstrates the existing gap in improving health services in this region.
These gaps emerge more visibly in times of contingencies, such as the experiences left in the confrontation of COVID-19, where functional weaknesses were shown at all levels of care of the health system in the region, in addition to the functionality of the strategies designed to deal with its spread and although a definitive evaluation of the most compelling experiences cannot yet be given, they confirm preliminarily the need to increase and properly plan public spending to achieve equitable access to a quality health service, that’s main, quality is available to everyone at all times [4]. This means doing everything right, somewhat, and timely in all circumstances.
In the present work, a bibliographic review is carried out on the different components that make up quality in providing a health service, constituting a permanent demand. This topic is contrasted from three dimensions, among which is: the culture of quality as a subjective element linked to the humane and humanistic actions of health personnel. An analysis is made on the standardization of quality systems and procedures promoted internationally by the governing bodies of health to seek homogeneity in the quality of these services. Finally, the policies and programs implemented in the country are exposed and analyzed. Ecuador focused on achieving excellence in services, and the limitations that cause fragmentation, existing segmentation throughout the Latin American region, as well as the economic conditions that affect the effectiveness of the proposed improvement strategies for the achievement of service integral with quality, which constitutes a challenge in the face of these realities, that they are integrated and become a style of permanent action and systematic improvement in which the control bodies responsible for their implementation must play a highly decisive role, focused on the achievement of excellence in these services at all levels of health in Ecuador.
Methodology
To realize this article, a review of more than 80 secondary sources was carried out, as well as updated reports from international organizations linked to the sphere of health, economy, and population, such as the WHO, PAHO, and ECLAC, among others. , for these queries, the descriptors or keywords such as Quality Culture, Quality Management, Organization and Administration, Health Services, and others were used, trying, in any case, to use more recent publications. However, other older sources were also used to analyze and describe the evolution of quality approaches through the years. Likewise, the quality of the publications in terms of indexed scientific journals was taken into account, allowing us to elaborate and critically analyze the main topic of this article.
Results
Culture of Quality in Health. A Permanent Condition
Quality management, implemented as a standardized system in the health sector, acquires specific characteristics.
For example, unlike the industry, it is only possible to compare this where the human and technological action scenarios are very different from that of a health institution. A robot with artificial intelligence can monitor the quality of a given product within a serial production process [5]. Instead, patient care is personalized and varies in a particular way from one patient to another and with specific demands; each patient is different, and treatments do not necessarily have to work the same [6].
In this context, the formation of human capital focused on customer (patient) satisfaction is considered decisive in providing a quality service; for this reason, “the most successful organizations are those that recognize human resources as the most important asset of them” [7]. Having motivated, committed, and satisfied workers contribute significantly to the results. A positive attitude from health personnel improves user treatment, reduces clinical errors, and even contributes to the efficient management of material resources by generating fewer expenses [8].
“…it has been shown that for the patient, his priorities are to receive a dignified, humane, personalized, kind and respectful treatment; where it has highly qualified personnel, sufficient and prepared to provide the care it requires and that also has sufficient resources and an adequate environment to achieve it” [8]. It is essential to highlight that, according to contemporary trends, treatment with quality is not limited to only satisfying the patient. Still, that treatment should extend to the family and community due to what these factors contribute to the recovery process. Inside or outside of Health Services, in this perspective, the measurement of quality has been extended to the perception of the patient and the accompanying staff [9]. These factors must be incorporated more and more into the thoughts and actions of those who guide the trends in treatment and monitoring of patient care processes to promote and facilitate a multifunctional environment increasingly favorable to achieve comprehensive service quality.
It should not be ignored that “The hospital turns out to be a hostile place for both the patient and the accompanying family member, where they are alone, frightened, afraid, where they must adapt to a strange environment and a specialized language, and even find themselves in unknown cities and hospitals, depending on people they do not know and facing problems they do not understand” [9]. In this sense, the reaffirmation of this condition by workers at this level of care should be promoted, as well as the strengthening of primary care to avoid hospital admission as much as possible, which also implies a more significant expenditure of resources.
In this sense, PAHO [2] recognizes that a sound health system focused on primary or outpatient care would avoid hospital admissions that also increase costs in health systems throughout Latin America and the Caribbean, which can be reduced by more than 40%. Still, due to the weak development of preventive medicine and treatments, to which not many have access, and deficiencies in the quality of the first level, they are forced to attend the emergency services for situations that can be addressed at the first level.
However, regardless of the levels of care, user-patients expect to find care that meets their needs in any of the health institutions, that provides immediate attention to their problems, and that they must be willing to know the suggestions, claims, and satisfactions to improve professional actions [10].
According to Vargas, et al. [10] Periodic evaluations of quality are required, which must be considered as a whole where multiple factors interact with tangible or intangible characteristics, whether they are technical-scientific, administrative, economic, human, interpersonal relations, among others, but which ultimately meet expectations. Of the user-patient. However, of these characteristics, some studies show that what the patient values most is good treatment, knowledge, and the interest shown and transmitted by health professionals at the time of care while offering clear and understandable concerning your privacy [11].
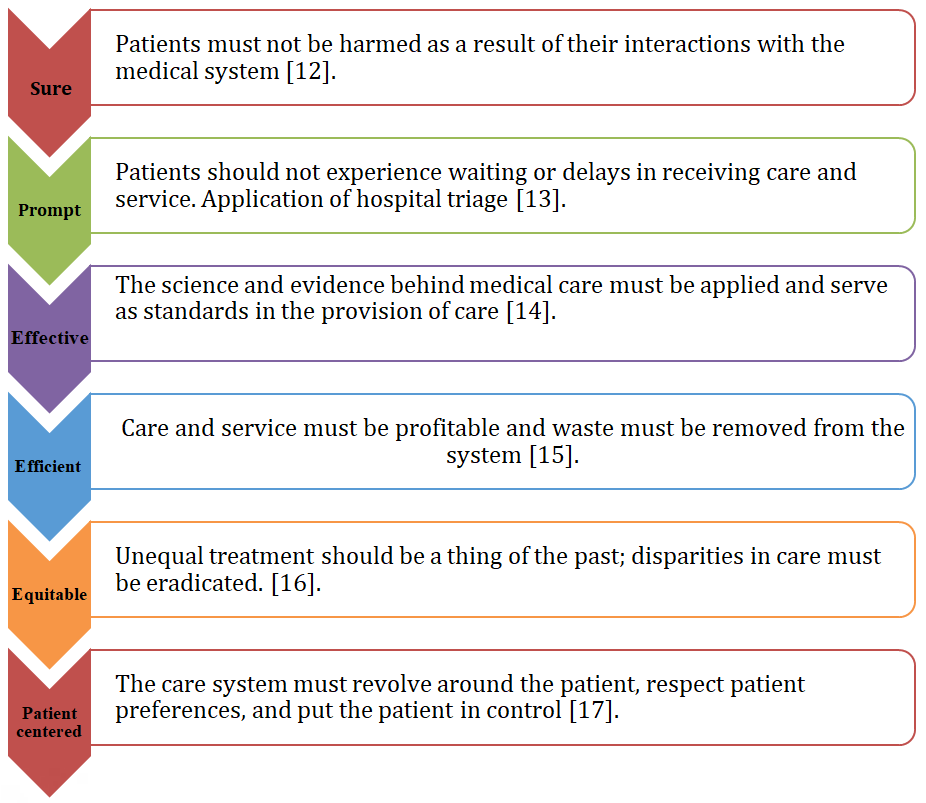
Figure 1 describes some of the dimensions of quality that, according to different authors, should be conceived as general rules to be followed by a health institution at any level of care. The six dimensions listed in Figure 1 corroborate the prevalence of human behavior and interpersonal relationships over the technical and administrative dimensions. This shows that a health service expected by the patient will be centered, in the first instance, on friendly behavior, with ethics, adequate communication, and efficient and specialized care, which only health personnel can provide.
For these conditions to be homogeneous or standardized, it is recommended to implement standardized quality systems that constitute the measurement and management pattern, which unifies a service of excellence at all levels of care.
Quality From the Perspective of Standardized Management Systems (Iso 9001) and Global Policies for its Development in Health
Providing quality services and products focused on customer satisfaction remains a rising trend, primarily motivated by the increasingly competitive nature of the environment or also by the understanding of managers that quality is a determining factor of economic efficiency, optimization of resources, productivity, and improvement of the work environment, which ultimately contribute to a better image and social recognition of any health institution. To achieve international standards, regulations have been developed focused on facilitating, in a more effective way, the purposes of organizations, considering quality management systems through standardized norms such as ISO (International Standard Organization), which provide planning tools, organization, evaluation, and systematic identification of opportunities for improvement which, in other words, facilitates the proper functioning of organizations [18].
However, there is still much resistance to the implementation of these management systems; it is common to hear the opinion that maintaining a quality management system generates many expenses, avoiding the analysis of what it represents, the cost of non-quality, which in the area of health can mean in some cases between 20 and 40% of the costs of the service [19]. For example, Valenzuela [20] affirms that, generally, adequate financial control of the waste generated in the different processes is not carried out, seeing these as justified without considering that they can be reduced with few actions, making it impossible for the decision-making of the high management or specific departments where the most significant waste has been identified, to eradicate failures or bad practices, which ultimately result in a lower cost of health services at any level of care.
A periodic review of the plan’s effectiveness, the training of human resources, a methodologically organized organizational system, interaction with clients, and commitment at all levels constitute the fundamental bases for achieving the objectives and goals proposed for Total Quality Management. “Implementing a system for its management is not an easy task and requires a cultural change in the organization that involves all the actors of the institution to satisfy the needs and preferences of patients” [21].
In Table 1, a comparison is made of the most frequent criteria that oppose the benefits and obstacles to implementing quality management systems.
| Benefits of management systems | Negative criteria |
|---|---|
| ● The implementation of quality. Management system brings both internal and external benefits (Improves the image of organizations). | ● It implies an initial investment and routine equipment maintenance to achieve highly reliable measurements and results. |
| ● Increases the reputation of the company. | ● A period is required for the scope of an external certification |
| ● Improves interpersonal relationships | ● Staff resistance to handling the new documentation |
| ● Influences the motivation of your employees. | ● Need for an initial training process |
| ● Promotes internal satisfaction of human resources. | ● Lack of organizational focus aimed at continuous improvement and customer satisfaction (Change of mentality) |
| ● Increases customer satisfaction and financial indicators. | ● Adaptation to carrying out internal and external audits |
| ● Increased efficiency and | |
| ● Competitiveness (More organized processes). |
Table 1: The opposition between the benefits of management systems and negative criteria Benefits of management systems Negative
Source: Theories, Models and Quality Management Systems [22]. Table 1: The opposition between the benefits of management systems and negative criteria Benefits of management systems Negative criteria.
Despite the initial resistance experienced by people or organizations to implementing a management system, international experience confirms that the number of companies and service companies certified yearly is increasing. However, it is undoubtedly recognized that these are found in countries with more developed economies, led by China (with 342,800 certified companies in 2017), associating this with a better corporate image, brand position, customer loyalty, and productivity [22].
But there is also consensus in affirming that beyond the documents and standardized technical procedures required for the certification of management systems, the most critical measurement indicator is found in the necessary change in behavior and organizational culture that distinguishes the company itself. Certificate, in which human capital has the most significant role [22]. And it is undoubtedly one of the most demanding of this change in behavior aimed at excellent care in the health sector.
Quality standards, infrastructure, equipment, medicines, personnel, and budget will improve the population’s health according to sectoral policies, current regulations, and approved care models [23].
It is required on the part that medical personnel can attend with professional and scientific effectiveness while incorporating humanism for quality care according to the population’s needs and their regular performance [24].
One of the core elements in monitoring a quality management system is the homogeneity or standardization of care practices, focused on the excellence of health services at all levels.
One of the ways promoted by PAHO to ensure quality is the Clinical Practice Guidelines (CPG), with which unification of the best medical experiences is achieved and helps both medical staff and patients to make decision-making based on the application of the best quality care standards, derived from systematic studies, prevention criteria, timely diagnosis, treatment and follow-up of patients. However, it is recognized that professional capacity and available resources play a fundamental role in clinical practice, in addition to scientific efficacy [25]. The guidelines only partially replace medical criteria but facilitate achieving standardized health services in all places and levels of care.
With the benefits achieved with the CPGs, PAHO, in its objective 1.1. to develop in 2020-2025 in the 57th. Assembly of said organization establishes in indicator 1.1.4 “the development, implementation, and evaluation of the impact of clinical practice guidelines based on evidence.” PAHO [2] to improve the quality of care in the provision of Health Services, which includes individuals, families, and communities in the provision of comprehensive health services”.
Aligned to this purpose, the Ministry of Public Health of Ecuador (MSP) has generated the publication Clinical Practice Guides, with emphasis on maternal and child care, severe or catastrophic diseases, and chronic non- communicable pathologies, with a view to medical personnel, have an instrument for clinical decision making, improve and standardize the quality of care and therefore reduce the mortality of the Ecuadorian population, prepared from 2013 to 2019, with the following [26].
and treatment of spontaneous, incomplete, delayed, and recurrent abortion; 4. Cystic fibrosis; 5. Transfusion of blood and its components; 6. Hypertensive disorders of pregnancy; 7. Systemic lupus erythematosus; 8. Nutritional treatment of pediatric and adolescent patients with galactosemia; 9. Urinary tract infection in pregnancy; 10. Diagnosis, treatment, and monitoring of patients with type 1 Gaucher disease; 11. Comprehensive Care Guide for Adults and Adolescents with HIV/AIDS infection; and, 12. Prevention and Control Guide for mother-to-child transmission of HIV and congenital syphilis and comprehensive care in children with HIV/ AIDS.
- The Year 2014: 8 clinical guidelines for managing: 1. Food and nutrition of pregnant women and breastfeeding mothers; 2. Diagnosis and treatment of anemia in pregnancy; 3. Palliative care; 4. Diagnosis and treatment of pregestational and gestational diabetes; 5. Diagnosis and treatment of congenital adrenal hyperplasia; 6. Diagnosis and treatment of vaginal infection in obstetrics; 7. Palliative care guide for citizens, 8. Diagnosis and treatment of patients with osteogenesis imperfect.
- The Year 2014: 8 clinical guidelines for managing: 1. Food and nutrition of pregnant women and breastfeeding mothers; 2. Diagnosis and treatment of anemia in pregnancy; 3. Palliative care; 4. Diagnosis and treatment of pregestational and gestational diabetes; 5. Diagnosis and treatment of congenital adrenal hyperplasia; 6. Diagnosis and treatment of vaginal infection in obstetrics; 7. Palliative care guide for citizens, 8. Diagnosis and treatment of patients with osteogenesis imperfecta.
- The Year 2015: 8 clinical guidelines: 1. Cesarean delivery care; 2. Caries; 3. Premature newborn; 4. Diagnosis and treatment of congenital hypothyroidism; 5. Neonatal sepsis; 6. Labor, postpartum and immediate delivery care; 7. Therapeutic abortion care; and 8. Maternal component pocket guide.
- The Year 2016: 12 guides aimed: 1. Prevention, diagnosis, treatment, and control of tuberculosis; 2. Dental trauma; 3. Newborn with difficulty breathing; 4. Prenatal management; 5. Dental treatment in pregnant women; 6. Hypertensive disorders in pregnancy; 7. Low back pain; 8. Diagnosis and treatment of acne; 9. Rheumatoid arthritis; 10. Diagnosis and treatment of congenital hemophilia; 11. Prevention, diagnosis, and treatment of allergy to cow’s milk protein; and 12. Hypertensive disorders of pregnancy.
- The Year 2017: 9 publications aimed: 1. Autism Spectrum Disorders in children and adolescents, detection, diagnosis, treatment, rehabilitation, and follow-up; 2. Community-acquired pneumonia in patients aged three months to fifteen years; 3. Type 2 diabetes mellitus; 4. Treatment of cancer pain in adults;
5. Anomalies of placental attachment and fetal blood vessels; 6. Gestational diabetes; 7. Hodgkin lymphoma in adults; and 8. Diagnosis and treatment of depressive episode and recurrent depressive disorder in adults.
- The Year 2017: 9 publications aimed: 1. Autism Spectrum Disorders in children and adolescents, detection, diagnosis, treatment, rehabilitation, and follow-up; 2. Community-acquired pneumonia in patients aged three months to fifteen years; 3. Type 2 diabetes mellitus; 4. Treatment of cancer pain in adults; 5. Anomalies of placental attachment and fetal blood vessels; 6. Gestational diabetes; 7. Hodgkin lymphoma in adults; and 8. Diagnosis and treatment of depressive episode and recurrent depressive disorder in adults.
- The Year 2018: the second edition of Prevention, diagnosis, treatment, and control of tuberculosis and the Clinical Guide for prevention, diagnosis, and treatment of Chronic Kidney Diseases are published.
- The Year 2019: The Clinical Guide for managing hypoxic-ischemic encephalopathy of the newborn is published, and two Clinical Guides are updated: 1. Arterial Hypertension; and 2. Prevention, diagnosis, and treatment of human immunodeficiency virus (HIV) infection in pregnant women, children, adolescents, and adults. As a baseline criterion in the evaluation of this indicator, by 2020, it was proposed to reach seven countries with compliance with this requirement in the Region of the Americas, and by 2025 at least twenty-five countries, so that Ecuador, already in 2020, became part of this baseline goal line within the region [25].
The implementation of these guidelines has responded to the country’s desire to standardize action protocols in the health system, which has been shaped as an action model to bridge the gaps from one level to another and homogenize services throughout the country; a preliminary analysis of it is made below.
Ecuadorian Model for Quality Assurance
The Ecuadorian model of quality management Article 52 of the Constitution of the Republic of Ecuador [27] states, “People have the right to have goods and services of the highest quality and to choose them freely, as well as accurate and not misleading information about its content and characteristics. To fulfill this mandate, a global system is designed to guarantee quality in Ecuador’s different spheres of production and services.
In Figure 2, you can see the synthesized scheme of the operation of the Ecuadorian quality system according to current action models.
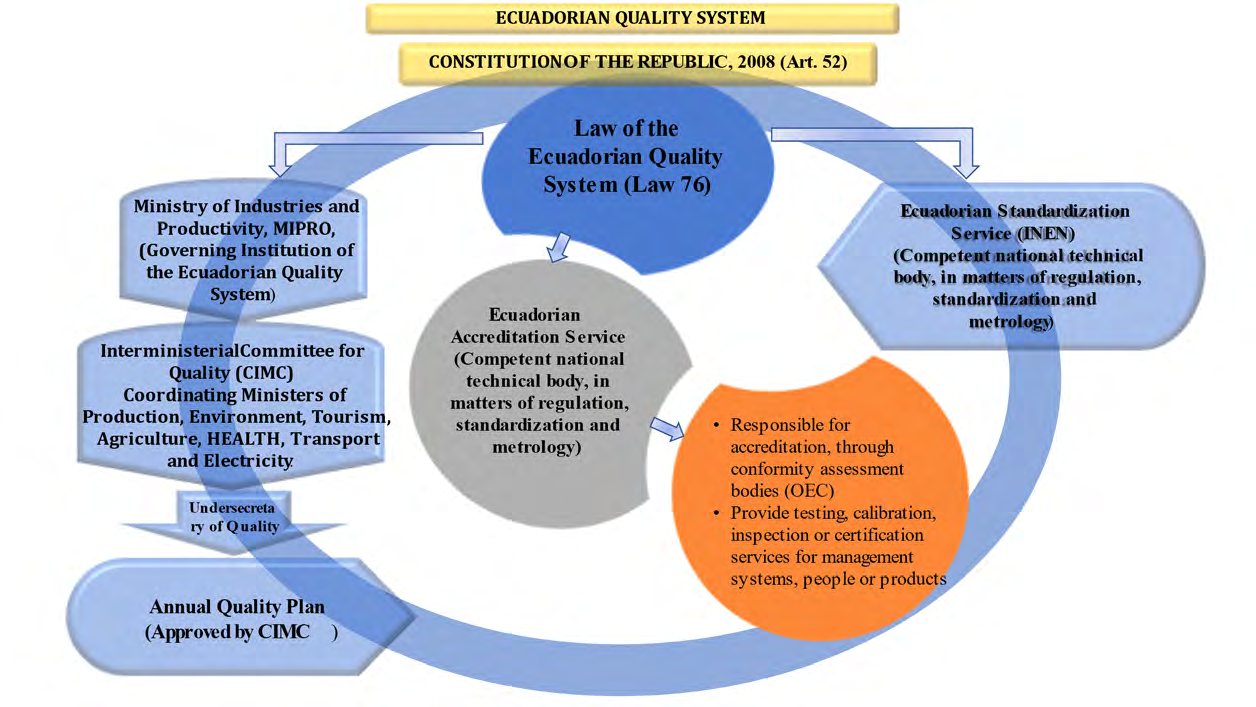
Source: Prepared by the authors. Figure 2: Operation of the Ecuadorian quality system.
Within the specific area of health, Law No. 67, “Organic Health Law”, establishes in Art. 6.- It is the responsibility of the Ministry of Public Health to design and implement comprehensive and quality care programs for people during all stages of life and according to their particular conditions [28].
On the other hand, in Ecuador, the quality policy is controlled through the National Directorate for the Quality of Health Services, whose Mission is [29].
“Guarantee the quality, efficiency, and effectiveness in the provision of health services provided by the Ministry of Public Health, within the framework of the rights of people, to achieve excellence in services, following established sectoral policies, quality models, regulations, and strategic guidelines.” Among its multiple responsibilities, it monitors and evaluates the quality of quality audit processes in health care, which implement technical tools for measuring user satisfaction, as well as attention to claims or complaints related to the quality of care in health services.
In addition to the legal and regulatory guidelines, strategic care programs are promoted by the central government of Ecuador, such as the “Plan for the Creation of Opportunities 2021-2025” and the Comprehensive Health Care Model (MAIS), among others. However, it is considered that the country must be prepared with long-term approaches based on demographic trends and the occurrence of natural events, epidemiological crises, and others [30]. This preparation must integrate the created infrastructure and fully trained human capital.
As another of the goals, work is being done to achieve the international guidelines, governed by the international agreements of PAHO, included in the Strategy and Action Plan to Improve the Quality of Care in the Provision of Health Services 2020-2025, of the which Ecuador is a signatory country.
The indicators of Ecuador have fluctuated since the Covid-19 pandemic; in 2019, there was evidence of progress in the socio-sanitary indicators of life expectancy, Gini index, and mortality rates, as evidenced in Table 2 next.
| Demographic and Socioeconomic Indicators | Health indicators | ||
|---|---|---|---|
| Life expectancy (2019) | 77 years Increases from 5.9 in men and 6.2 in women | Maternal mortality | 42.8 for every 100,000 live births |
| Births (2019) | 337,1 thousand | Neonatal Mortality | 5,6 for every 1,000 live births |
| Fertility rate (2019) | 2,4 children/woman | Child mortality | 9,7 for every 1,000 live births |
| Adolescent fertility rate (2019) | 78,8 for 1000 women | Deaths in <5 years | 13,8 for every 1,000 live births |
| Population growth (2019) | 1,6% | New HIV cases | 23,9 for every 100,000 inhabitants |
| Gross Domestic Product Growth | 1,4% | Tuberculosis incidence | 43,0 for every 100,000 inhabitants |
| Gini coefficient | 44,7% | overall mortality | 5,5 for every 1,000 inhabitants |
| median age | 28 years old | Communicable disease mortality | 78,0 for every 100,000 inhabitants |
| Deaths (2019) | 88,7 Thousand | Mortality from non- communicable diseases | 405,0 for every 100,000 inhabitants |
| Urban population | 64% | Mortality from ischemic heart disease | 60,4 for every 100,000 inhabitants |
Table 2: ** Socio-sanitary indicators of Ecuador.
Source: Pan American Health Organization [31]. Table 2: Socio-sanitary indicators of Ecuador.
However, the pandemic and its mitigation measures generated a decline of -6.9% of GDP in 2020, with an improvement in 2021 of 6.5% with vaccination, since in 2021, there was a vaccination rate It reached almost 80% of complete schemes per 100 people, and a maternal mortality ratio of 9.7 of pregnancies positive for Covid-19 per 100,000 live births [32].
It is interesting to mention that the Health Security Index, which analyzes prevention; detection and notification; fast answer; Health System; commitments to improve national capacity, financing, and global standards; the risk environment, granting a scale from 0 to 100; scores Ecuador with 48 points, above the world average of 38.9; in agreement with the registry with the mortality rate, as evidenced in the figure [32].
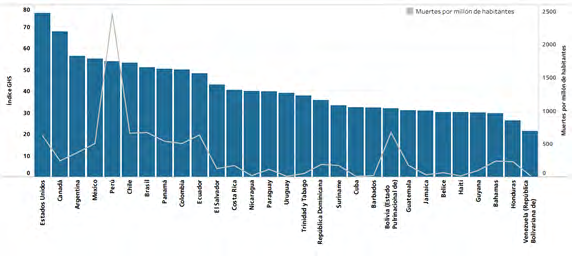
Source: Pan American Health Organization [32]. Figure 3: Global Health Security Index World Index of Health Security and mortality in the Region of the Americas, by country, 2021.
However, from the perspective of PAHO, in its call to “leave no one behind,” it is considered that the segmentation and fragmentation that characterize health systems in the region make it difficult for people to access quality health services, especially those with lower incomes. Still, at the same time, they cause an irrational and inefficient use of available resources and consequently a low satisfaction of people with the services received [33]. The health service in Ecuador does not differ from the rest of the countries in the region in terms of its fragmentation, inequity, and inefficiency, oriented towards providing individual attention, with insufficient financing and an unequal distribution of services, in addition to considering that there is no Adequate control for compliance with the care programs designed [34].
Some authors argue that the fragmentation of the health system in Ecuador hurts the operational capacity of the Public Health Ministry since it makes it challenging to provide feedback for the monitoring and control of compliance with public policies and better management of medical or healthcare resources, and also hinders standardization and homologation of services according to levels of care, which determines the effectiveness of the purpose of achieving a comprehensive approach in the health system [35].
It is recognized that the concept of comprehensive quality is not only limited to the technical quality of the service but also implies the guarantee of access to health facilities, friendly, humanistic, and timely treatment focused on families and communities [36]. In Ecuador during the Covid-19 pandemic, deficiencies emerged due to the curative approach that has prevailed in the country for many years above the primary and preventive level, which surprised all the country’s provinces even though some of the most affected, had met the rate of health personnel (medical and nursing professionals) of more than 25 per ten thousand inhabitants, promoted by PAHO, and with a ratio of 5 to 1 in terms of establishment of the public and private network, the first being the most used by the population. However, the non-consolidation of the first level of care could not overcome the timely capture of infected people, bringing an accelerated spread of infections and the consequent saturation in health units due to insufficient control, prevention, and epidemiological surveillance [37]. These realities are not yet resolved despite having been able to overcome the moments of this pandemic stage, so action to reduce the gaps must remain a daily challenge in the medium and long term.
The quality and security in the access and coverage of health services in Ecuador are not reduced to the medical care space; it requires the impact of the living conditions of the population, access to aspects that affect the quality of life, and the ability to respond to situations that violate the state of health. The provision of a safe environment, free of contamination, with the services required to maintain the quality of life in harmony with the diverse cultural characteristics of the country, is an indicator of justice and quality in the country’s health.
Conclusions
It is recognized that, in the health system field, in any country in the world, the quality of services constitutes a challenge permanently demanded by clients and personnel of health establishments at any level of care. To achieve and maintain this condition, a culture and a particular vocation towards a humanistic service with quality and warmth are required, where human capital intervenes to a greater extent over the regulations and laws that regulate it without failing to apply the latter.
In the case of Ecuador, it is recognized that its health system, despite the actions carried out to improve it, is still characterized by its fragmentation, segmentation, and inequity, which determines the effectiveness in the standardization and application of the best medical practices to all. Levels of care and geographical areas of the country, also recognizing deficiencies in the control and monitoring of the health programs designed. The non-consolidation of the preventive approach remains a current challenge, especially at the first level of care.
Conflicts of Interest
It is declared by the authors that there are no conflicts of interest
References
-
Tápanes W, Erasti MY, Arana RM, Román Santana R (2019) Quality Control in Public Health. Historical review. Rev Med Electrón 41(3): 809-813.
-
Pan American Health Organization (2019) Strategy and action plan to improve the quality of care in Health Services 2020-2025. Document 57th Board of Directors. 71st Session of the WHO Regional Committee for the Americas.
-
Abramo L, Cecchini S, Ullmann H (2019) Addressing health inequalities in Latin America: the role of social protection. Ciência & Saúde Coletiva 2020 25(5): 1587- 1598.
-
Economic Commission for Latin America and the Caribbean (ECLAC) (2020) The 2030 Agenda for Sustainable Development in the new global and regional context: scenarios and projections in the current crisis (LC/PUB.2020/5), Santiago.
-
Lee SM, Lee D, Kim YS (2019) The quality management ecosystem for predictive maintenance in the age of Industry 4.0. Int J Qual Innov 5(4).
-
Vasquez NB, Preciado IJ (2019) Epidemiological, clinical study of patients with diabetes mellitus, Riobamba Provincial Hospital. Bachelor’s thesis, Higher Polytechnic School of Chimborazo.
-
Santos LA, Miguel Guzmán MD, Noda Hernández ME, Álvarez López LF, Chacón GG (2016) Diagnosis of job satisfaction in a hospital care entity. Cuban Rev of Public Health 42: 407-417.
-
Tovar D, Rodríguez Y, Del Canto E, Martins V, Neto EB (2016) The quality of Venezuelan healthsystems: towards a positive attitude. Rev Científica e-Locução 1(09): 17-17.
-
Frausto VMR, Rico Venegas RM, Armendariz GV (2012) Perception of the accompanying family member regarding nursing care in hospitalization. Rev Enfermería global 11(1).
-
Gonzalez V, Valecillos V, Hernandez J, Carmen (2013) Quality in the provision of health services: Measurement parameters. Journal of Social Sciences 19(4): 663-671.
-
Rovere Herrera V, Rebolledo D (2021) Quality management and user satisfaction of the emergency service of the center type C Rioverde District 08D06. Revista Científica Conecta Libertad 5(2): 48-61.
-
Rocco C, Garrido A (2017) Patient safety and safety culture. Rev Las Conde 28(5): 785-795.
-
Vasquez R, Luna C, Ramos CM (2019) Hospital triage in emergency services. Rev of the Faculty of Human Medicine 19(1).
-
Gamboa L (2001) The doctor-patient relationship and the quality of medical care. Rev Conamed 6(3): 25-29.
-
Terán Rosero GJ, Mora Chuquer EJ, Gutiérrez Villarrea Md, Maldonado Tapia SC, Delgado Campaña WA, et al. (2017) The management of innovation in public health services. Cuban Rev Inv Bioméd 36(3).
-
Hernandez Betancourt J (2015) An urgent approach of the Cuban health system to quality. Electronic Rev. Dr. Zoilo E. Marinello Vidaurreta 38(7).
-
Serra JC (2016) Quality management in the Cuban health system. Medisan 20(5): 593-595.
-
Hernández H, Barrios I, Martínez D (2018) Quality management: an essential element for the development of organizations. Free Criterion 16(28): 179-195.
-
Saturno-Hernández PJ, Hernández-Avila M, Magaña- Valladares L, García-Saisó S, Vertiz-Ramírez J (2015) Comprehensive training strategy for the continuous improvement of the quality of health services. Rev. Public Health of Mexico 57: 275-283.
-
Valenzuela LF (2016) The costs of poor quality as the fifth element of the cost: theoretical approach in the management of competitiveness amid accounting convergence. Rev. of the Faculty of Economic Sciences: Research and Reflection 24(1): 63-84.
-
Forrellat M (2014) Quality in health services: an unavoidable challenge. Cuban Rev. of Hematology, Immunology, and Hemotherapy 30(2): 179-183.
-
Chacon Songs J, Rujel Kamarova S (2018) Theories, Models, and Quality Management Systems. Rev. Spaces 39(50): 14.
-
Haro-Alvarado JM, Haro-Alvarado JI, Macías-Intriago MG, López Calderón BA, Ayala-Astudillo MD, et al. (2018) Quality management system in the health care service. Rev. Pole of Knowledge. (Issue no. 27). 3(11): 210-234.
-
Hernandez BE, Coffin CN, Miralrio MC, Jimenez RML, Vite SA (2015) Towards medical bioethics: Vocation or training? Rev Elec Psic Izt 18(2): 451-469.
-
Toledo AM, Portuondo M, Mejías Y, Santana L (2017) Proposal of actions for developing evidence-based clinical practice guidelines in the national health system. Rev. Higher Medical Education 31(1): 178-192.
-
Ministry of Public Health of Ecuador (2021) Clinical practice guides.
-
Constitution of the Republic of Ecuador (2008) Legislative Decree 0 Official Registry 449 of 20-Oct-2008 Last modification.
-
Law 67. Organic Law of Health (2015) Official Registry Supplement 423 of 22-Dec-2006 Last modification: 18- Dec-2015.
-
Ministry of Public Health of Ecuador (2021) National Directorate for Quality of Health Services.
-
Parreno Urquizo AF, Ocaña Coello SP (2018) Environmental trends impact the management of the quality of health services in Ecuador. Caribbean Rev. of Social Sciences.
-
Pan American Health Organization (2019) Fundamental indicators 2019: Health trends in the Americas. Washington, DC: PAHO.
-
Pan American Health Organization (2022) Health in the Americas 2022. Overview of the Region of the Americas in the context of the COVID-19 pandemic. Washington, DC: PAHO.
-
Pan American Health Organization (2017) Health in the Americas PAHO; Abstract: regional overview and country profile. Washington DC, USA, PAHO.
-
Castelo WP, Castelo AF, Rodríguez Díaz JL (2016) Patient satisfaction with emergency medical care. Cuban Rev of Nursing 32(3).
-
Molina Guzman A (2018) Operation and governance of the National Health System of Ecuador. Rev. of Social Sciences 63: 185-205.
-
Ubillus P, Patricia O (2018) Experience in the implementation of the Comprehensive Health Care Model based on Family and Community from the National Health Strategy for Family Health. Rev. Peru. Gyneco. OB. 64(3): 375-382.
-
Velasco M, Hurtado F, Tapia J (2020) Unequal geographic access to health in Ecuador. Originally published in the Social Observatory of Ecuador and FES-Ildis.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda