Evolution of Cholecystectomy-Gall Bladder must be Removed not because it Contains Stones but Forms them
Normally, human bile contains enough chemicals to dissolve the cholesterol excreted by our liver. But if our liver excretes more cholesterol than the bile can dissolve, the excess cholesterol, too much bilirubin, or not enough bile salts, first form into crystals and eventually turn into stones when stored in the gall bladder. The estimated overall prevalence of cholelithiasis is 10–15% in the general population, with some differences across countries, ethnic and age groups. The good fact is most of the gall stone patients are asymptomatic. The prevalence of gall stones is around 6% of the total population in India, with a clear predominance among females with 10% and 3% in men. In India among 808 million adult population 81 million will suffer Cholelithiasis every year and a conservative 1.6 million (2%) of them would need surgery. Among American adults the prevalence of cholelithiasis is about 10% while in Western Europe the prevalence ranges from 5.9% to 21.9%. More than one million Americans are diagnosed with gallstones every year, joining about 38 million who already have the disorder. Cholecystectomy: the surgical resection and removal was and continues to be the permanent solution and the gold standard for the definitive management of symptomatic cholelithiasis. J. L. W Thudichum proposed a two-stage elective cholecystostomy in 1859, In the first stage, the inflamed gall bladder was sewed to the anterior abdominal wall through a small incision, to serve as a route for the removal of gall stone later in the second stage. Laparoscopic cholecystectomy (LC) since its inception in 1989 has become the gold standard treatment for gall stone disease. The technique of performing LC has undergone many changes and variations. Several surgeons have tried to reduce the size and number of ports to improve cosmetic and postoperative outcomes and developed their own different versions. The most recent development in technique of LC is single incision laparoscopic surgery (SILS) or single site laparoscopic cholecystectomy (SSLC). This review is a consequence of witnessing an elective Cholecystectomy and review of the prevailing cost across the country and health insurance coverage in India. As a public health problem Cholelithiasis can’t be prevented, and Cholecystectomy is needed to 1.6 million Indian adults each year costing a fortune. Currently it cannot be accessed by all, especially the poor and even lower middle socio-economic class. With overall, health insurance coverage of around 30%, that too among urbanites, mainly covered by employers in India is a public health challenge. Ayushman Bharat a national initiative launched on 23rd September 2018, a GOI health assurance initiative adapted by almost all State governments for providing accessible and affordable healthcare to the common man for secondary and tertiary care hospitalization is still in a nascent stage. Methodology: This review is based on an observation of Laparoscopic Cholecystectomy in a 3-star private hospital on a middle socioeconomic woman, followed by literature review and costs across India by the end of 2022.
Introduction
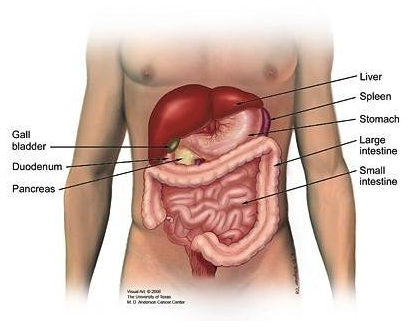
The gallbladder (cholecyst) is a small hollow organ where bile is stored and concentrated before it is released into the small intestine. Normally, our bile contains enough chemicals to dissolve the cholesterol excreted by our liver. But if our liver excretes more cholesterol than our bile can dissolve, the excess cholesterol, too much bilirubin, or not enough bile salts, first form into crystals and eventually into stones when stored in the gall bladder [1]. Blood cholesterol appears to play a role in the formation of gallstones. Therefore, it’s advised to avoid eating too often and large quantities of foods like meat pies, sausages and fatty cuts of meat butter, ghee, and lard, cream, hard cheeses, cakes and biscuits and food containing coconut or palm oil as all of them have a high saturated fat content. Gallstones can cause sudden, severe abdominal pain lasting 1 to 5 hours, sometimes it may last just a few minutes. The pain can be felt in the centre of your abdomen just under the ribs on your right-hand side-it may spread from here to your side or shoulder blade [1].
Gallstones are created in the gallbladder when the substances in the bile create hard, crystal-like particles. Eighty percent of gallstones are made of cholesterol and appear light in colour. About 20% of total gall stones are Pigment stones that are small, dark stones made of bilirubin and calcium salts that are found in bile. Risk factors for pigment stones include cirrhosis of the liver, biliary tract infections, hereditary blood cell disorders (sickle cell anaemia). Gallstones can be as small as a grain of salt or as large as a golf ball. The gallbladder may develop many smaller stones, or a single, often large one. It may even develop several thousand stones [2].
Bile Duct Stones
Gallstones that move out of the gallbladder can pass into our stomach. However, a stone may become lodged in our bile duct due to the size of the stone or the anatomy of the biliary tree. Thus, bile duct stones are gallbladder stones that have become lodged in the bile duct. Stones that become stuck in the ducts that lead to the duodenum can be both agonizing and dangerous [2].
The estimated overall prevalence of cholelithiasis is 10–15% in the general population, with some differences across countries and good fact is most of the patients are asymptomatic. The incidence of gall stones is around 6% of the total population in India, with a clear predominance among females, as it is seen that around 10% of women and 3% in men have it. In elderly people, it may go up to 20 per cent [2]. Among American adults the prevalence of cholelithiasis is about 10% while in Western Europe the prevalence ranges from 5.9% to 21.9%. More than one million Americans are diagnosed with gallstones every year, joining about 38 million who already have the disorder [3]. Fortunately, most people with gallstones do not have symptoms and do not require treatment [1]. The at-risk population to have cholelithiasis is described for ages as five ‘F’s standing for ‘fair, fat, female, fertile and forty’. Cholecystectomy - the surgical resection and removal, was and continues to be the permanent solution for the condition. There are basically 2 approaches today- i) Open Cholecystectomy and 2) Laparoscopic Cholecystectomy [3].
This review is triggered by an elective laparoscopic Cholecystectomy I witnessed in October 2022, costing INR 250,000, recall of seeing first open cholecystectomy in 1963, literature review of evolution of Cholecystectomy and the current costs across the country in India.
Cholecystectomy is the commonest operation of the biliary tract and is the gold standard for the definitive management of symptomatic cholelithiasis. Carl Langenbuch a German surgeon is credited with pioneering the concept and execution of the first gall bladder extirpation [1].
The first account of gallstones was given in 1420 by a Florentine pathologist Antonio Benevieni, in a woman who died with abdominal pain [1]. The first interaction of gallstones and surgery dates back to 1687 when Stal Pert Von Der Wiel, while operating a patient with purulent peritonitis accidentally found gallstones [2]. The treatment of symptomatic gallstone disease remained primitive and ineffective until the 18th century. Jean-Louis Petit, the founder of gall bladder surgery in 1733 suggested removal of gallstone and drainage of the gall bladder, thus creating fistula in patients with empyema, which he successfully performed in 1743 [2]. Thudichum JLW proposed a two-stage elective cholecystostomy in 1859, In the first stage, the inflamed gall bladder was sewed to the anterior abdominal wall through a small incision, to serve as a route for the removal of gall stone later in the second stage [3]. In July 1867, Dr John Stough Bobbs from Indianapolis, while operating on a patient with suspected ovarian cyst found an inflamed and adhered gall bladder packed with multiple gallstones. He removed the gallstones and left the gall bladder in the abdomen after a cholecystostomy, and the patient recovered and outlived the surgeon.
Marion Simms must be credited with designing, perfecting, and performing the first cholecystostomy on a 45-year-old woman with obstructive jaundice in 1878 [4]. Even though the patient died on the eighth postoperative day due to massive internal haemorrhage, it paved the way for Theodor Kocher to perform the first successful cholecystostomy in June 1878 [1, 4]. It was Carl Johann August Langenbuch found a definite solution for the disease. Langenbuch at the age of 27 was appointed director of the Lazarus hospital in Berlin that allowed him to see many Cholecystitis patients and develop improved the surgical procedure. After developing the technique of cholecystectomy through cadeveric dissection, on July 15, 1882, he successfully removed the gall bladder of a 43-year- old man who was suffering from the disease for 16 years [4]. He had found two gallstones and a chronically inflamed and thickened gall bladder. The patient was discharged uneventfully from the hospital after six weeks. Though initial report appeared in 1882 this new cholecystectomy procedure was debated against the established cholecystostomy.
An audit performed in 1886 showed 39 cholecystostomies with a mortality of 27% as against 8 cholecystectomies with a mortality of 12%. By now Langenbuch cholecystectomy had convinced more and more surgeons worldwide and by 1897nearly 100 operations with a mortality rate of less than 20 per cent were performed [5].
Langenbuch open cholecystectomy remained the gold standard for symptomatic cholelithiasis for over a century with the introduction of operative cholangiography for the detection of common bile duct stone by Mirizzi [6].
Mouret from France performed the first human laparoscopic cholecystectomy in March 1987 as he was completing a gynaecologic laparoscopy on a woman also suffering from symptomatic gallstones, he shifted his laparoscope to the subhepatic area. Upon finding a comparatively free and supple gall bladder he decided to remove it laparoscopically instead of opening, successfully and the patient recovered without complications [7]. In September 1992 a NIH consensus conference held in Bethesda concluded that laparoscopic cholecystectomy was the treatment of choice for gall bladder lithiasis [6]. Current global guidelines also say that the gallbladder should be removed, not because it contains stones, but because it forms them [5, 8].
In a prospective randomized study of 120 patients of cholelithiasis aged between 20 years to 80 years, with one or multiple gallstones diagnosed on ultrasonography, were subjected to open and laparoscopic Cholecystectomy by drawing a lottery. The median (range) operation time for laparoscopic cholecystectomy was 55-155 min (mean=102 min) and 40-105 min (mean=72 min) for open cholecystectomy (p <0.001). Form LC group 5 cases (8.3%) had to be converted to OC. LC was found to be superior to OC, but open cholecystectomy is preferable in complicated cholecystectomy (Table 1 & Figures 1,2).
| Age group (Yrs) | L C | O C | Male | Female | M: F Ratio |
|---|---|---|---|---|---|
| 20-39 | 11 | 13 | 5 | 19 | 1:04 |
| 40-59 | 41 | 36 | 11 | 66 | 1:06 |
| 60-80 | 8 | 11 | 3 | 16 | 1:05 |
| Total | 60 | 60 | 19 | 101 | 01:05.3 |
Table 1: Age and sex distribution of patients.
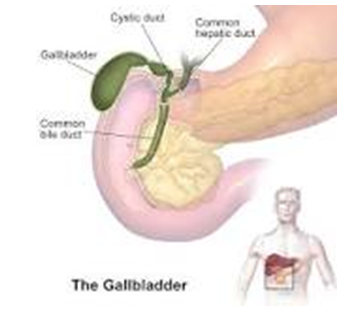
Source: Gallbladder - Wikipediahttps://en.wikipedia.org › wiki. Figure 2: Gallbladder and Ducts.
Indian Scenario
As a medical student the first description of Gallstone disease (GSD) I had heard from our professor of surgery as early 1962 theory class, describing at risk population as five ‘F’s standing for ‘fair, fat, female, fertile and forty’ to have cholelithiasis. In India, the incidence of gall stones is around 6% of the total population, affecting 10% of women as compared to 3% in men. In elderly people, the incidence it sharply increases up to 20% [7] (Figure 3).
Prevalence of gallstone ranges from 10 to 20% in India varying in different states, affecting nearly 4.3% of the total population In India. Gallstone disease (GSD) is most prevalent in northern and north-eastern states of Uttar Pradesh, Bihar, Orissa, West Bengal, and Assam. It is seven times more common in north than south India. The incidence of gallstone disease increases after age of 40 years, and it becomes 4-10 times commoner in old age, affecting 16% and 29% of women above the age of 40-49 years and 50-59 years, respectively [8, 9]. While 40-59 age group contributed
64% of cases 20-39 age group contribute 20% and the rest (16%) were above 60 years. In each age cohort women cases outnumber men (Figure 4).

Case Report
- My niece a young lady of 35 years, with recurrent abdominal pain since adolescence, was referred by a general practitioner and goes for an Ultrasonography (USG) in Bengaluru on 31 October 2022. The MRI report read 1. Grade 1 Hepatic Fatty Infiltration 2. Cholecystolithiasis & dilated common bile duct (CBD), central intrahepatic biliary radical dilatation due to distal CBD calculi.
- On 03/11/22 Endoscopic retrograde cholangiopancreatography (ERCP), a procedure to diagnose and treat problems in the liver, gallbladder, bile ducts, and pancreas was done, after basic investigations like FBS (120), PPBS (160), HBA1c ((6.9),TC &DC (normal range) Serum Cholesterol (205), Triglycerides prothrombin time (14.5 Sec), HBASG, HCAVG (both Negative), It combined X-ray and the use of an endoscope a long, flexible, lighted tube to treatment of pancreatic ducts by placing stents. The findings included bulky Papilla; selective CBD cannulation was done after pre- cut papillotomy. Cholangiogram showed a dilated CBD measuring 12 mm with lucent filling defect measuring 10mm in the lower GBD. GB was not opacified, IHBR was mildly dilated. Cholelithiasis involves the presence of gallstones- concretions that form in the biliary tract, usually in the gallbladder. Choledocholithiasis refers to the presence of one or more gallstones in the common bile duct (CBD).
- Over the wire sphincterotomy and balloon retrieval of yellow pigmented calculus done. Placed 7 cm ErDPT, PVC stent and good bile flow noted. Patient had some discomfort when swallowing for 2-3 days after an ERCP. A bit of bloating was also experienced mainly due to the air that we put into your stomach during the procedure. Since there were multiple GB stones of various sizes, no attempt was made to remove. Usually stones up to 12 mm can be easily removed by ERCP. As stones, larger than 12 mm require additional procedure like mechanical lithotripsy or Post Sphincterotomy Balloon Sphincteroplasty (PSBS) a surgeon’s intervention was advised. The whole procedure costing about INR 130,000 and advised cholecystectomy by a gastroenterologist.
- An USG of abdomen on 07/10/22 showed 1 Hepatic Fatty Infiltration, 2. Cholelithiasis with CBD stent in situ, 3. Low place IUCD and Left lateral wall subcostal uterine fibroid
- A week later she underwent laparoscopic cholecystectomy. She was admitted previous evening and put on light diet overnight and empty stomach on the day.
The Surgery Procedure Steps Included
- First the patient was inducted and put on general anaesthesia.
- Surgeons made 4 small incisions on the patient’s abdomen, and then inflated the abdomen for easy viewing and insert the laparoscope through one of the incisions along with other surgical tools needed to properly remove the gallbladder.
- The laparoscope is a lighted instrument with a video camera attached so provide a magnified view of the patient’s internal organs.
- The surgeon searched the common bile duct and detected multiple gallstones lodged there.
- Using a special scoop, he removed those gallstones.
- Clipping of the cystic duct and cystic artery was achieved from 10 mm epigastric port, the gall bladder was resected, and extracted from umbilical port.
- An entire cholecystectomy procedure took about 1 hour.
- She was kept hospitalized for 24 hrs, fluids were given in the evening orally, and semi-solid food introduced next morning.
- She was discharged next evening with an advice of normal activities to be resumed after 10 days of the surgery and no special diet was advised once the gallbladder is removed.
- Care of the incisions: The incisions were covered with tape. Was asked to keep the tape clean and dry and if the tape falls off at home, leave it. Look at the incisions each day, it should be a dry and closed. Stitches in the incisions, were taken out on day 5 after the surgery. The usual time off work is 2 weeks, depending on the type of work patient does.
- After 2/3 months she is advised to go back to Gastroenterologist to get the stent removed. A repeat ERCP at the time of biliary stent removal is commonly performed to confirm closure of the leak and to exclude other pathology. Plastic biliary stents are commonly placed during endoscopic retrograde cholangiopancreatography (ERCP) and should be removed or replaced within 3 months to reduce the risk of stent obstruction.
- A basket catheter, snare, balloon catheter, grasping forceps, stent retriever, and other tools are used, and the procedure done under sedation. This would cost another INR 50,000.
- Post-cholecystectomy dilatation of the bile duct occurs slightly in most cases and some cases may show more than 3 mm dilatation over baseline. Asymptomatic bile duct dilatation of up to 10 mm can be considered as normal range in patients after cholecystectomy.
Open Cholecystectomy (A Recall Memory 1963)
The first open cholecystectomy I saw in 1963, during my first surgical clinical posting. That was an emergency cholecystectomy, as the patient was admitted with acute abdominal pain, signs of extensive inflammation (rigid abdomen), X-ray revealing, retained bile duct stones. Other conditions require open cholecystectomy are adhesions, anatomical variances, bile duct injury, and uncontrolled bleeding for an open procedure. Pre-Operative Preparation: Prior to the cholecystectomy, our professor had asked me and another colleague to follow -up full pre-operative assessment to check patient’s pulse, blood pressure and arrange blood tests for grouping, cross matching, Total and differential cell counts, bleeding time and clotting time and an ECG and X-ray of the abdomen. Preparing for Surgery: The Intern had Stopped drinking and eating for 6 hours before the time of surgery. After a thorough cleaning and shaving the abdomen area to be operated on and again a chemical cleansing was done. Anaesthesia: General Anaesthesia was used and one of the assistant professors of Anaesthesia department had induced anaesthesia using open ether drops and then maintained by ethyl chloride. The patient was placed supine, with arms extended, before induction. Anaesthesia provided adequate muscle relaxation for the surgery. The Equipment Used: The equipment used for the surgery included instruments like Kelly clamps, Kocher forceps, needle holders, scissors, clips, suctions, knife/knife handles, forceps, retractors, right-angle clamps, Kitner dissectors, and electrosurgical devices. The Surgical Procedure: In the actual surgical procedure, I had seen the surgeon (our professor & head of the unit) makes a 6-inch (15-centimeter) incision on patients’ abdomen below your ribs on the right side. The muscle and tissue were pulled back to reveal liver and gallbladder. He had applied two surgical clips (made of sterile titanium) each to the proximal artery and distal duct and one clip to the portion of each structure which will be removed with the gallbladder. He then freed up and secured cystic duct and artery, separated the gallbladder from liver, and removed it. The incision was closed in two running layers using a no 1 PDS suture. The first layer included the peritoneum, transversus abdominis, and internal oblique laterally, and posterior rectus sheath medially and the second layer included the external oblique laterally and anterior rectus sheath medially. The surgery had lasted for nearly 2 hours. post -surgery recovery had taken about 4 hours. Post-Operative Care: The patient was on complete rest for the first 24 hours. After he was made to get up and walk as often as possible. Being active helped recover fast. He was discharged after one week with some advice for normal diet- bland, low-fat foods like plain rice, broiled chicken, toast, and yogurt but to avoid fatty foods like whole milk, cheese, and oily snacks for about one month.
Discussions
Cholesterol stones are formed in the gallbladder because of altered hepatocellular and gallbladder function. Hepatocellular factors include excretion of more cholesterol, too much bilirubin, or not enough bile salts by liver to dissolve. Gallbladder factors promoting stone formation include hypomotility and the secretion of nucleating factor- glycoprotein, mediated by an increase in the prostaglandin production by the gallbladder mucosa [2].
Cholecystectomy is one of the commonest elective surgical procedures performed, to address symptoms related to biliary colic from cholelithiasis, to treat complications of gallstones (acute cholecystitis, biliary pancreatitis), or as incidental cholecystectomies performed during other open abdominal procedures in India [7]. The widespread use of diagnostic abdominal ultrasonography has led to the increased detection of clinically unsuspected gallstones, resulting in controversy regarding the optimal management of asymptomatic (silent) gallstones. Biliary colic with sonographically identifiable stones is the most common indication for elective cholecystectomy. Cholecystectomy is not indicated in most patients with asymptomatic stones because only 2-3% of these patients go on to become symptomatic per year. Patients who are immunocompromised, are awaiting organ allotransplantation, or have sickle cell disease are at higher risks of developing complications are operated irrespective of the presence or absence of symptoms. Additional indications recommended include , a) Calculi >3 cm in diameter, in geographical regions with a high prevalence of gallbladder cancer b) Chronically obliterated cystic duct c) Non-functioning gallbladder d) Calcified gallbladder e) Gallbladder polyp >10 mm or showing a rapid increase in size f) Gallbladder trauma g) Anomalous junction of the pancreatic and biliary ducts h) Morbid obesity is associated with a high prevalence of cholecystopathy, as the risk of developing cholelithiasis is increased during rapid weight loss. Choice of the Surgery: Open cholecystectomy was the gold standard for over 100 years. Laparoscopic cholecystectomy, introduced in the 1980s is the preferred choice now. If the procedure is expected to be straightforward, laparoscopic cholecystectomy is preferred [9].
Laparoscopic and open cholecystectomy seem equivalent considering complications and operative time, but laparoscopic cholecystectomy is associated with quicker recovery. The classical open cholecystectomy and the minimally invasive laparoscopic cholecystectomy are two alternative operations for removal of the gallbladder. There are no significant differences in mortality and complications between the laparoscopic and the open techniques. The laparoscopic operation has advantages over the open operation regarding duration of hospital stay and convalescence [10, 11, 12].
Laparoscopic cholecystectomy (LC) since its inception in 1989 has become the gold standard treatment for gall stone disease. Most gallbladder surgeries today are done using laparoscopic surgical techniques, in which narrow instruments, including a camera, are introduced into the abdomen through small puncture holes. It is done by making 4 small incisions (cuts), 2.5 cm (1/2 inch) or less, in abdomen [8, 12].
- The more traditional retrograde (“top-down”) approach in our student day used to starts with dissection at the gallbladder fundus and proceeds toward the portal triad and the triangle of Calot. This strategy facilitated for sure identification of the cystic duct and artery, the two attachments to the gallbladder.
- Anterograde approach (Bottom approach): With increased experience and expertise in the laparoscopic technique, surgeons often prefer the anterograde approach, in which dissection begins at the triangle of Calot with dissection and ligation of the cystic artery and duct. This is followed by dissection of the gallbladder from the liver bed, starting usually from the infundibulum up. Dissection from the fundus down can also be done.
Patients are admitted a day prior to surgery in case of elective cholecystectomy. Some patients are admitted from emergency department of hospital as they had presented with acute abdominal pain. A detailed clinical history was taken from all patients. Physical examination is done with the help of a common proforma. Full range of investigations like chest X-ray, ECG, CBC (Complete Blood Count), LFT (Liver Function Test), KFT (Kidney Function Test), serum electrolytes and viral markers were done on all patients. Medical and anaesthetic fitness were assessed preop. Gas and relaxant general anaesthesia are used.
Standard Laparoscopic Cholecystectomy
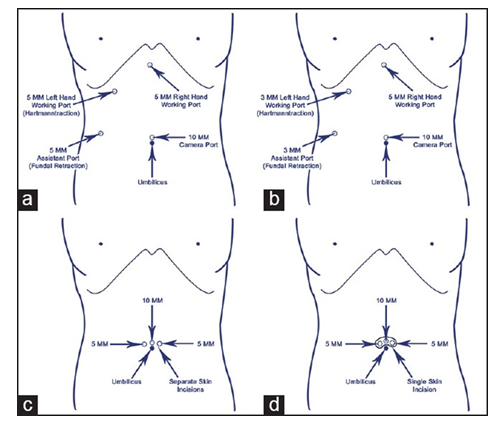
The standard technique of performing LC is to use 4 ports. The pneumoperitoneum is achieved by either closed Veress needle technique or open technique using a blunt trocar or a Hasson’s trocar. A 10 mm telescope usually a 30 degree is used at the umbilicus either infra, intra or supraumbilical depending on patient’s habitus and surgeon’s preference. Another 10 mm trocar is used in the epigastrium which is the main right working port for the surgeon. One 5 mm trocar in the right lumbar region is used for gallbladder fundus traction and another 5 mm trocar in the right hypochondrium is used as left-hand working port for the surgeon. With left hand Hartmann’s pouch is retracted and with right hand anterior and posterior dissection is done in Calot’s triangle and wide window is created. Critical view of safety is of utmost importance to prevent bile duct injury. Clipping of the cystic duct and cystic artery is achieved from 10 mm epigastric port. Gallbladder extraction is generally done from either epigastric or umbilical port. This technique can be named as “10-10-5-5” or “4 ports standard LC”. “10- 10-5-5” denotes 10 mm umbilical port for camera, 10 mm epigastric port for right working instrument, 5 mm right hypochondrium port for left working instrument and 5 mm right lumber port for fundal retraction respectively.
Recently several surgeons have been using more and more modified techniques to make the operation more minimally invasive and to inflict lesser postoperative pain and better cosmesis. The modifications may be either reduced port size, i.e., from 10 mm to 5 mm or from 5 mm to 3 or 2 mm or reduced port numbers. There are various techniques like trans-gastric, transvaginal, and trans-colonic approaches also [9].
Single Site Laparoscopic Cholecystectomy (SSLC) or Trans-Umbilical Single Site Surgery (TUSS)
In the last 3 to 4 years, the single incision laparoscopic surgery (SILS) through the umbilicus. SSLC includes single skin and sheath incision or single skin and separate sheath incisions or separate skin and sheath incisions but at the same site. One of the port devices such as SILS port (Covedien), Tri port or Quad port (Olympus) or X cone (Storz) through the single incision. However, this incision typically requires a larger skin incision of at least 20 mm [9].
Hybrid Laparoscopic Cholecystectomy
In the hybrid technique three trocars are placed into the umbilicus whereas; one trocar which is the active dissection trocar is placed into the epigastrium lower down and more on the left side. This trocar is placed under direct vision of the first trocar and then the other two 5 mm trocars are also placed under direct vision with the telescope from this trocar. With this technique “10/5/5-5” or “5/5/5-5”, advantages of both single incision and multiport are gained and the surgery can be expeditiously completed [9].
Cost of Cholecystectomy in India
On average, the cost of Gallstone removal surgery in India will be somewhere in between Rs. 45,000 to Rs. 1,00,000 for open surgery and Rs. 80,000 to Rs. 1,60,000 for laparoscopic cholecystectomy surgery (LCS) in cities like Mumbai, Bengaluru, Delhi, Kolkata, New Delhi, and other towns [13]. However, the final cost will depend on a variety of factors such as type of surgery, surgical care required, etc with an average cost of 95,000 for LCS [13]. Compared to this the Govt. Of India provides INR 10,000, for laparoscopic Cholecystostomy and 22,800 for Cholecystectomy open or Laparoscopic in Ayushman Bharat Package [14].
Public Health Importance
If 10% of the adult population suffers from Cholelithiasis in a country and a conservative 2% of them needing Cholecystectomy, the annual burden and expenditure is huge. For example, in India with an estimated total population (the World Population Prospects 2022) of 1.428 billion and 808 million adult population as on July 1, 2023, 81 million adults will suffer from Cholelithiasis and among them 1.6 million would need surgery annually.
Cholecystectomy & its Effect
One can lead a perfectly normal life without a gallbladder. Our liver will still make enough bile to digest your food, but instead of being stored in the gallbladder, it drips continuously into digestive system. It may be harder and take longer for your body to digest fat. However, large amounts of fatty, greasy, or high-fiber food become harder to digest. The Post- surgery one may experience temporary side effects related to the way your digestive system processes fatty foods. These symptoms may include loose stools or diarrhoea, bloating, cramping, and excess gas in response to meals or certain foods. The larger amounts of bile reaching the colon may cause irritation resulting in diarrhoea with a yellow hue. The increased amounts of bile salt can also make one’s bowel movements have a more potent smell as well.
Removing the gallbladder will stop the pain and treat the infection caused by gallstones. It stops gallstones from coming back. Long-term effects of gallbladder removal include diarrhoea, fatty food intolerance, gas, heartburn, nausea, vomiting, jaundice, and intermittent episodes of abdominal pain. Symptoms of post-cholecystectomy syndrome typically begin in the postoperative period but can also begin months or years after surgery.
Cholecystectomy patients must get used to drink plenty of water, broth, and sports drinks. Avoid alcohol for at least 2 days after your surgery. Consume Low-fat foods as they will be easier for you to digest and are less likely to cause gas, bloating, or diarrhoea.
Way Forwards
- The expert committee that decided the Ayushman Bharat package, fixed the cost of Laparoscopic / open cholecystectomy charges at INR 22,000, in December 2022, need to review and fix a realistic all-inclusive cost.
- As a recent survey across India among around 1,800 people in the age group of 18-35, showed the incidence of health insurance of 35% population registration under Ayushman Bharat should reach the expected 50 million by end of 2024.
- The author feels that Lap. cholecystectomy surgery be made available in the public sector in all district hospitals over next 2 years to minimize the expenditure.
- Ayushman Bharat need to negotiate with recognized private facilities for this surgery with an upper limit of INR 100,000 until district hospital can provide the facility.
- Reassure the people that they can lead a perfectly normal life without a gallbladder.
- It may just be a bit harder and take longer time for the body to digest fat.
References
-
Shehadi WH (1979) The biliary system through the ages. Int Surg 64(6): 63-78.
-
Bouchier IA (1992) The formation of gallstones. Keio J Med 41(1): 1-5.
-
Beal JM (1984) Historical perspective of gall stone disease. Surg Gynecol Obstet 158(2): 181-189.
-
Utpal DE (2004) Evolution of cholecystectomy: A tribute to Carl August Langenbuch. Indian J Surg 66(2): 97-100.
-
Karam J, Roslyn JR (1997) Cholelithiasis and cholecystectomy. Maingot’s Abdominal Operations. 12th (Edn.), Prentice Hall International Inc, pp: 1717-1738.
-
Servetus M (1989) Christianismi Restitutio and Other Writings. Birmingham, the Classics of Medicine Library, Philadelphia, USA, pp: 1511-1553.
-
Mirizzi PL (1938) Operative cholangiography Its Contribution To The Physio-Pathology Of The Common Bile-Duct. Lancet 2(5998): 366-369.
-
Hina Zahid (2021) Cholecystectomy: Govt. of India Standard Treatment Guidelines.
-
Haribhakti SP, Mistry JH (2015) Techniques of laparoscopic cholecystectomy: Nomenclature and selection. J Minim Access Surg 11(2): 113-118.
-
Doke A, Ninad G, Jayant G, Niranjan D, Santosh U, et al. (2016) A comparative study between open versus laparoscopic cholecystectomy. Sch J App Med Sci 4(1): 57-61.
-
Keus F, Jong J, Gooszen HG, Laarhoven CJHM (2006) Laparoscopic versus open cholecystectomy for patients with symptomatic cholecystolithiasis. Cochrane Database of Systematic Reviews 4: 1465-1858.
-
Ranjan R Kishore KS, Mahesh C (2018) A comparative study of laparoscopic (LC) vs. open cholecystectomy (OC) in a medical school of Bihar, India. Int J Adv Med 5(6): 1412-1416,
-
Medifee Gallbladder Stone Surgery Cost in India.
-
(2023) Ayushman Bharat Covered Diseases.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda