Mental Health Issues and Coping Mechanism adopted by Primary Healthcare Workers against COVID-19: A Study in Northwestern State of India
Background: The healthcare providers (HCWs) of primary health facilities suffered with dual burden of work, as they had to deliver COVID-19 related services along with routine work, which put immense strain on their capacities. Objective: To assess the prevalence of mental health issues among HCWs of public primary health facilities and understand the coping mechanisms adopted by them during the first wave of the COVID-19 pandemic. Method: It is a cross-sectional study, conducted by administering telephonic and self-administered questionnaires with a sample of 272 HCWs from 24 public primary healthcare facilities of 13 districts in the state of Rajasthan. Result: 76.2% had a fear of getting infected, whereas 56.3% were not able to spend time with family, and 41% had less time for rest while working in the pandemic. The pandemic impacted the lives of HCWs beyond the workplace, significantly affecting their personal lives as well, leading to mental health-related issues. 53% of HCWs experienced depression ‘sometimes’, followed by anger, boredom, irritability, and fear. Age and type of residence were found to be significantly associated with mental health issues. Exercise (44.9%), followed by yoga (29.4%), and meditation (22.8%) were a few coping mechanisms adopted by HCWs. Conclusion: The impact of COVID-19 on mental health varied with the background characteristics like age, sex, residence, workplace, and nature of work. There is a need to create a resilient health system to support s in primary health facilities.
Introduction
The exceptional response by healthcare workers (HCWs) in the fight against COVID-19 pandemic unquestionably makes HCWs the COVID-19 warriors [1]. The pandemic demonstrated that healthcare personnel were the cornerstone of healthcare systems, and their dedication and professionalism was excellent throughout the pandemic [2]. They remained motivated and resolutely continued their work [3]. The health systems were never challenged to this extent in recent history, and the laid-out systems for business as usual was not adequate to address the demand during the COVID-19 pandemic. The resources available and the business hours were stretched to its extreme and HCWs were at the forefront in absorbing this. Despite their dedication and resolve, globally HCWs faced situational and organizational challenges often during the pandemic. due to inadequate health infrastructure, long working hours, inadequate logistics and supplies, shortage of personal protective equipment, social stigma, stressful environment, and occupational burnout [4].
India, to show gratitude towards its HCWs, the Indian Medical Association (IMA) declared ‘Save the Saviours’ as the theme for National Doctor’s Day in 2021, observed on July 1 each year [5]. Honoring the HCWs, including doctors, is important to boost their morale because they played a pivotal role in dealing with the pandemic despite varied challenges. However, the pandemic showed that doctor-to- patient ratio and insufficient medical facilities [6] exerted immense pressure on Indian healthcare system and there were incidences of violence and stigma against healthcare providers during the pandemic [7].
In the first wave, by August of 2020, about 87,000 healthcare workers were infected in six Indian states [8]. Data collected by the Indian Medical Association, shows nearly 1,800 doctors succumbed to the infection during the course of COVID-19 pandemic, 757 during the first wave, 839 during the second wave and the remaining thereafter [9]. Multiple studies show that several risk factors- age, gender, medical specialty, lack of training to deal with COVID-19, mismanagement, lack of adequate PPE, race and ethnicity, and other factors such as comorbidities were associated with increased mortality amongst HCWs including doctors [10]. A US study found that HCWs who died of COVID-19 were disproportionately older (>50 years of age), male, and Black or Asian [11] and another study found that Healthcare workers are seven times as likely to have severe COVID-19 as others engaged in ‘non-essential’ jobs [12].
COVID-19 pandemic has imposed significant physical and psychological burden on physicians and other HCWs [13]. The psychological burden and overall wellness of HCWs have received heightened attention, with research continuing to show high rates of burnout, psychological stress, and suicide [14]. A scope review in terms of stress and trauma- related symptoms in HCWs shows the prevalence ranged from 7.4% to 35%, particularly among women, nurses, frontline workers, and in workers who experienced physical symptoms [15]. Detrimental effects include high rates of infection and death, excessive financial hardships, stress related to known and particularly unknown information, and fear of uncertainty regarding continued impact [14]. Studies indicate that up to 75% of doctors have experienced workplace violence, which often results in psychological issues, absenteeism, shattering mental peace, self-esteem, and diminished service quality [7]. The reasons also include stress due to their profession, working in the affected areas, lack of support from health authorities, inadequate time for family care, and stigma associated with COVID-19 [16, 17, 18]. In a systematic review study, the prevalence of anxiety and depression was found relatively high among healthcare workers during the COVID-19 pandemic [19]. A study in Iran found that the prevalence of anxiety and depression was significantly higher in doctors and nurses compared with other occupations [20]. Similarly in another study in India the prevalence of anxiety disorder and depression were significantly higher among those with clinical responsibilities compared to those with supportive responsibilities [21]. The current paper is analyzing such issues through the study conducted with HCWs of primary healthcare facilities in the state of Rajasthan, India, during the COVID19 pandemic.
Study Objective
To assess the prevalence of mental health issues among HCWs of public primary health facilities and understand the coping mechanisms adopted by them during the first wave of the COVID-19 pandemic.
Material and Methods
Study Design
It is a cross-sectional study conducted among healthcare workers of primary health facilities to understand their knowledge and participation in COVID-19 activities and their perceptions regarding personal risk, family, and community. The study also tries to assess preparation of facilities during COVID-19 to support the HWCs against the risk of infection and the challenges being faced by them while working during the pandemic.
Sample Size and Respondents
A study was conducted with 272 HCWs from 24 public primary healthcare facilities (7 urban and 17 rural) spread across 13 districts in the state of Rajasthan during April 2020 to May 2020. The data was collected from a formal and consented interactions conducted with HCWs (doctors, staff nurses, Lady Health Visitors (LHV), Auxiliary Nurse Midwives
(ANMs), Pharmacists, lab technicians, Multipurpose Health Workers (MPHW)) posted at public primary healthcare facilities to understand the aforementioned mental health issues in the state of Rajasthan, India, during the COVID-19. Among the 280 selected staff to administer the survey the response was received from 272 (97.1%) respondents. Among the 272 respondents, the majority, 105, were ANMs, followed by 53 Staff Nurse, 34 MPWs, 22 MOICs (Medical Officers in-Charge), 22 Pharmacists, 20 lab technicians and 16 LHVs.
Study Settings
The 24 public facilities selected were managed by LEHS (Lords Education & Health Society- a non-governmental organization) under its flagship program WISH (Wadhwani Initiative for Sustainable Healthcare) in a public-private partnership mode through a formal agreement with the Rajasthan Government. The study was conceptualized and completed from April to May 2020, during first wave of COVID-19 pandemic.
Inclusion Criteria
Only the medical and paramedical staff at all facilities being managed by LEHS|WISH was included in the study.
Exclusion Criteria
The HCWs with whom the study tools were pretested, were excluded from the study.
Data Collection Tools
Being mindful of the in-force COVID-19 social distancing protocols, the data collection was carried out using online survey tools (google form). There were two close-ended questionnaires as part of the self-administered questionnaire (Part A), and a telephonic/mobile survey questionnaire (Part B). Part ‘A’ covered information related to demographic characteristics, personal health, participation in COVID-19 response, perceived risks, and associated coping mechanism, whereas part ‘B’ covered information on awareness and exposure of staff to COVID-19 related risks, type of support HCWs received and challenges faced at health facilities and impact of COVID-19 on their life. The validity and reliability of the tools were assessed by applying ALPHA test on both part ‘A’ and part ‘B’ of the questionnaire. The overall scale reliability coefficient was 0.7689 for part ‘A’ and 0.6686 for part ‘B’.
Data Collection Process
As the survey was conducted at LEHS|WISH managed facilities, the study respondents- HCWs were those who were recruited as LEHS|WISH staff, and hence their contact details including address, mobile numbers and email IDs were available with the human resource department of LEHS|WISH.
Data Quality
Data quality at all stages of the study was duly ensured at all levels, starting from tool designing to data collection. The tools were pretested for consistency, sequencing, skip pattern of questioning, identifying any repetition, and completeness of the information. All interviewers were trained virtually, and guided interviews were conducted for monitoring and supervision of the quality of interaction.
Ethical Approval
Ethical approval was obtained from Sigma IRB board following all required compliances.
Consent
A virtual (Google) consent form was shared with the respondents informing them of the purpose of the survey, process of data collection, risks and benefits of participating in the survey, and regarding process to ensure confidentiality of the collected data and their privacy. It was clearly described in the consent form that their participation is voluntary and they are free to withdraw at any time during the interview.
Statistical Analysis
The data was analyzed using STATA-15. In order to assess the level of mental health issues, namely, depression, irritability, insomnia, fear, confusion, anger and boredom, they were listed in the questionnaire and the respondents were asked to respond in terms of ‘often’, ‘sometimes’ or ‘never’; ‘Often’ considered as ‘very frequently’ and ‘sometimes’ considered as ‘not very frequently’. The collated responses were analyzed to assesses the prevalence of any of the mental health issues being studied among the HCWs. Univariate and Bivariate analyses were undertaken to understand the mental health status of medical and paramedical staff by background characteristics. Chi-square statistical test was applied to measure the association between any mental health issues among medical staff, by background characteristics.
Result of the Study
Medical doctors accounted for 8% of the staff, and ANMs (38.1%) & staff nurses (19.5%) make up majority of the surveyed HCWs. Majority of the respondents (57.4%) were females, more than three-fourth were married. Half of the respondents were in the age group of 25-30 years (Table 1). Of the surveyed, nearly three-fourths worked in rural PHCs and remaining in urban facilities. Nearly 48.2% of the staff belonged to other districts in the state and living in a rented accommodation near the facility of their posting as there was no provision of residences at the concerned facility. About 7% of staff was vulnerable due to their personal health conditions as some were either pregnant or suffering from chronic health conditions such as Diabetes Mellitus, Hypertension and Asthma. During COVID-19 pandemic these populations were categorized as high-risk populations and were asked to take extra precautions to safeguard themselves from COVID-19 infection and the resulting complications.
| N | % | |
|---|---|---|
| Age (Years) | ||
| 20-24 | 42 | 15 |
| 25-30 | 136 | 50 |
| 31-35 | 57 | 21 |
| >35 | 37 | 14 |
| Sex | ||
| Male | 116 | 43 |
| Female | 156 | 57 |
| Marital Status | ||
| Married | 207 | 76 |
| Unmarried | 58 | 21 |
| Separated/divorce/other | 7 | 2.5 |
| Place of Posting | ||
| Rural | 206 | 76 |
| Urban | 66 | 24 |
| Type of residence | ||
| Government sanctioned staff residences | 64 | 24 |
| Rented accommodation | 131 | 48 |
| Own residence | 77 | 28 |
| Designation | ||
| Medical officer in-charge (MOIC) | 22 | 8.1 |
| Pharmacist | 22 | 8.1 |
| Lady Health Visitor (LHV) | 16 | 5.9 |
| Staff Nurse | 53 | 20 |
| ANM | 105 | 39 |
| Lab Technician | 20 | 7.4 |
| Multipurpose Worker (MPW) | 34 | 13 |
| Work place in home district | ||
| No | 131 | 48 |
| Yes | 141 | 52 |
| Personal health risks | ||
| Pregnant | 7 | 2.6 |
| Diabetic | 2 | 0.7 |
| Hypertension | 6 | 2.2 |
| Asthma | 3 | 1.1 |
| Total | 272 |
Table 1: Background characteristics of healthcare workers, year 2020.
While HCWs remained steadfastly committed to their duties, their unwavering engagement also exposed them to increased risk of infection due to prolonged working hours, shortage of personal protective equipment, disruption to their social and family ties, and unfortunately, instances of violence from relatives of the patients and public [22, 23]. Table 2 provides apprehensions of HCWs for their families amidst the pandemic to a multi-response question. Excluding the 12.5% (34 HCWs) who had no worries, remaining 87.5% (238 HCWs) were analyzed across three distinct categories: i) HCWs stationed in their home district, ii) those posted and working in a different district and, iii) in totality. HCWs residing in districts other than their home district and away from their families exhibited heightened concerns for wellbeing of their families. Notably, among those residing in different districts, 50% expressed their worry on the uncertainty of days for reuniting with their families. In contrast, HCWs living in their home district displayed notably a lower percentage (20%). Considering all responses, over two-thirds of the respondents were occupied with the thought that their family would be worried about their wellbeing; whereas almost equal number of HCWs had fear of transmitting infection to their family members. More than half of the HCWs were worried regarding health of the elderly parents and 47.1% regarding wellbeing of their children. This underscores the complex array of anxieties that HCWs grappled with while performing their duties during the pandemic.
| Work place in home district (N=119) (%) | Work place outside home district (N=119) (%) | Total (N=238) | |
|---|---|---|---|
| Fear of passing infection from me to my family | 68.9 | 68 | 68.5 |
| Spending time with the family/ children | 36.9 | 44.5 | 40.8 |
| Health and Wellbeing of children* | 56.1 | 57.3 | 56.7 |
| Health and Wellbeing of children* | (N=98) | (N=89) | (N=187) |
| Health and Wellbeing of spouse** | 41.9 | 51.1 | 46.4 |
| Health and Wellbeing of spouse** | (N=93) | (N=88) | (N=181) |
| Shortages in supplies of food, cooking fuel, and medicine at home | 21.8 | 24.3 | 23.1 |
| Health of elderly parents in family | 57.1 | 56.3 | 56.7 |
| Education of children | 31.1 | 32.7 | 31.9 |
| Family is worried about us | 68.9 | 73.9 | 71.4 |
| When I will be able to go home | 20.1 | 50.4 | 35.3 |
| Someone may get infected in family | 63.8 | 62.1 | 63 |
Table 2: Concerns of HCWs for their families during work in COVID-19 (N=238).
*Unmarried respondents are excluded; **only for married respondents, whereas, unmarried divorced and separated are excluded. Table 2: Concerns of HCWs for their families during work in COVID-19 (N=238).
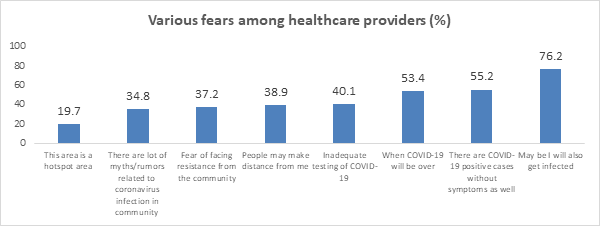
Figure 1 illustrates eight distinct types of challenges that healthcare providers encountered at personal and professional level. Apart from 36.8% who had no fear of working during COVID-19 pandemic, the other HCWs mentioned one or more than one type of fear. Nearly three- fifths (76.2%) of the respondents had fear of getting infected and 55.2% of HCWs had this fear because many COVID-19 positive cases were asymptomatic and difficult to identify, whereas 53.4% were uncertain about when the pandemic would be over. Technical issues like inadequate testing of COVID-19 (40.1%), issues of social stigma such as fear of facing resistance from the community (37.2%), and people distancing from them (38.9%) also contributed to declining morale amongst the HCWs. Compounding these challenges, the prevalence of various myths and rumors concerning COVID-19 in the community (34.8%) contributed in further heightening psychological and mental distress amongst them. These psychological burdens added an additional layer of complexity to the already demanding roles being undertaken by HCWs during this unprecedented time. Figure 1 highlights the multifaceted nature of the challenges faced by HCWs beyond the professional duties, delving into personal fears, uncertainties, and the detrimental effects of social and psychological factors.
Several studies suggest that while working in the pandemic HCWs were susceptible to distress and negative health outcomes including anxiety, poor quality sleep, and feelings of isolation [24, 25]. Analysis of a multi-response question Table 3 illustrates how pandemic affected the personal life of HCWs. Many (56.3%), were not able to spend adequate time with family or were not able to visit home (46%) during the pandemic. The impact on personal wellbeing was further evident, with 41% of HCWs expressing they had less time available for rest. Moreover, 45% indicated that they struggled to dedicate enough time to personal care routines, including timely meals. An additional 28% faced challenges in managing routine activities such as laundry and cleaning due to time constraints.
On the positive front, a substantial (72%) of the HCWs reported that they acquired new skills relevant for work/ profession and 58% learnt new skill for day-to-day life. It can be concluded that although during pandemic the family time, personal care, and routine management of HCWs was compromised; they exhibited adaptability and capacity to embrace new opportunities for growth and skill acquisition.
| Type of impact | Response | |
|---|---|---|
| N=272 | % | |
| Getting less time to take rest | 111 | 40.8 |
| Not able to visit home | 125 | 46 |
| Not able to spent adequate time with family / have to keep myself separate from the family | 153 | 56.3 |
| Not able to give sufficient time to personal care like eating food on time | 123 | 45.2 |
| Not able to get sufficient to time to manage routine activities like washing of cloths, cleaning, etc. | 81 | 29.8 |
| No friend circle/ no leisure time | 77 | 28.3 |
| Learned new skills for day-to-day life | 157 | 57.7 |
| Learned new skill for work / profession | 197 | 72.4 |
Table 3: Effect of COVID-19 on routine life of HCWs.
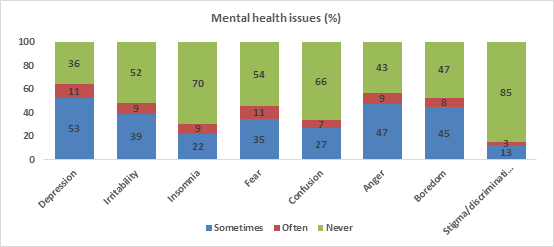
The myriad of challenges arising from COVID-19, both in personal and professional space, subjected the HCWs to go through a range of mental health issues manifesting as emotional distress and burnout, emotional fatigue, anxiety disorders, depression, insomnia, acute stress and post- traumatic stress disorders, and other psychological problems [26]. The current study shows that more than half of the HCWs experienced depression ‘sometimes’ followed by anger (47%), boredom (45%), irritability (39%) and fear (35%) (Figure 2). Depression and fear were reported ‘often’ by 11% of the respondents while irritability and anger were reported by 9% each. 85% respondents had never experienced ‘stigma and discrimination’ followed by insomnia (70%), confusion (66%), fear (54%) and irritability (52%). These findings show the pervasive impact of COVID-19 pandemic on HCWs’ mental well-being and sheds light on the complex interplay between various circumstances faced by HCWs that impact their mental well-being.
Mental health issues in HCWs when analyzed against the background characteristics, age and type of residence, were found to be significantly associated. With increasing age proportion of HCWs who ‘Never’ experienced any symptom rises from 9.52% in the 20–24year age group to 24.32% in those aged >35 years (Table 4). Also, the proportion of ‘Never’ was higher among those who were living on rent or in their own house in comparison to those who were living in staff residences provisioned by the government. Among other characteristics, no significant relationship was observed, but the proportion of HCWs who had ‘Never’ experienced any fear was higher among HCWs who were male, married and working in their home districts.
58% of the HCWs reported any one of the mental health issues ‘Sometime’, 32% ‘Often’ and 9.6% did not experience any issues at all. There were variations in experiencing mental health issues among the HCWs; the HCWs who were engaged in field activities, 92.4% of ANMs, 92.5% of Staff Nurses and 100% of the LHVs experienced mental health issues more frequently than those who worked primarily in facility setting such as lab technicians (80%) and medical officers (81.8%), pharmacists being an exception (91%). This could be because LHVs, ANMs and staff nurses were mostly engaged in surveillance, quarantine, contact tracing contacts and counseling in the field. In summary it can be concluded that age and residence type stand out as the key influencers along with nature of work that determine the occurrence and frequency of considered mental health issues amongst various cadres of health care providers that were interviewed in this study.
| Background Characteristics | Any Mental health symptoms | ||
|---|---|---|---|
| Never# | Sometime## | Often### | |
| Age ** | |||
| 20-24 | 9.5 | 59.5 | 31.0 |
| 25-30 | 5.2 | 62.5 | 32.3 |
| 31-35 | 10.5 | 54.4 | 35.1 |
| >35 | 24.3 | 46 | 29.7 |
| Pearson Chi2 (6) | 13.044 | Probability=0.042 | |
| Male | 12.9 | 56 | 31.0 |
| Female | 7.1 | 59.6 | 33.3 |
| Marital | |||
| Married | 11.1 | 57.0 | 31.9 |
| Unmarried | 5.2 | 62.1 | 32.7 |
| Separated/divorce/other | 0.0 | 57.1 | 42.9 |
| Place of posting | |||
| Rural PHC | 9.2 | 59.7 | 31.1 |
| Urban PHC | 10.6 | 53.0 | 36.4 |
| Type of residence | |||
| Government sanctioned staff residences | 6.3 | 60.9 | 32.8 |
| Rented accommodation | 12.2 | 63.4 | 24.4 |
| Own residence | 7.8 | 46.8 | 45.5 |
| Pearson Chi2 (4) | 11.002 | Probability=0.027 | |
| Work place in home district | |||
| No | 8.4 | 63.4 | 28.2 |
| Yes | 10.6 | 53.2 | 36.2 |
| Staff | |||
| MO IC | 18.2 | 50.1 | 31.8 |
| Pharmacist | 9.1 | 54.5 | 36.4 |
| LHV | 0.0 | 68.7 | 31.3 |
| Staff Nurse | 7.5 | 64.2 | 28.3 |
| ANM | 7.6 | 60.0 | 32.4 |
| Lab Technician | 20.0 | 55.0 | 25.0 |
| MPW | 11.8 | 47.1 | 41.2 |
| Total | 9.6 | 58.1 | 32.3 |
Table 4: Any mental health symptom by background characteristics of HCWs (N=272). #Never refers to those who never experienced an
Table 4: Any mental health symptom by background characteristics of HCWs (N=272). #Never refers to those who never experienced any mental health issue ##Often refers to those who has experienced atleast one mental health condition ###Sometimes refer to those who have experienced atleast one mental health condition but have not experienced any mental health condition often To adopt safe behaviors and maintain physical wellbeing during the pandemic, HCWs employed range of coping strategies [27], which encompass activities such as engaging in leisurely pursuits such as watch TV, read books, and sufficient sleep [4] to manage their negative emotions. In addition to personal coping mechanisms, HCWs also implemented proactive measures that played a pivotal role in the overall response to the pandemic. These measures include adequate planning, timely sharing of information, provisioning of PPE kits, along with training [28].
In our study many of the HCWs were practicing one or more types of coping mechanisms like exercise, meditation and yoga to manage the stress. On careful examination of data, it becomes apparent that a considerable 44.9% exercised, followed by 29.4% practicing yoga and 22.8% practicing meditation (Table 5). An analysis by health care provider type indicates that MPWs demonstrated the highest tendency to engage in daily exercise (67.7%), followed by pharmacists (63.6%); nurses (41.5%) and ANMs (32.4%) showed low levels of participation in physical exercise, medication and yoga. This could be because ANMs were mostly in the field and also had to undertake household chores. However, the stress management activities like exercise, yoga, meditation etc. were found useful for mental wellbeing [29, 30, 31]. Almost all the staff reported that they tried to get sufficient sleep to reduce stress. Many HWCs elicited about taking hot water bath, drinking hot water and taking green leafy vegetables to improve health.
| Staff | Every Day | Meditation | Yoga |
|---|---|---|---|
| Exercise (%) | (%) | (%) | |
| MOIC | 50 | 22.7 | 31.8 |
| Pharmacist | 63.6 | 45.5 | 36.4 |
| LHV | 50 | 25 | 25 |
| Staff Nurse | 41.5 | 20.8 | 26.4 |
| ANM | 32.4 | 15.2 | 28.6 |
| Lab Technician | 50 | 40 | 40 |
| MPW | 67.7 | 23.5 | 26.5 |
| Total | 44.9 | 22.8 | 29.4 |
Table 5: Yoga and exercise by designation among medical and paramedical staff. (N=272).
Discussion
The HCWs were engaged in an array of critical COVID-19 prevention and treatment activities, which included triaging of patients with symptoms of influenza like illness (ILI), referral, community surveillance, tracing the contacts of COVID-19 infected patients, door-to-door surveys, assisting the testing teams, monitoring home quarantined patients, arranging ambulance services for critical patients, setting- up teleconsultations, counseling services and awareness generation [32]. HCWs across all tiers of the healthcare system were engaged in similar activities. However, the workload on healthcare workers of primary healthcare facilities underwent a staggering surge. They had to navigate through these tasks while continuing to do their usual jobs within the framework of national health programs. The study illustrates that HCWs of primary healthcare facilities faced tough and overwhelming times, as well as distinctive mental health challenges because of COVID-19. It is reasonable to assume that HCWs were more informed than the general population, but still working in COVID-19 led to sufficient fear and anxiety and stress among them. Interestingly, HCWs who were living in their own house, showed mental health issues more often than those who occupied government provisioned residences or in rented housing. Likewise, the HCWs who were deployed in their home district expressed more mental health issues than those who were posted in districts other than their home district. This suggests that the HCWs working in proximity to their families harbored heightened concerns, potentially stemming from the fear of transmitting the infection to their family members. Working in the challenging environment induced anxiety among healthcare workers particularly concerning the safety of their aged parents and children.
This study shows the need to support HCWs who are comparatively young, which may be due to their lack of experience, as prevalence of mental issues was inversely correlated with age. In case of HCWs of rural and urban facilities, the difference in proportion of staff who had never experienced mental health issues were not very acute but a higher proportion of HCWs at urban facilities had mental health issues more often, which could be associated with overwhelming of their facilities (PHCs) in the urban areas. Also, early on during the pandemic, the infection was spreading in urban areas at a higher pace, coinciding with timing of the study.
Conclusion
COVID-19 showed us the vulnerabilities in mental health of healthcare providers working in primary healthcare institutions and the pressing need to address them. Although this assessment was conducted with a small number of healthcare providers in a limited geographical area, its findings show the urgency to create institutional support mechanisms for HCWs to prepare them for similar public health emergencies in future. HCWs had shown that despite all the formidable challenges, they toiled hard and extended unceasing care to the patients.
Acknowledgement
We are thankful to the various stakeholders and respondents who participated in this research study. We also extend our thanks to our funders- Lords Education and Health Society (LEHS).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
-
Nichols C, Jalali F, Fischer H (2022) The “Corona Warriors”? Community health workers in the governance of India’s COVID-19 response. Polit Geogr 99: 102770.
-
(2021) Health and Care Worker Deaths during COVID-19. WHO.
-
Sahashi Y, Endo H, Sugimoto T, Nabeta T, Nishizaki K, et al. (2021) Worries and concerns among healthcare workers during the coronavirus 2019 pandemic: A web-based cross-sectional survey. Humanit Soc Sci Commun 8: 41.
-
Ali A, Kumar S (2023) Indian Healthcare Workers’ Issues, Challenges, and Coping Strategies during the COVID-19 Pandemic: A Cross-Sectional Study. Int J Environ Res Public Health 20(4): 3661.
-
Mascarenhas A (2021) IMA flags 800 doctor deaths in second wave. The Indian Express.
-
Ghosh S, Moledina N, Hasan MM, Jain S, Ghosh A (2021) Colossal challenges to healthcare workers combating the second wave of coronavirus disease 2019 (COVID-19) in India. Infect Control Hosp Epidemiol.
-
Patil P, Taneja S (2021) Medicine or martyrdom? A peek into the rising violence against doctors during times of COVID 19. J Family Med Prim Care 10(8): 2732-2734.
-
(2020) Covid-19: 87k healthcare workers infected, 573 dead; 74% cases from six states. Times of India.
-
Jayanth AS (2022) 974 health workers died of COVID-19: Centre. The Hindu.
-
Iyengar KP, Ish P, Upadhyaya GK, Malhotra N, Vaishya R, et al. (2020) COVID-19 and mortality in doctors. Diabetes Metab Syndr 14(6): 1743-1746.
-
Lin S, Deng X, Ryan I, Zhang K, Zhang W, et al. (2022) COVID-19 Symptoms and Deaths among Healthcare Workers, United States. Emerg Infect Dis 28(8): 1624- 1641.
-
Mutambudzi M, Niedwiedz C, Macdonald EB, Leyland A, Mair F, et al. (2020) Occupation and risk of severe COVID-19: prospective cohort study of 120 075 UK Biobank participants. Occup Environ Med 78(5): 307- 314.
-
Alrawashdeh HM, Al-Tammemi AB, Alzawahreh MK, Al-Tamimi A, Elkholy M, et al. (2021) Occupational burnout and job satisfaction among physicians in times of COVID-19 crisis: a convergent parallel mixed-method study. BMC Public Health 21(1): 811.
-
Gupta N, Dhamija S, Patil J, Chaudhari B (2021) Impact of COVID-19 pandemic on healthcare workers. Ind Psychiatry J 30(1): S282-S284.
-
Benfante A, Di Tella M, Romeo A, Castelli L (2020) Traumatic Stress in Healthcare Workers during COVID-19 Pandemic: A Review of the Immediate Impact. Front Psychol 11: 569935.
-
Mohsin SF, Agwan MA, Shaikh S, Alsuwaydani ZA, AlSuwaydani SA (2021) COVID-19: Fear and Anxiety among Healthcare Workers in Saudi Arabia. A Cross- Sectional Study. Inquiry 58: 469580211025225.
-
Khanal P, Paudel K, Devkota N, Dahal M, Mishra SR, et al. (2021) Corona virus fear among health workers during the early phase of pandemic response in Nepal: A web- based cross-sectional study. PLOS Glob Public Health 1(12): e0000083.
-
Kumar J, Katto MS, Siddiqui AA, Sahito B, Ahmed B, et al. (2020) Predictive Factors Associated With Fear Faced by Healthcare Workers During COVID-19 Pandemic: A Questionnaire-Based Study. Cureus 12(8): e9741.
-
Sahebi A, Nejati-Zarnaqi B, Moayedi S, Yousefi K, Torres M, et al. (2021) The prevalence of anxiety and depression among healthcare workers during the COVID-19 pandemic: An umbrella review of meta-analyses. Prog Neuropsychopharmacol Biol Psychiatry 107: 110247.
-
Hassannia L, Taghizadeh F, Moosazadeh M, Zarghami M, Taghizadeh H, et al. (2021) Anxiety and Depression in Health Workers and General Population During COVID-19 in IRAN: A Cross-Sectional Study. Neuropsychopharmacol Rep 41(1): 40-49.
-
Parthasarathy R, Ts J, K T, Murthy P (2021) Mental health issues among health care workers during the COVID-19 pandemic - A study from India. Asian J Psychiatr 58: 102626.
-
(2020) Covid-19: Indian government vows to protect healthcare workers from violence amid rising cases. BMJ 369: m1631.
-
Bhatti OA, Rauf H, Aziz N, Martins RS, Khan JA (2021) Violence against Healthcare Workers during the COVID-19 Pandemic: A Review of Incidents from a Lower-Middle-Income Country. Ann Glob Health 87(1): 41.
-
Giannis D, Geropoulos G, Matenoglou E, Moris D (2021) Impact of coronavirus disease 2019 on healthcare workers: beyond the risk of exposure. Postgrad Med J 97(1147): 326-328.
-
Shreffler J, Petrey J, Huecker M (2020) The Impact of COVID-19 on Healthcare Worker Wellness: A Scoping Review. West J Emerg Med 21(5): 1059-1066.
-
Gupta S, Sahoo S (2020) Pandemic and mental health of the front-line healthcare workers: a review and implications in the Indian context amidst COVID-19. Gen Psychiatr 33(5): e100284.
-
Singh J, Sood M, Chadda RK, Singh V, Kattula D (2021) Mental health issues and coping among health care workers during COVID19 pandemic: Indian perspective. Asian J Psychiatr 61: 102685.
-
Meena J, Dhiman S, Sharma R, Kumari K, Singhal S, et al. (2022) The Impact of the COVID-19 Pandemic on the Psychological Well-being of Healthcare Workers in Obstetrics and Gynaecology: An Observational Study at an Apex Institute. Cureus 14(4): e24040.
-
Nagarathna R, Anand A, Rain M, Srivastava V, Sivapuram MS, et al. (2021) Yoga Practice Is Beneficial for Maintaining Healthy Lifestyle and Endurance Under Restrictions and Stress Imposed by Lockdown During COVID-19 Pandemic. Front Psychiatry 12: 613762.
-
Priyanka, Rasania SK (2021) A cross--sectional study of mental wellbeing with practice of yoga and meditation during COVID-19 pandemic. J Family Med Prim Care 10(4): 1576-1581.
-
Kanchibhotla D, Saisudha B, Ramrakhyani S, Mehta DH (2021) Impact of a Yogic Breathing Technique on the Well-Being of Healthcare Professionals During the COVID-19 Pandemic. Glob Adv Health Med 10: 2164956120982956.
-
(2021) Government of India Ministry of Health and Family Welfare, SOP on COVID-19 Containment & Management in Peri-urban, Rural & Tribal areas.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda