PROMs in Total Hip Arthroplasty: A Comparison between Robotic Mako Assisted Versus Manual Technique
Study Purpose: The purpose of this observational study is to evaluate the degree of satisfaction and improvement in quality of life through PROMs (Patient Related Outcome Measures), which were administered to patients who underwent Total Hip Arthroplasty (THA) by robotic-arm assisted technique (RIO®, MAKO Surgical Corporation). These data were then compared to a sample of patients operated on by standard manual technique. Both groups were operated on by the same surgical team, in the same hospital, and were subjected to the same recommendation and rehabilitation protocols. Surgeries were performed from November 2017 to March 2019 at a hospital in Asl Toscana Sudest. Endpoint of our study is to verify the rate of improvement – which is assumed to be stable one year after surgery – and how the satisfaction rate increases over time. Another aim is to determine – through the use of Forgotten Joint Score questionnaires and the satisfaction scale – whether there is a difference between arthroplasty operated on by standard manual technique vs robotic-assisted method one year after surgery. Method: Patients who undergone robotic-assisted surgery were evaluated before surgery, at discharge, 1, 4 and 12 months after surgery. 70 robotic-assisted THA patients were studied for a whole year, while 31 standard-technique THA patients were evaluated only 12 months after surgery. PROMs post-surgical evaluations occurred during follow-up visits by orthopedists and physiotherapists. Harris Hip Score (HHs), Oxford Hip score (OHS), EQol VAS (Dimension Visual Analogue Scale), LiKert satisfaction scales were used. Likert scale was administered only 4 and 12 months after (no significant results before this time). The Forgotten Joint Scale (FJS) and the satisfaction scale were administered 1 year after surgery both in robotic-assisted and standard manual THA patients (70 robotic-assisted THA vs 31 standard THA). They were operated on in the same period by the same surgical team, with the presence of a senior surgeon, and were subjected to the same rehabilitation protocols by the same team of physiotherapists.Results: 70 robotic-assisted THA were analyzed (30 l, 40r), with a mean age of 63, 76 years. The average hospital stay in acute care settings was 3.07 days. 40 patients then continued in the rehabilitation department after discharge for further 2.98 days. HHs scale gave a value of 54, 94±14, 71 before surgery and 98, 63±2, 54 one year after surgery. OHS scale reported a value of 21, 27±9, 24 before surgery and 47±2, 06 one year after surgery. The EqolVas scale had a value of 56, 23±20, 04 before surgery and 81, 25±15, 84 one year after. 4 months after surgery, the satisfaction rate was 4, 67±0, 61 and 12 months later was 4, 77±0, 54. The FJS scale in 70 robotic-operated patients had a value of 86, 24±21, 1 and it has been compared to a group of 31 standard-operated patients, whose values were 87, 02±16, 57 and P=0,86. 12 months after surgery, the satisfaction rate for robotic-operated patients was 4, 77±0, 54 and 4, 47±0, 83 and P<0, 05 for standard-operated patients, thus statistically significant. Conclusion: Patients undergoing hip arthroplasty surgery all have a high level of expectations and clinical outcomes are very satisfactory, while knee replacements have more limitations and less appreciable results. Some studies regarding THA report more favorable short-to-medium-term outcomes, fewer transfusions, and fewer days of hospital stay by the use of the roboticassisted technique, when compared to the standard manual surgery. Differences in function and quality of life after 1 year from the two types of surgery tend to decrease, although in our study the satisfaction rate of the robotic-assisted surgeries was statistically significant compared to the standard manual technique. Furthermore, it has been noticed that the rate of functional improvement, well-being, satisfaction and quality of life increases over time after surgery. At the first year of follow-up, no statistically significant differences are shown between the robotic-assisted and standard sample concerning the FJS scale.
Introduction
Total hip arthroplasty is one of the most successful orthopedic interventions and, because of this, it has been called the surgery of the century [1]. The number of arthroplasty surgeries has significantly grown in recent decades, and the trend is that it will progressively increase. Population growth, progressive aging of the population, and the increased functional demand due to young patients with osteoarthritis and early necrosis will lead to an exponential increase in the demand for hip arthroplasty. The popularity of this procedure has increased, with a projected growth of 170% by 2030 and with more than 193,000 procedures performed annually in the United States [2].
Among the British population, the projection of historical rates predicts an exorbitant number of TKA and THA procedures in 2035: about 96,000 THAs and about 119,000 TKAs, although some forecasting models indicate even higher figures. The study was conducted to provide information to policy makers on what the future surgical demand on arthroplasty might be [3].
By 2030 in the US the demand for THA is estimated to grow by 174% and by 673% for TKA. The estimated number is necessary for a proper policy plan on the use of adequate resources that meet this need [4].
Patients undergoing arthroplasty surgery due to osteoarthritis have a high level of expectations before both THA and TKA surgeries. It is well known that generally both interventions significantly improve activities, even though the rate of satisfaction is considerably higher after THA. Preoperative expectations are a major contributor to the final degree of satisfaction one year after surgery. Therefore, preoperative interaction between health care providers and patients is essential to achieve a reasonable outcome [5].
There is increasing interest in robotic-assisted surgery which theoretically aims at achieving short-term and long- term outcomes, as well as a higher survival of the prostheses. Firstly, it is shown that it has a higher surgical precision in reducing misplacements which has been associated, especially for the hip, with higher rates of dislocation, impingement, wear, discrepancy in limb lengths and thus an increase in revisions. In the study by Hadley et al., it has been highlighted that the robotic-assisted THA performed better than the standard technique [6].
In the 2021 review by Ahmed Emara et al., it is shown that robotic-arm assisted hip replacement had higher rates of cup orientation within the Lewinnek and Callanan safe zones, improved femoral stem alignment and offset [7]. In the study by Marcovigi et al., robotic technology was used to assess the influence of native femoral version on final SV and combined anteversion using a straight, uncemented stem and excellent results were delivered [8].
Patient Reported Outcome Measures (PROMs) are questionnaires that are completed by patients in order to collect information about their health status. The term PROMs appeared in the early ’60 of the latest century and their use increased along with the growth of publications since 1980. Today’s challenge is to find reliable and valid instruments for scientific purposes, which are able to determine also the clinical decision-making process [9]. The use of instruments that measure the outcome from the patient’s point of view is well known also in orthopedics and thus in arthroplasty. PROMs instruments with methodological requirements must measure the patients’ general health and well-being, as well as be reliable, valid, determine responsiveness to changes and be acceptable to the intended population. Knowing the results is crucial to interpret whether a patient has had real improvement, for example after surgery [10]. Unfortunately, today there are major obstacles that prevent its full implementation, its proper use and especially the benefits that might result from the use of Patient Reported Outcome Measures [11].
Our study focuses on the use of PROMS because we strongly believe – as Eric C. Makhni explains in his recent 2021 study – that these comprise valuable data, when combined with traditional clinical information and are invaluable tools for improving care and in shared decision-making with patients. PROMs should be introduced in preoperative and postoperative care for clinical monitoring and should be used for predictive analytics and for value-based healthcare delivery pathways [12].
Materials and Methods
The study was approved by Ethics Committee for Clinical Trials of Tuscany Region with Prot. n°13111- 2018 (June 18, 2018) and Det.n°1594 (June 20, 2018).
The observational study was carried out at a hospital in the Asl Toscana Sudest from November 2017 to March 2019. The study considers a sample of patients operated on hip arthroplasty, both by robotic-arm assisted technique and by standard manual technique.
Inclusion/Exclusion Criteria
Males and females, aged 18 to 95 years, were recruited in the study. They all undergone elective hip arthroplasty and were diagnosed with primary osteoarthritis or osteonecrosis.
Patients diagnosed with severe cognitive impairment, traumatic injuries or fractures, major comorbidities such as cancer, cardiovascular, psychiatric, or severe rheumatologic diseases that could affect the functional outcome were excluded. One THA patient with infection was also excluded.
PROMs
The challenges regarding PROMs were meeting regulatory requirements for the collection and processing of sensitive data, some methodological issues such as the length of follow-up visits and the possibility of losing the enrolled patient and consequently of losing data [13].
In order to determine the degree of satisfaction, the scales identified for the study were Harris Hip score, Oxford Hip score, EqolVas, Forgotten Joint Score, and Likert scale. The rating scales were administered the day before surgery and at discharge. Follow-up visits continued 1, 4 and 12 months after surgery. In the preoperative phase, each patient was adequately and comprehensively informed about participation in the study anonymously, according to the principles of good practice in line with the Declaration of Helsinki regarding clinical trials. Patients were also trained to use and compile PROMs in case of scales that needed self- administration.
HHS was compiled and written by a physiotherapist at hospital admission, while the Oxford scale, EquolVas, the satisfaction scale, and FJS were all self-administered. At discharge only HHS scale was administered by a physiotherapist.
One month after surgery, HHS was administered by a physiotherapist, while Oxford scale was self-administered. 4 and 12 months later, HHS scale was administered by a physiotherapist, while Oxford, EqolVas, Likert scale of satisfaction were all self-administered. 12 months later, FJS scale and the satisfaction scale were self-administered.
Description of rating scales
HHS (Harris Hip Score): This rating scale was developed to evaluate the results of hip surgery. The original version was published in 1969. It is administered by health care personnel (a physician or a physical therapist). It consists of 4 sub-scales: pain, function, absence of deformity, ROM measurement. The maximum score is 100: <70 poor function; 70/80 fair function; 80/90 good function; 90/100 excellent function [14, 15].
OHS (Oxford Hip Score): This is a self-administered rating scale. It consists of 12 questions regarding pain, function, and ADL reported over the past 4 weeks. Each question can be answered with a score ranging from 1 to 5. The maximum score is 60 [16, 17, 18].
Euroquol/VAS: This rating scale records the patient’s self- rated health on a 20-cm vertical numbered visual analog scale from 0 to 100, where endpoints are labeled as “Best possible state of health” – which is 100 – and “Worst possible state of health” – which is 0. VAS can be used as a quantitative measure of health outcome that reveal the patient’s judgment [19, 20].
Scala Likert: Likert scale was developed in 1932 as an easy- to-use instrument for measuring opinions and attitudes. It is self-administered and the respondent expresses his/ her degree of agreement/disagreement by choosing from 5 response modes between “completely agree, agree, uncertain, disagree, completely disagree”.
FJS (Forgotten Joint Scale): FJS was created in 2012 to evaluate joint awareness after its prosthesis (both hip and knee) during various activities of everyday life. It consists of 12 questions and it uses Likert (5-point) response format. The maximum score is 100, which means that the patient has almost forgotten that their joint has been operated on [21].
Sample size
A total of 94 robotic-arm assisted THA surgeries were performed during the study period. The 70 THA-operated patients who joined the study underwent questionnaires (PROMs) before surgery, at discharge and 1, 4 and 12 months after surgery.
In order to assess patients’ adaptation to THA by using the FJS scale, one year after surgery 70 patients operated on by robotic-assisted technique vs 31 patients operated on by standard surgery were compared, as well as the degree of satisfaction for surgery and the outcomes in the two groups. All surgeries were performed in the same period. In addition, the surgical and rehabilitation teams, the posterolateral surgical approach and the rehabilitation protocol were the same both in robotic-arm assisted and in standard THA. If the general condition due to anesthesia permitted, patients could be lifted and walk, even on the very day of surgery.
Once discharged from the orthopedic department, some patients continued rehabilitation in the functional rehabilitation and recovery department in the event of general problems. Most of the discharged patients continued rehabilitation in local physiotherapy clinics.
Endpoints
Of particular interest within this study are the functional outcomes of everyday life, as shown by the scores deriving from the administered rating scales and how outcomes progressively increase over time.
Statistical Analysis
Descriptive statistics were used for data of participants. One sample and independent sample T tests were used to assess any differences within and between groups for the continuous variables that are presented with their mean and standard deviation (SD). SPSS software version 12 was used. The significance threshold was set up at P < 0.05.
Results
A total of 94 robotic-asssited THA surgeries were performed between Nov 2017 and March 2019. Among all, 70 patients participated in the study and in follow-up visits that lasted for 12 months (Table 1). There were 36 males and 34 women, with a mean age of 63,76 years. Laterality was 30 left-THA and 40 right-THA. All patients were admitted to the orthopedic department with an average hospital stay of 3.07 days (LOS). Among these, 40 patients were then hospitalized in the low/medium-intensity rehabilitation department, with an average of additional 2.98 days.
The other 30 patients were discharged home directly from the orthopedic surgery department. 37 out of 70 patients were ambulatory on day 0, i.e., the same day of surgery, about 3-4 hours after surgery was completed. The other 33 were ambulatory on day 1, that is the morning after surgery. Walking aids could be either the walker with arm support or forearm crutches, depending on whether the patient felt safe or not.
Hemoglobin before surgery averaged 15.12 (11.6 min - 17.1 max), at discharge it was 11.47 (8.1 min- 14.6 max). ASA-score data were collected. There were 12 patients with ASA 1, 42 patients with ASA 2, 6 patients with ASA 3, 10 patients with unspecified ASA in medical records.
The patients’ height was also measured, with an average of 167, 95 cm. Among these, 159 cm was noted in females and 176, 5 cm in males. The average weight was 82, 24 kg. Among these, 73 kg were registered in females and 92 kg in males. The average BMI was also monitored. The average score was 29, 01; 28, 54 of which were females and 29, 48 were males.
| THAr | 70 pt. | |
|---|---|---|
| Sex | 36 male/ 34 female | |
| Age aver. | 63,76 | |
| Laterality | 30 left/40 right | |
| Hospital stay | 3,07 days | |
| Rehab.depart | 2,98 days | |
| Walking | 37 pt at 0 day | |
| 33 pt at 1° day | ||
| Hb before surg. | 15,12 aver. | (11,6 min- 17,1 max) |
| Hb after surg. | 11,47 aver. | (8,1 min -14,6 max) |
| Asa 1 | 12 pt | |
| Asa 2 | 42pt | |
| Asa 3 | 6pt | |
| Asa missing data | 10pt | Missing data: was omitted during pre-admission assessment or could not be extracted from patient medical chart |
| Height | 167,95 cm | 159 cm female, 176,5 cm male |
| Weight | 82,24 kg | 73 kg female, 92 kg male |
| BMI | 29,01 | 28,54 fem, 29,48 male |
Table 1: Characteristics of participants.
Rating Scale
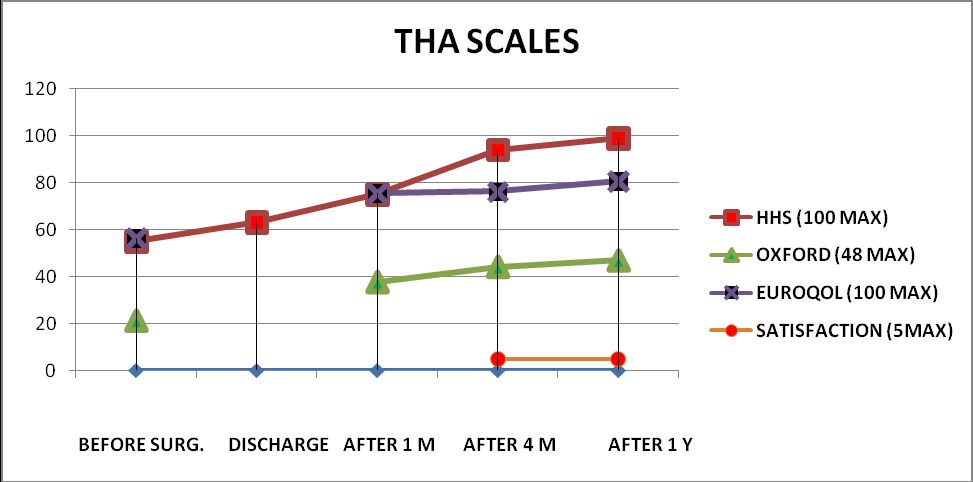
As regards the rating scales which were administered (Table 2): As for Harris Hip Score – considering that the maximum well-being is 100 – there was a mean score of 54, 94 ± 14, 71 before the operation. At hospital discharge, score increased to 63.09±6.83. After 1 month, it was 75, 15±8, 74; 4 months later score sharply increased to 94, 102 ± 6, 08 and after a year it stopped at an average of 98, 63±2,54.
As for the Oxford scale, scores started from 21, 27±9, 24 before surgery (maximum well-being is 48). No assessment was made at discharge because the questionnaire items address everyday life functions with undetectable changes within the hospital a few days after surgery. After a month, score arrived at 37, 78±6, 71, after 4 months scores considerably increased to 44, 16±5, 44. A year later the outcome is 47±2, 06, which is very close to a score of complete well-being.
As regards the Eqol Vas scale, a thermometer-like graph indicating general health status was considered. The patient marked with a cross the score that he considered appropriate for his health status at the time. The rating scale ranges from 0 – minimum well-being and health – to 100 – maximum well-being and health. The score which was found before surgery was 56, 23±20, 04, after a month it was 75,
07±13,83. 4 months later it increased to 76, 11 ± 14, 79 and after a year it increased to 81, 25±15, 84.
With regard to the operation and its outcomes, the satisfaction scale was administered 4 months after surgery and the outcome was 4,67±0,61 and 4,77±0,54 one year later. The rating scale had been administered no earlier than 4 months because in most cases there was no complete stabilization of the post-surgical state of health (due to pain, hypotonia and muscular hypotrophy, edema and swelling of the operated limb, etc...), which may obviously affect satisfaction. This scale was also administered to patients operated on by standard method 12 months after and the result was 4.47±0.83 and with P<0.05, which is statistically significant (Table 3).
The Forgotten Joint Score was administered 12 months after surgery (the process of adaptation to hip may not yet be evident before) and the outcome was compared with that obtained from patients operated on by standard hip replacement during the same period, from the same surgical team and followed by the same team of physiotherapists. The score in the robotic prosthesis group was 86, 27± 21, 10, while in the standard group was 87, 02 ±16, 57. Since P=0, 86, the outcome is not statistically significant for P<0,05 (Table3).
| BEFORE SURGERY | DISCHARGE | AFTER 1 Month | AFTER 4 Months | AFTER 1 Year | |
|---|---|---|---|---|---|
| HHS (0 min - 100 max) | 54,94±14,71 | 63,09±6,83 | 75,15±8,74 | 94,102±6,08 | 98,63±2,54 |
| OXFORD (0 min-48 max) | 21,27±9,24 | 37,78±6,71 | 44,16±5,44 | 47±2,06 | |
| EUROQOL (0 min-100 max) | 56,23±20,04 | 75,07±13,83 | 76,11±14,79 | 81,25±15,84 | |
| FJS(0min-100 max) | 86,27±21,1 | ||||
| SATISFACTION (0 min-5max) | 4,67±0,61 | 4,77±0,54 |
Table 2: value scales.
| AFTER 12 MONTHS | FORGOTTEN J.S. (FJS) | SATISFACTION SCALE | ||
|---|---|---|---|---|
| 70THA r | 86,27± 21,10 | P=0,86 | 4,77±0,54 | P<0,05 |
| 31THA s | 87,02 ±16,57 | 4,47±0,83 |
Table 3: FJS and Satisfaction Scale (standard THA vs robotic-assisted THA).
The number and percentage of patients with maximum scores in the administered scales was also highlighted (Table 4). In HHS scale, 44 patients out of 70 reported maximum score (100), with a percentage of 62.85%. In the Oxford scale, 46 patients out of 70 reported maximum score (48), with a percentage of 65.71%. In the Eqolvas scale, only 5 patients gave maximum score (100), with a percentage of 7.14%. In the satisfaction scale 51 patients were satisfied with the intervention with a percentage of 72.85%.
| Robotic-assisted THA SCALES | VALUE MAX | TOT.PT 70 | PERCEN. |
|---|---|---|---|
| HHS(0 min - 100 max) | 100 | 44 | 62,85% |
| OXFORD(0 min-48 max) | 48 | 46 | 65,71% |
| EUROQOOL(0 min-100 max) | 100 | 5 | 7,14% |
| SATISF.(0 min-5max) | 5 | 51 | 72,85% |
Table 4: maximum value on scales and percentages in robotic-assisted THA.
The graph illustrates the increasing outcomes of the various rating scales over time (Figure 1).
We compared (Table 5) by T-test the average resulting from the administered rating scales before hip surgery and 12 months later.
As concerns hip replacements, we compared the resulting scores within the HHS scale before surgery (54, 94±14, 71) and 12 months later (98,63±2,54). The average between the observed differences is significant for P<0, 05.
We also compared the resulting scores within the Oxford scale before surgery (21, 27±9, 24) and 12 months later (47±2, 06). The average between the observed differences is significant for P<0, 05.
In the EqolVas scale the comparison was between the resulting scores before surgery (56, 23±20) and 12 months later (81, 25±15, 84). The average between the observed differences is significant for P<0, 05.
Only the satisfaction scale was administered for the first time 4 months after surgery (4, 67±0, 61) and 12 months after surgery (4, 77±0, 54). The average between the observed differences is not significant for P<0, 05, since P=0, 3062.
| BEFORE SURGERY | AFTER 4 MONTHS | AFTER 12 MONTHS | P<0,05 | |
|---|---|---|---|---|
| HHS | 54,94±14,71 | 98,63±2,54 | P<0,05 | |
| Oxford | 21,27±9,24 | 47±2,06 | P<0,05 | |
| Eqolvas | 56,23±20 | 81,25±15,84 | P<0,05 | |
| Satisf.f.scale | 4,67±0,61 | 4,77±0,54 | P=0,3062 |
Table 5: Comparison scales before surgery, after 4 m., after 12 m., in robotic-assisted THA.
Discussion
Robotic surgery in literature appears to have higher outcomes both in THA and TKA, as compared with standard surgery. Specifically, the preeminence of robotic prosthesis has been demonstrated by accuracy in placement of prosthetic components. Through the use of robotics, the so-called outliers in anatomic-radiographic outcomes are reduced.
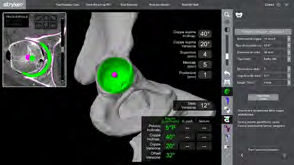
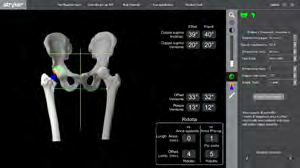
Robotic hip replacement appears to be associated with greater accuracy of both the acetabular and femoral components. This facilitates restoration of the center of rotation with the corresponding acetabular, femoral and global offsets. In addition, the MAKO technique offers a customized dynamic 3D-planning by matching preoperative CT data with intra-operatively detected data. This enables to quantify and to correct pathological-anatomical data, as well as the components’ sizing, such as length, offset, cup and femoral neck version, and especially the so-called combined version (cup + acetabulum). The mutual anteversion of the acetabular cup and stem neck is the key element for the functional kinematics of hip prosthesis and for reducing the probability of negative phenomena in hip replacement i.e. impingement, edge loading and instability, which could consequently lead to dislocation and increased wear. Robotic planning and execution reduce the likelihood of these negative phenomena occurring, as they can highlight and reduce anatomical orientation defects through anteversion modification of prosthetic components. (Images 1-2-3-4-5 by Dr P.Caldora) (Figures 2-6).



Robotic hip replacement thus appears to be associated with greater accuracy of the center of rotation, optimization of offset and precise positioning of the acetabular component, as compared with manual prosthesis. This was confirmed by the study of Kayani et al. that emphasized the Mako system, since this gave more favorable outcomes with similar complications to standard surgery [22].
In addition to the level of accuracy of the prosthetic components, other comparative factors related to the manual technique were studied. The study by Caldora et al. (2020) demonstrates that there is statistical significance in the reduction in the number of transfusions (p<0.001) and hospital stay (p<0.01) in favor of robotic-assisted THA versus standard surgery [23]. The 2021 study by Clement et al. reported that patients who underwent robotic-assisted THA had a greater functional outcome than standard THA, related to improved positioning of components, although there was no difference between the two groups in postoperative general health and satisfaction [24].
In our previous study by Banchetti, et al. [25] we observed that - when comparing PROMs between 120 standard procedures and 100 robotic THA - there was statistical significance in favor of robotics concerning the length of hospital stay, which was lower in robotic prostheses. There were no significant differences between the robotic and standard groups with regard to the outcomes obtained from the PROMs used but rather a significant improvement with regard to postoperative outcomes 2 years after surgery in both surgical techniques (P<0.001).
Although the advantage of implant accuracy is evident when using robotics, other authors amplify some of its limitations, such as the robot’s cost, the presence of additional professionals, such as the biomedical engineer during operation or the consideration that not all hospitals are able to acquire this technology, which is considered expensive and not yet beneficial if compared to cost [26].
Domb’s [27] study reports that 5 years after surgery outcomes are more favorable for robotic prostheses with higher scores than standard prostheses, with 89% reduced risk on acetabular implant placement.
Despite all, scientific studies highlight how hip or knee replacements – operated on with manual and robotic techniques – result in significant improvement from a functional, quality-of-life, and pain point of view. Some studies specify that the outcomes in THA are superior to those concerning TKA, with higher quality-of-life satisfaction in THA. Satisfaction seems to derive from a high level of expectation in the preoperative phase: where it is higher, the outcome seems greater from a quality perspective [28, 29].
Other studies affirm that expectations with regard to pain and walking ability are moderately or not at all correlated with satisfaction [30, 31].
The findings of our study reveal how robotic-assisted THA have an inevitable progressive improvement in both pain and quality of life over time, before surgery and up to the first year, with statistical significance. Furthermore, the satisfaction scale has become increasingly crucial over time for the outcome of arthroplasty. It does not clarify what the patient is satisfied with, and for that reason it is definitely a multidimensional construct. It can be related to the process of care delivery, empathy with the surgeon and nursing staff, or negatively linked to problems in the postoperative process (delay in starting physical therapy or difficulty in motor recovery, persistent pain). Satisfaction could be correlated with improvement in the ability to perform work or recreational activities and with the extent of pain relief [32, 33, 34]. In our study, robotic patients reported an excellent outcome 1 year after surgery (4, 77±0, 54), very close to the maximum score, which is 5. Also patients operated on by standard method have a very high value 1 year after surgery (4,47±0,83) but what is definitely interesting is the outcome obtained in our study in favor of robotics, with statistical significance (P<0,05). More studies are necessary in order to define the factors that influence patient satisfaction after THA surgery – especially in robotic-assisted THAs – such as young age, good preoperative physical condition and good mental health, including the optimistic expectation of results by the surgeon [35].
Overall, it is evident that, one year later, meeting the expectations [36] is highly correlated with improvement in mobility and pain. This confirms that satisfaction is not associated with age, gender, race or social status [37] but with the expectation in the preoperative phase of an optimal quality of life with absence of pain.
We can deduce, then, that the perception of forgetting the artificial joint during everyday life and in recreational activities is an added value that thus determines the patient’s satisfaction and the patient’s preference of one surgical technique over another [38].
The FJS scale provides us with important information with regard to the process of adaptation to prosthesis and it is in line with the outcomes of the Oxford scale. For this reason, many studies are moving toward the combined use of the Oxford and FJS scales to have more and more specific data on functional outcomes in arthroplasty [39]. In the study by U. G. Longo, et al. [40], a range of FJS values (69.8 to 91.7) was found, which is considered as cut-offs within which there is a minimal clinical difference (MCDI) and an acceptable state of symptoms (PASS) that can correspond to a satisfactory quality of life.
On the other hand, in the study by Puliero, et al. [41] it is ascertained that only with scores higher than 93 in the FJS, patients perceive the replaced hip as if it is natural, that is, they forget that it is artificial. However, in 20-30% of cases, the Womac scale combined to FJS failed to identify the forgotten joint because patients did not perceive adaptation, although the outcomes reached the maximum score.
In our study, the 1-year values of FJS in robotic-assisted (86.27± 21.10) and standard (87.02 ±16.57) arthroplasty are similar. There is no statistical significance and they are within the range of scores considered as cut offs in Longo’s study, and in any case not far from Puliero’s 93 score. In the two types of interventions, the outcomes cancel each other out in the long term. Therefore, more studies are needed in order to strengthen the evidence for comprehensive answers.
Conclusions
Patients who undergo hip arthroplasty surgery all have a high level of expectation and clinical outcomes are very satisfactory regardless of the robotic technique. The index of functional improvement, well-being, satisfaction and quality of life increases with time after surgery. Some studies report more favorable short/medium-term outcomes, fewer transfusions, and fewer days of hospital stay in the robotic- assisted surgery compared to the standard one, while differences in function and quality of life in the first year after the two different types of surgery tend to cancel each other out. Our study showed no statistically significant differences between the robotic and manual samples with regard to the FJS scale but instead it gave statistical significance for the satisfaction scale. The latter parameter could also depend on the psychological conditioning of the patient for being operated on with advanced technology but still represents a positive aspect for the patient and a coefficient of attraction for the hospital and the surgical team.
This study makes some points that need to be evaluated more carefully and with more targeted studies of higher level. One question is, why the greater accuracy of prosthetic component placement with the robotic technique does not result in better functional outcomes (FJS scale) one year later, when compared to the sample of manually operated hip replacements? The other question is, how come that at the same time robotic patient shows greater satisfaction?
Our study has some limitations. It was a retrospective analysis and the sample had a small number, especially of patients operated on with standard method. In addition, the lack of long-term follow-ups does not highlight any differences in complications in both robotic and standard groups of patients. Further research is needed in order to report functional outcomes, data on survival of the prosthesis, complications, cost-effectiveness but also research with regard to long-term PROMs i.e. beyond 10 years.
References
-
Learmonth ID, Young C, Rorabeck C (2007) The operation of the century: total hip replacement. – Lancet 370(9597): 1508-1519.
-
Deak N, Varacallo M (2022) Hip Precautions. In: Stat Pearls [Internet]. Treasure Island (FL), pp: 30725716.
-
Culliford D, Maskell J, Judge A, Cooper C, Prieto Alhambra D, et al. (2015) Future projections of total hip and knee arthroplasty in the UK: results from the UK Clinical Practice Research Datalink. COASt Study Group, Osteoarthritis and cartilage 23(4): 594-600.
-
Steven K, Kevin O, Edmund L, Fionna M, Michael H (2007) Projections of primary and revision hip and knee arthroplasty in the USA from 2005 to 2030. JBJS 89(4): 780-785.
-
Neuprez A, Delcour JP, Fatemi F, Gillet P, Crielaard JM, et al. (2016) Patients’expectatios impact their satisfaction following total hip or knee arthoplasty. PloS ONE 11(12): e0167911.
-
Hadley CJ, Grossman EL, Mont MA, Salem HS, Catani F, et al. (2020) Robotic-Assisted versus Manually Implanted Total Hip Arthroplasty: A Clinical and Radiographic Comparison. Surg Technol Int 28(37): 371-376.
-
Emara AK, Samuel LT, AJ Acuña, A Kuo , Khlopas A, et al. (2021) Robotic-arm assisted versus manual total hip arthroplasty: Systematic review and meta-analysis of radiographic accuracy. Int J Med 17(6): e2332.
-
Marcovigi A, Ciampalini L, Perazzini P, Caldora P, Grandi G, et al. (2019) Evaluation of Native Femoral Neck Version and Final Stem Version Variability in Patients With Osteoarthritis Undergoing Robotically Implanted Total Hip Arthroplasty. J Arthroplasty 34(1): 108-115.
-
Churruca K, Pomare C, Ellis LA, Long JC, Henderson SB, et al. (2021) Patient-reported outcome measures (PROMs): A review of generic and condition-specific measures and a discussion of trends and issues. Health Expect 24(4): 1015-1024.
-
Collins NJ, Roos EM (2012) Patient-reported outcomes for total hip and knee arthroplasty: commonly used instruments and attributes of a “good” measure. Clin Geriatr Med 28(3): 367-394.
-
Whitebird RR, Solberg LI, Ziegenfuss JY, Norton CK, Chrenka EA, et al. (2022) What Do Orthopaedists Believe is Needed for Incorporating Patient-reported Outcome Measures into Clinical Care? A Qualitative Study. Clin Orthop Relat Res 480(4): 680-687.
-
Makhni EC (2021) Meaningful Clinical Applications of Patient-Reported Outcome Measures in Orthopaedics. J Bone Joint Surg Am 103(1): 84-91.
-
Laboratorio Management e Sanità-Scuola Superiore Sant’Anna di Pisa (2017) Dalle valuatazioni tradizionali di outcome ai Patient-Reported Outcome Measures (PROMs) in chirurgia elettiva.
-
Söderman P, Malchau H (2001) Is the Harris hip score system useful to study the outcome of total hip replacement?. Clin Orthop Relat Res (384): 189-197.
-
Kirmit L, Karatosun V, Unver B, Bakirhan S, Sen A, et al. (2005) - The reliability of hip scoring systems for total hip arthroplasty candidates: assessment by physical therapists. Clin Rehabil 19 (6): 659-661.
-
Murray D, Fitzpatrick R, Rogers K, Pandit H, Beard D, et al. (2007) The use of the Oxford hip and knee scores. J Bone Joint Surg Br 89: 1010-1014.
-
Dawson J, Fitzpatrick R, Carr A, Murray D (1996) Questionario sulle percezioni dei pazienti sulla sostituzione totale dell’anca. J Bone Joint Surg Br 78(2): 185-190.
-
Dawson J, Fitzpatrick R, Murray D, Carr A (1998) Questionnaire on the perceptions of patients about total knee replacement. The Journal of Bone and Joint Surgery British volume 80(1): 63-69.
-
Yan Feng, David Parkin, Devlin NJ (2014) Assessing the performance of the EQ-VAS in the NHS PROMs programme. Quality of Life Research 23(3): 977-989.
-
Devlin N, Parkin D, Janssen B (2020) Methods for Analysing and Reporting EQ-5D Data. Cham (CH): Springer, Analysis of EQ VAS Data pp: 51-59.
-
Matsumoto M, Baba T, Homma Y, Kobayashi H, Ochi H, et al. (2015) Validation study of the Forgotten Joint Score-12 as a universal patient-reported outcome measure. Eur J Orthop Surg Traumatol 25(7): 1141-1145.
-
Kayani B, Konan S, Thakrar RR, Huq SS, Haddad FS (2019) Assuring the long-term total joint arthroplasty: a triad of variables. Bone Jt J 101:11-18.
-
Caldora P, Urso AD, Banchetti R, Arniani S, Colcelli D, et al. (2020) Blood transfusion, hospital stay and learning curve in robotic assisted total hip arthroplasty. (Congress of the Italian Orthopaedic Research Society.) D.J Biol Regul Homeost Agents 34: 37-49.
-
Clement ND, Gaston P, Bell A, Simpson P, Macpherson G, et al. (2021) Robotic arm-assisted versus manual total hip arthroplasty. Bone Joint Res 10(1):22-30.
-
Banchetti R, Dari S, Ricciarini ME, Lup D, Carpinteri F, et al. (2018) Comparison of conventional versus robotic- assisted total hip arthroplasty using the Mako system: An Italian retrospective study. Journal of Health and Social Sciences 3(1): 37-48.
-
Kouyoumdjian P, Mansour J, Assi C, Caton J, Lustig S, et al. (2020) Current concepts in robotic total hip arthroplasty. SICOT J 6: 1-45.
-
Domb BG, Chen JW, Lall AC, Perets I, Maldonado DR (2020) Minimum 5-Year Outcomes of Robotic-assisted Primary Total Hip Arthroplasty With a Nested Comparison Against Manual Primary Total Hip Arthroplasty: A Propensity Score-Matched Study. J Am Acad Orthop Surg 28(20): 847-856.
-
Anakwe RE, Jenkins PJ, Moran M (2011) Predicting dissatisfaction after total hip arthroplasty: a study of 850 patients. J Arthroplasty 26(2): 209-213.
-
Gonzalez Saenz de Tejada M, Escobar A, Bilbao A, Espiñeira CH, García Perez L, et al. (2014) A prospective study of the association of patient expectations with changes in health-related quality of life outcomes, following total joint replacement. BMC Musculoskelet Disord 15: 1-248.
-
Eisler T, Svensson O, Tengström A, Elmstedt E (2002) Patient expectation and satisfaction in revision total hip arthroplasty. J Arthroplasty 17(4): 457-462.
-
Lingard EA, Sledge CB, Learmonth ID, Kinemax Outcomes Group (2006) Patient expectations regarding total knee arthroplasty: differences among the United States, United Kingdom, and Australia. - J Bone Joint Surg Am 88(6): 1201-1207.
-
Graham B, Green A, James M, Katz J, Swiontkowski M (2015) Measuring patient satisfaction in orthopaedic surgery. J Bone Joint Surg Am 97(1): 80-84.
-
Shirley ED, Sanders JO (2016) Measuring quality of care with patient satisfaction scores. J Bone Joint Surg Am 98(19): e83.
-
Sidani S, DR Epstein, M Fox (2017) Psychometric evaluation of a multi‐dimensional measure of satisfaction with behavioral interventions. Res Nurs Health 40(5): 459-469.
-
Palazzo C, Jourdan C, Descamps S, Nizard R, Hamadouche M, et al. (2014) Determinants of satisfaction 1 year after total hip arthroplasty: the role of expectations fulfilment. BMC Musculoskelet Disord 15(53).
-
Scott CEH, Bugler KE, Clement ND, MacDonald D, Howie CR, et al. (2012) Patient expectations of arthroplasty of the hip and knee. J Bone Joint Surg Br 94(7): 974-81.
-
Mahomed NN, Liang MH, Cook EF, Daltroy LH, Fortin PR, et al. (2002) The importance of patient expectations in predicting functional outcomes after total joint arthroplasty. J Rheumatol 29(6): 1273-9.
-
Azzi E, Thienpont E, M Avaux, FA Houssiau, P Durez (2014) The Forgotten Joint Score, A New Questionnaire to Evaluate Patient’s Perception of Total Knee and Hip Arthroplasty in Patients with Established Rheumatoid Arthritis. Annals of the Rheumatic Diseases 73(2).
-
Galea VP, Ingelsrud LH, Florissi I, Shin D, Bragdon CR, et al. (2020) Patient-acceptable symptom state for the Oxford Hip Score and Forgotten Joint Score at 3 months, 1 year, and 2 years following total hip arthroplasty: a registry-based study of 597 cases. Acta Ortho 91(4): 372-377.
-
Longo UG, Salvatore SDe, Piergentili I, Indiveri A, Naro CDi, et al. (2021) Total Hip Arthroplasty: Minimal Clinically Important Difference and Patient Acceptable Symptom State for the Forgotten Joint Score 12. Int J Environ Res Public Health 18(5): 2267.
-
Puliero B, Blakeney WG, Beaulieu Y, Vendittoli PA (2019) Joint Perception After Total Hip Arthroplasty and the Forgotten Joint. J Arthroplasty 34(1): 65-70.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda