Evaluating Enrollee Perceived Benefit of the Contributory Scheme Post Implementation in Katsina State Contributory Scheme North-West of Nigeria
Background: The Katsina State Contributory Health Care Management Agency (KTSCHMA) is visualized as one of the single most powerful social security interventions in the State’s effort geared toward the attainment of Universal Health Coverage (UHC). The Agency is designed to provide a cost-effective comprehensive healthcare delivery system for employees of formal sectors, self-employed, poor, and vulnerable groups. This study was conducted to assess the perceived benefit, problems and suggested ways of improving the scheme among civil servants in Katsina state, Nigeria. Methods: The study was a cross-sectional study conducted among 393 state civil servants. Participants were selected using a multistage sampling technique and data was obtained using a structured questionnaire. Data were analyzed with SPSS version 2.5 to obtain frequencies, means, and standard deviation. Results: The majority 53.8% of the respondents had reported reduced out-of-pocket expenditure as the major perceived benefit of the scheme, 20.9% easy access to healthcare service delivery, 13.2% availability of quality drugs, 9.3% affordable healthcare delivery, 2.6% short waiting time and 0.2% reported the benefit of the scheme is to achieve universal health coverage. Regarding the scheme perceived problems, almost half 50.5% of the respondents indicated the unavailability of most prescribed drugs as the main problem, and the majority 54.4% reported regular monitoring of the scheme operations by the Agency as the main way of improving the scheme. Conclusions: Reducing out-of-pocket expenditure and easy access to qualitative healthcare service delivery is the main enrollee perceived benefit of the scheme and the finding in this study show the high level of out-of-stock of prescribed drugs. Major suggestions proffered by enrolees for improving the scheme covered were regular monitoring of Healthcare Providers, provision of drugs and consumables, sensitization workshops on the modus operandi of the scheme, prompt response to enrollee complaints, and continuous review of the policy.
Introduction
The Katsina State Contributory Healthcare Management Agency (KTSCHMA) was established in Katsina in 2018 as part of the health systems reform to improve health services [1]. The Scheme offers Formal and Informal sector program, the Formal Sector Program comprises all elected and political appointees of State and Local Government, Public Sector Employees (State, Local Government, and SUBEB), Organized Private Sector (OPS) for organizations with a minimum of five (5) staff, Tertiary Institution Contributory Health Program (TICHP), and Retirees. For the informal sector, it includes the Basic Healthcare Provision Fund Program (BHCPF), Community Based Contributory Health Scheme (CBCHS), Vital (Voluntary) Contributory Program (VCP), Urban Self Employed (USE). The main purpose for the establishment of the scheme was to facilitate fair financing of healthcare cost through a credible and sustainable pooling mechanism and judicious utilization of financial resources to provide sustainable and efficient financial risk protections and cost-burden sharing for people against high cost of healthcare through various prepayment mechanisms prior to the falling ill. Formal sector program to informal sector program, defined mainly by the source of financing for the premium [1]. Effective implementation of these programs will enable the State and the country achieve a high coverage of the population as obtained in some countries such as Colombia, with 95% coverage and Thailand with very few citizens without insurance coverage [2], While according to the household baseline assessment conducted by the Agency for the implementation of the scheme shows that only 2.5% of the federal civil servants were covered by the National Health Insurance Authority in the state and 0.3% of the State civil servant was covered by other form of contribution health scheme like community based health insurance scheme, a remarkable number (87%) of State Civil servants within one year of its implementation recorded under the scheme at the time of this survey. The scheme has an overall goal of achieving universal health coverage which ensures access to and use of quality health care services by all resident of Katsina State, and protection from catastrophic financial effect of ill-health [1]. However, out-of-pocket health expenses, as high as 99.3%, as of 2010, as shown by the KTSCHMA [3]. The contributions to the scheme are earnings-related for state civil servants. The employee pays 2.5% of the consolidated salary deductible at source, for the organized private sector, the employer pays 10%, while the employee pays 5% representing 15% of the employee’s monthly basic salary collective of which shall not be less than N5, 000. However, the employer/employee may decide to pay the entire contribution. For students, (TICHP) payment of contribution shall be per academic session at the rate of Two Thousand Naira (N2, 000.00) only subject to review by the Agency. For Retirees, contribution rates are to be determined by the Agency after due consultation with relevant stakeholders [1]. There shall be a processing/ waiting period of 90days (3 months) before an enrolee can access healthcare services.
The Contributions for formal sector program cover an employee, a spouse and four (4) biological children below the age of 18 years. Principals are entitled to register a maximum of Four (4) extra dependents, upon payment of N9, 000 only per annum per additional dependent subject to review by the Agency. The extra dependent has to be a wife, biological parents or biological children below the age of 18 years. Birth certificate of biological children must be provided at the point of registration for authentication. Multiple registration and that of an ineligible dependents/spouse is a criminal offence punishable by law. The beneficiary has the right and privileges to: Freely choose his/her NHIS/KTSCHMA accredited primary healthcare facility (ies) that registered with the Agency. Change primary healthcare facility after six (6) months with the present primary health care facility. Access care once his/her name is on the current Agency’s enrollee register after proper identification. Treatment at the nearest NHIS/KTSCHMA accredited healthcare facility registered by the Agency in case of emergency. Add or remove dependent(s) subject to approval by the Agency. Add extra dependent(s) on payment of a fee. Enrollees had several reasons for choosing a healthcare facility.
The findings in KTSCHMA baseline survey showed that 51.5% of the respondents chose the hospital because of the expectation of excellent services (quality of care), 23.2% affordability and 10.6% selected it on account of easy accessibility. Similarly, another study by Osungbade, et al. [4] approached this through assessment of staff attitude, waiting time and consultation process, highlighting the importance of enrolee’s perceptions in assessing the insurance schemes. Enrolees’ satisfaction with the services provided by health insurance schemes has been shown in Ghana in a study conducted by Fenny, et al. [5] and in Ibadan south west Nigeria by Adebayo, et al. [6] to constitute one of the key factors for sustaining the scheme and for expansion. Women
accessing health services from Primary Health Care facilities in Nnewi, Nigeria expressed high level of satisfaction with the quality of maternal services [7]. A well implemented health insurance scheme should transform lives especially of the poor, by enabling access to previously unaffordable medical treatment and good quality health care. Given the dearth of literature from north-west Nigeria on clients’ perceived benefit with health contributory scheme, recording enrolees experience and their identified problems should enable improvement for effective implementation. Against this background, this study sought to generate evidence to improve the functioning of the Katsina State contributory scheme in Nigeria. It assessed civil servant (enrollees’) perceived benefit, problems, and their proffered suggestions for improvement. It addressed the following research questions; what are the enrolees perceived benefit? What are the problems perceived under the scheme? And What are enrolees’ suggestions for improving the scheme? Findings from the study would generate some evidence on KTSCHMA achievements on some of its set goals of reducing out-of- pocket expenses (OPE) and meeting enrolees’ expectations.
Methods
Study Area
The study covered 170 accredited healthcare providers comprises 20 public secondary providers, 29 private and 121 public primary health centres under formal sector program of the Katsina State Contributory Healthcare Scheme. all located in Katsina, North- West, Nigeria. Katsina is located on latitude 120 59’ N and longitude 70 36’ E. The city of Katsina is the administrative capital of Katsina state, Nigeria. The main town is situated about 400 kilometres east of Sokoto 160 kilometres northwest of Kano, 300 kilometres north of Kaduna, 460 kilometres north of Abuja Federal capital, and about 90 kilometres southeast of Maradi in Niger Republic. It covers an area of about 24,192sqkm (9341 sq. miles). The scheme has 170 accredited healthcare providers, of which 20 are public secondary providers, 29 private and 121 public primary health centres, and an enrolment of 278,254 (87%) of the expected target during this survey. The coordination of the entire system rests on the Katsina State Contributory Healthcare Management Agency.
Study Design
This was a descriptive, cross-sectional study that focused on healthcare providers in Katsina State. Quantitative data were collected using semi-structured questionnaire designed to probe into benefit, problems and their proffered suggestions for improvement of Katsina State Contributory Scheme.
Study Population
A cross-sectional study was conducted among the enrollees of the scheme from 1st October to 30th November, 2022. The population for this study was all beneficiaries of the formal sector program that was registered with the Agency. The total population of the registered enrollees was 280,370 based on data obtained from the Agency Dashboard. Only enrollees in formal sector program registered by the Agency and who have received healthcare for at least one visit were considered eligible. We excluded Informal Sector program.
Sample Size Estimation and Sampling Technique
The sample size was estimated at 393 enrollees’ this is in line with the formula according to Ibrahim, et al. [8] for cross section descriptive study as;
2
2 Z pq n d =
Where n = Minimum Sample size z = Standard normal deviate at 95% confidence interval= 1.96 p = Study by Nwanaji et al, 2022 on patient satisfaction with the Nigerian National Health Insurance Scheme two decades since establishment from (2011 to 2020) found that moderate overall satisfaction with the NHIS (64%) from respondents. q = q= 1-P (1-0.64) = 0.36 d = Precision expected at 95% confidence limit (0.05) precision of tolerable alpha Error. n= (1.96)2 x (0.64) x (0.36) / (0.05)2 0.885/0.0025 Therefore n= 354 Allowing for 10% non-respondent rate the Optimum sample size will be n/RR (Ibrahim, 2009) where n=353, RR=90% (0.9) this gives 354/0.9= 393
Sample and Sampling Technique
The sample of the study was 393 enrollees’ this is in line with the formula according to Ibrahim, et al. [9] for cross section descriptive study and to select 393 study participants from the 46,650 enrollees that have access care the following sampling techniques were deployed.
Step 1: Selection of utilization register from July 2021 to September, 2022 using simple random sampling techniques and September 2022 register was selected comprised of
46,650 (17%, utilization rate) enrolee that have access care in the reporting month.
Step 2: Selection of number of respondents from each healthcare providers using proportional allocation first as sample frame, examples; to select 16 from the 1944 enrolee that have access care in CHC Bakori, proportional allocation was used to select the study respondents (sample unit) from the sample frame as follows;
Number of enrollees that haveaccess services Total number of enrollees that haveaccess service sample i e s s z ′ × ′ For example: using CHC Bakori where 1944 enrollees’ access services
1944 393 46,650 × This means 16 enrolees were enrolled from the CHC Bakori.
This was repeated for all the healthcare providers to give the number of study respondents to be interviewed from each healthcare providers, Step 3: Systematic sampling was used to select the study subject, using procedure of systematic random sampling.
Data Collection Instrument
The instrument used for data collection was a set of structured pre-tested questionnaires. The questionnaire consists of four sections; section A sought information on socio-demographic characteristics of respondents; section B consists of enrolees perceived benefit of the scheme, section C consist of enrolees identified problems and section D consists of enrolee proffered suggestions for improvement of the scheme.
Validation of the Instrument
The research instrument was validated by two jurors of experts in public health who validated the face and content validity of the instrument all observations, suggestions, corrections, and comments of the expert was incorporated in the final draft of the questionnaire to the satisfaction of the research team before pilot study.
Data Collection Procedure
The research proposal was presented to the Ethical Research Committee of Katsina State Ministry of Health for ethical approval with reference number MOH/ADM/ SUB/1152/1/655; then to the Organized Labor Union, SPHCA, and HSMB for approval to conduct the study in the facility. Then to the healthcare providers for noting of using their facility enrolees, 20 research assistants were recruited to assist in administering the research instrument.
Data Analysis
The data obtained from the questionnaire will be coded and entered into the computer for data cleaning and analysis, using the Statistical Package for Social Scientists (IBM SPSS) version 23 and Microsoft Excel 2016. Frequency count and percentage were used to organize and describe the demographic characteristics of the respondents, benefit, problems and their proffered suggestions for improvement.
Results
Out of the 393, enrolees included in this study 364 of them returned their questionnaire giving response rate of 93%. Other demographic details of the respondents are summarized in Table 1 below.
Demographic Profile of Respondents
| Demographic profile | Frequency | Percentage |
|---|---|---|
| Gender | ||
| Male | 164 | 45.1 |
| Female | 200 | 54.9 |
| Level of Education | ||
| Primary | 48 | 13.2 |
| Secondary | 60 | 16.5 |
| Tertiary | 256 | 70.3 |
Table 1: ** Socio-demographic profile of the respondents (n=364).
Source: Survey, 2022 Table 1: Socio-demographic profile of the respondents (n=364).
Table 1 Show that 54.9% of the respondents are female and 45.1% of the respondents are male. 70.3% of the respondents are having tertiary education (Bachelor’s or Master’s Degree), 16.5% have a secondary qualification, and 13.2 primary qualifications, which means about 70% of respondents have higher education, which means the majority of the respondents have access cares have a higher educational level. The ultimate effect is that our research has a certain level of very accurate responses as this part of the respondents understood the survey question clearly and responded accurately.
Enrolees Perceived Benefits from the Scheme
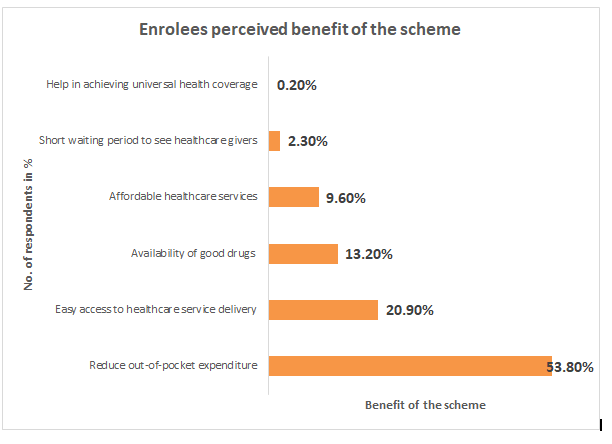
- Figure 1 above shows that; reduce out-of-pocket expenditure was the most mentioned benefit derived from the scheme (53.8%), easy access to healthcare service delivery 20.9%, availability of good drugs (13.2%), affordable
- Enrolees Perceived Problems from the Scheme
- Perceived problems of the scheme n (364)
- Most drugs not available
- 184
- 50.5
- Low quality products/drugs
- 35
- 9.6
- Time spent to see a doctor/health care giver
- 28
- 7.7
- Exclusion of some drugs
- 28
- 7.7
- Facility is closed always I attended the facility
- 20
- 5.5
- ID card not ready
- 16
- 4.4
- Poor staff attitude
- 14
- 3.8
- No place to complaint
- 12
- 3.3
- Enrollment update difficult to access
- 8
- 2.2
- Delay in having authorization code for referral
- 8
- 2.2
- We still paid for expensive drugs and test
- 7
- 1.9
- Children above 18 years do not benefit into the scheme
- 4
- 1.1
Table 2: Enrolees Perceived Problems from the Scheme.
Table 2 above shows that more than half 50.5% of the respondents expressed a high level of problem with the pharmacy services and 9.6% reporting low-quality drugs under the scheme. The high level of dissatisfaction and problem with the pharmacy services may be attributed to pharmacy staff attitude and the timeliness of receiving the drugs from the Drugs and Medical Supply Agencies (DMSA).
Respondents Suggested ways of Improving the Scheme
Suggested ways of improving the scheme n (364)
Frequency Percentage (%)
Regular monitoring of the scheme’s operations by regulator 198 54.4
Availability of genuine drugs 84 23.1
Continuous review of the scheme’s guidelines 36 9.9
Improve human resource in the facility 22 6
Prompt response to enrollees’ complaints 14 3.8
Provision of quality healthcare services 10 2.7
Source: Survey, 2022 Table 3: Respondents suggested ways of improving the scheme.
Table 3 Above shows enrolees enrolee proffered suggestions for improvement of the scheme of which majority 54.4% reported regular monitoring of the scheme operations by the Agency, as the leading proffered method of improving the scheme, Continuous availability of genuine drugs 23.1%, Continuous review of the scheme’s guidelines 9.9%, Improve human resource in the facility 6.0%, prompt response to enrolees’ complaints 3.8% and provision of quality healthcare services were the major issues suggested for improvement of the scheme.
Discussion
The majority of the respondents were females. It suggests that women have better health-seeking behaviour than their male counterparts. A study in the United States suggested that men are less likely to seek help from health professionals for problems more complicated as depression, substance abuse, physical disabilities, and stressful life events than women. Previous research has revealed that the principal health-related issues facing men in the United Kingdom (UK) are related to their reluctance to seek healthcare services [9]. This may probably account for a higher proportion of females than male enrolee-respondents in this study.
The greater proportion of the respondents with a tertiary level of education 256 (70.3%) enrolled in the scheme compared to those with primary education 48 (13.2%); secondary 16.5 (16.5%). A study conducted in Ghana indicated a positive relationship between education and uptake of the NHIS Scheme [10]. This could be attributed to the fact that individuals with tertiary levels of education tend to be more informed of the benefits of the scheme than those with a primary and secondary level of education who may be less aware of the scheme and its benefits.
More than half of the enrollees’ stated that the most important benefit of the scheme was that the contributory scheme saves money and enables them to pay fewer hospital bills. This finding is comparable to that of another study carried out by Ibiwoye, et al. [11] on the impact of health insurance on healthcare provision in developing countries, which showed that the scheme has the potential of reducing out-of-pocket payment at the point of service utilization. Also similar to the finding of Brian, 2016 study on the Evaluation of the Benefits, Quality of Services, and Challenges to the Nigerian National Health Insurance Scheme among Enrolees in a Tertiary Teaching Hospital in Southeast Nigeria [12].
The enrolees in this study identified various problems with the contributory scheme. The majority of them, 198 (50.5%) agreed that most of the drugs were not available during the visit and this is attributed to delay in receiving the drugs from the drugs and medical supply Agency as the main supplies of the essential medicine under the scheme, few reported low quality of the drugs, time spent to see doctors. Other reporters had also shown that issuance of identity cards presented a major barrier to accessing care, exclusion of some drugs from the benefits package, the facility closed in some visits, poor staff attitude, difficulty to undergoes enrolees update. Most of the suggestions given by enrolees for improving the scheme are issues that can be covered through constant monitoring of the healthcare providers (HCPs) and the enrolees’ views on services provided and accessed. Another problem identified regarding the unavailability of most drugs is an administrative problem within the healthcare facility and Agency responsible for supplying the drugs. Regular monitoring of healthcare providers’ activities on the quality of care and efficiency within the scheme as emphasized by the majority of the respondents as their proffered suggestions for improving the scheme this finding is similar to that of Omoruan et al. that shows regular monitoring is critical as one of the ways of improving the scheme. This, according to Lagomarsino et al. will enable enrolees’ utilization of healthcare facilities and uptake of services as well as protect them from impoverishment resulting from health costs.
Conclusion
Katsina State Contributory Scheme has a positive impact on healthcare financing in Katsina. It reduces catastrophic out- of-pocket spending on quality healthcare services. This study reported a reduce out-of-pocket expenditure for healthcare service delivery, and unavailability of some prescribed drugs as the major problems and reported regular monitoring of the scheme operations by the Agency, continuous availability of genuine drugs, continuous review of the scheme’s guidelines, Improve human resource in the facility, prompt response to enrolees’ complaints and provision of quality healthcare services were the major issues suggested for the improvement of the scheme. This scheme has the potential to assist the government in achieving universal health coverage (UHC) targets of the 2030 agenda for sustainable development, under goal 3 (Ensure healthy lives and promote well-being for all at all ages).
References
-
Katsina State Contributory Healthcare Management Agency (KTSCHMA) Law No. 10 of 2018 Katsina State Operational Guideline 2010.
-
Dutta A, Hongoro C (2013) Scaling up national health insurance in Nigeria: Learning from Case Studies of India, Colombia, and Thailand. Futures Group, Health Policy Project. Washington, DC, USA.
-
Household baseline Assessment survey for the implementation of the Katsina State contributory scheme 2020.
-
Osungbade KO, Obembe TA, Oludoyi A (2014) User satisfaction with services provided under National Health Insurance Scheme in South-western Nigeria. Int J Trop Disease & Health 4(5): 595-607.
-
Fenny AP, Enemark U, Asante FA, Hansen KS (2014) Patient satisfaction with primary health care - a comparison between the insured and non-insured under the national health insurance policy in Ghana. Glob J Health Sci 6(4): 9-21.
-
Adebayo AM, Asuzu MC (2015) Utilisation of a community-based health facility in a lowincome urban community in Ibadan, Nigeria. Afr J Prim Health Care Fam Med 7(1): 735.
-
Nnebue CC, Ebenebe UE, Adinma ED, Iyoke CA, Obionu CN, et al. (2014) Clients’ knowledge, perception and satisfaction with quality of maternal health care services at the primary health care level in Nnewi, Nigeria. Niger J Pract 17(5): 594-601.
-
Omoruan AI, Bamidele AP, Phillips OF (2009) Social health insurance and sustainable healthcare reform in Nigeria. Studies on Ethno-Medicine 3(2): 105-110.
-
Galdas PM, Cheater F, Marshall P (2005) Men and health help-seeking behaviour; literature review. J Adv Nurs 49(6): 616-23.
-
Gobah F, Zhang L (2011) The national health insurance scheme in Ghana: Prospects and challenges: A cross- sectional evidence. Global J of Health Sci 3(2): 90-101.
-
Ibiwoye A, Adeleke AA (2007) The impact of health insurance on health care provision in developing countries. Ghana Journal of Development Studies 4(21): 49-58.
-
Akande T, Salaudeen A, Babatunde O (2011) The effects of national health insurance scheme on Utilization of health services at Unilorin Teaching Hospital Staff Clinic, Ilorin, Nigeria. Health Science Journal 5(2): 98-106.
-
Ele GN, Ochu U, Odili VU, Okechukwu RC, Ogbonna BO (2016) Evaluation of the Benefits, Quality of Services and Challenges to the Nigerian National Health Insurance Scheme among Enrollees in a Tertiary Teaching Hospital in Southeast Nigeria, Journal of Advance in medical and pharmaceutical science 9(3): 1-11.
-
Lagomarsino G, Garabrant A, Adyas A, Muga R, Otoo N (2012) Moving towards universal health coverage: Health insurance reforms in nine developing countries in Africa and Asia. Lancet 380(9845): 933-943.
-
Zea NV, Castro H, Páez FR, Tellez D, Arias RS (2012) Colombian health system on its way to improve allocation efficiency-Transition from a Health Sector Reform to the Settlement of an HTA Agency. Value in Health Reg 1(2): 218-222.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda