Prioritize Placating Panicky Parents of Paediatric Pyrexial Seizure
A febrile seizure is a convulsion in a toddler or a child that's caused by a fever, from an explicit or implicit infection. Febrile seizures occur in young, healthy children who have normal development and haven't had any neurological symptoms before. Febrile seizures are common, occurring in up to 5% of children in the United States and up to 10% in India. Frequently perceived by caregivers as a life-threatening event, results in panic even among young, educated parents and accounts for emergency department visits and hospital admissions. It is not clear why some children have a febrile seizure following fever due to viral or bacterial infections, but they do occur due to abnormal increased electrical activity in the brain. Fortunately, febrile seizures are usually harmless, lasting for a few minutes, and don’t signify any serious health problem. The Primary Care Physician/ Provider (PCP) must be able to address young parents’ concerns as the first Pyrexial Seizure of a young infant or even a toddler, as they become panicky and calming them down is equally important as much as the treatment of the child. Most common precipitating cause for fever in febrile seizures are Upper respiratory infection (URI), Acute gastroenteritis (AGE), and Urinary tract infections (UTI). The causative organisms are usually viruses (RSV, Influenza, SARC-V 2, Roseola Virus) and Bacteria. However, the development of childhood vaccines over the past several decades has led to a significant reduction in childhood bacterial meningitis, whooping cough, Diphtheria etc. but streptococcus pneumonia and staphylococcus aureus bacteria with no vaccines are the common causes for hyperpyrexia. Most hospital studies indicate that about 15% cases prove positive for blood culture and another 7% are positive for urine culture. Management of Pyrexial seizure involves using Paracetamol and or Ibuprofen syrup or tablets every 3-4 hours and Diazepam if the seizures or long lasting or repeated. Bactrim (Sulfamethoxazole 40mg/Kg body weight and Trimethoprim 8mg/Kg body weight) suspension divided in 2 doses is given each day for 5 days for urinary infections. Material and Methods: This article is based on distant counselling the parents and managing two Fever Seizure cases one a girl of 6 years in Belgaum, Karnataka India and another a toddler of 17 months in San Jose, SFO, USA both my grandchildren in October 2023. The girl case was poorly investigated, and unnecessary broad-spectrum antibiotics given initially and, in the repeat attack, were administered standard Bactrim antibiotic. The boy in San Jose was investigated with 20 panels of pathogens in the first 4hours of emergency consultation and managed with only Paracetamol and Ibuprofen, no antibiotic.
Introduction
A Paediatric Pyrexial Seizure (PPS) or febrile seizure (FS) is a convulsion in a toddler or a child that’s caused by a fever, due to an explicit or implicit infection. Febrile seizures occur in young, healthy children who have normal development and haven’t had any neurological symptoms before. Medical fraternity defines age-related development periods as: i) newborn (ages 0–3 months); ii) infant (ages 3 months - 1 year); iii) toddler (ages 1–3 years); iv) preschooler (ages 3 – 6 years); v) school-aged child (ages 6–11 years); vi) teens (ages 12–17 years). First, parents and primary Crae Provider must try to differentiate FS/PPS from Rigors. A rigor is a violent and uncontrollable shivering, sometimes with mild confusion, but the patient remains conscious and can respond to you. A seizure exhibits jerky shiver-like movements but are not aware of their surroundings and do not respond to you.
It is not clear why some children have a febrile seizure. It usually occurs when the child develops fever because of viral or bacterial infections such as common cold or flu-like illness, ear infection, or urinary tract infection. Some children may have one or more affected family members with febrile seizures or epilepsy. Convulsion occurs due to abnormal increased electrical activity in the brain. Usually, the brain systematically generates electric currents and transmits it through a network of nerves in a well-coordinated fashion to carry out various body functions. During a febrile convulsion, due to the rapid rise of fever, sudden and dysregulated increase in electric discharges in the brain lead to unconsciousness with shaking of the limbs [1]. A higher- than-normal body temperature, even a low-grade fever can trigger a febrile seizure in toddlers. Febrile seizures most often occur within 24 hours of the onset of a fever and can be the first sign that a child is ill. It is frightening to parents especially moms when their child has the first febrile seizure. Therefore, it is important for the PCP to calm them down and re-assure them that febrile seizures are usually harmless, last for a few minutes, and don’t signify any serious health problem. Parents must be educated to help the child to be safe during a febrile seizure and by comforting afterwards. A thorough assessment of the child as soon as possible after a febrile seizure is advised to rule out serious causes of Fever. Of late viral fevers (Adenoviruses, Influenza Virus, and Respiratory Syncytial Virus (RSV) Roseola Virus) are common in toddlers and bacterial lower urinary tract infections or parasitic infections in school-aged children are responsible for seizures [2]. Currently outbreaks of Roseola virus are reported in USA.
Most common precipitating cause for fever in febrile seizures are Upper respiratory tract infection, Acute gastroenteritis, and Urinary tract infections. 15% cases were positive for blood culture, common bacteria being streptococcus pneumonia and staphylococcus aureus while 7% were positive for urine culture.
The rigors with malaria in tropical countries are a manifestation of cerebral dysfunction rather than simple febrile in Seizure. All forms of cerebral dysfunction in malaria must be managed as clinical manifestations of cerebral malaria.
This article is outcome of digital or distant counselling and managing two Fever Seizure cases one a girl of 9 years in Belgaum, India and another a toddler of 18 months in San Jose, SFO, USA both my grandchildren in October 2023.
Case Reports
Case 1: Anagha 6 years Belagavi, Karnataka
Sixth October 2023, Ms Laxmi mother of Anagha called me around midnight reporting that their daughter was having fever for last 2 days and after Basic blood tests was prescribed a broad-spectrum antibiotic (Cefixime 200 MG twice a day) and paracetamol tablet every 6 hours. In the midnight the child had high temperature of 1040FF despite giving antibiotics and Paracetamol and developed seizures which made them to call me as the local doctor was not available. A compete Hemogram done showed i) Hb%-10.3 (NV=12-15 gm %), Packed Cell volume -29% (NV-36-45%), MCV-59.2 fL (NV-80-99fL) MCH-21 Pg (NV 25-33Pg), RDW SD-27.8 fL (NV-35-56 fL), PDW-8.2% (NV-10-15%), P-LCR- 2.8 (NV-13-43%), all other biomarkers were within normal value range. CRP was 4.9 mg/L Negative (NV—6 mg/L) ruling out bacterial infections. WIDAL Test for Q, H, AH and BH were also negative. Since by that time only one dose of antibiotic was given, I advised them not to worry and give Tepid sponging. They were advised to use lukewarm water [90 - 95 °F] and not cold water, or ice, Sponge for 20 to 30 minutes and stop once the child stops shivering. After 50 minutes they called back reporting that shivering had stopped, and temperature had come down to 1010F.
On 7 October entire day the temperature was around 100°F, but around by evening the temperature shot up to 103°F and she was having seizures. After another Paracetamol tablet it came down to 101°F within 45 minutes and shivering stopped. The local paediatrician asked them to admit the child to the hospital. That’s when the parents called me. Another rise in temperature to 102°F around 0500hrs on 8th with no seizures declined after another dose of paracetamol tablet. Parents reported that whenever temperature went above 102°F she got seizures. A detailed history revealed increased frequency in urination. She was advised for adequate rehydration with frequent fluids and paracetamol every 4 hours or if the temperature crossed 101°F at any time with hourly monitoring of body temperature.
On 8th October after the early morning rise the girl did not have high temperature and by night, she was almost normal and playing. Advised to continue the antibiotic for 5 days and use Paracetamol only if fever touched 101°F. The child was fine following days until 11th October. They travelled by Car on 11 October to a temple about 150Kms.
On 15th the child developed fever again. Temperature rose to 103.2°F but no rigours this time. I put the girl on Bactrim (Sulfamethoxazole 40mg/Kg body weight and Trimethoprim 8mg/Kg body weight combination suspension in 24 hours divided in 2 doses) a better Urinary antibiotic for Indian children). After 4 doses the temperature cam to Norma ranges by 17 October 2023 and continues to be normal even today the 20th of October 2023.
Lesson learned 1. The Paediatricians must avoid using broad spectrum antibiotics and unnecessary investigations (Widal on day 2/3, CRP etc) with specific provisional diagnosis. 2. If locally available Respiratory Viral Panel Tests must be used for diagnosis. 3.Avoid admission advise unless there are reasons like i) Age at the onset before 18 months ii) Duration of fever <1 hour before the seizure occurs iii) The seizure occurs at a lower temperature, iv) One or more of the parents and siblings have history of a febrile seizure.
Case 2: Saahil Age 17 Months San Jose, SFO, USA
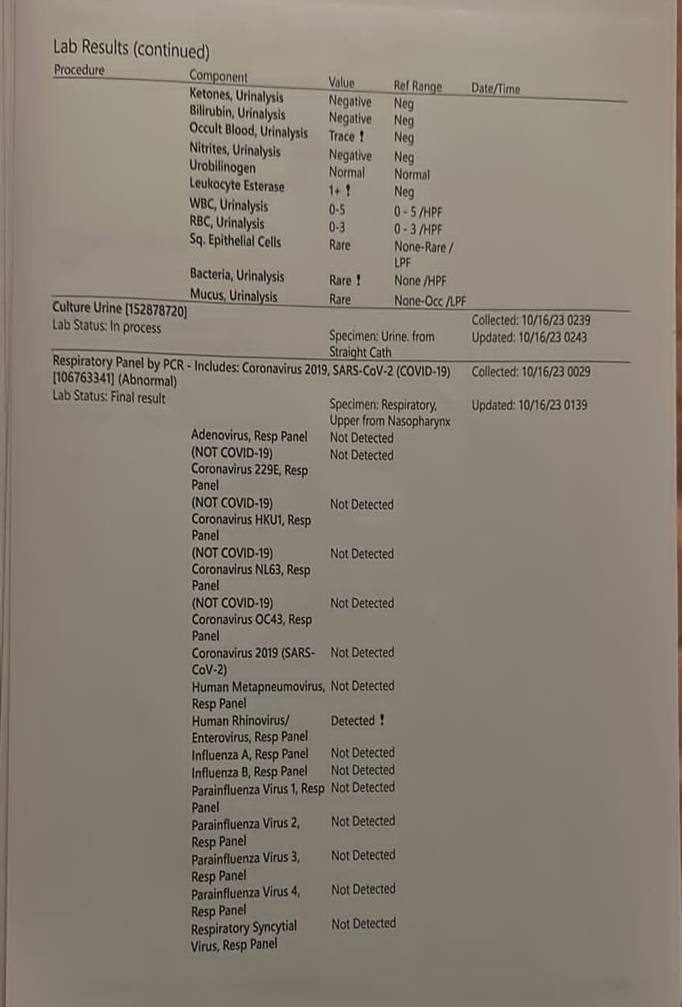
It was around 1130 hrs India- on last Tuesday 16 October 2023, I get a call from my son in San Jose (around 2300 hrs local time Monday 15 October 23). My daughter in law (DIL) was panicky, and seeing her panic my son was also concerned as their younger son Saahil was having seizures first time since birth following a temperature of 1010 F and wondering if an emergency consultation needs to be sought. A video look (Facetime), the child was having seizure with vigorous shaking of Right hand & legs and was semi- conscious. I consoled and counselled them not to panic and give Tylenol available at home. However, our DIL was crying, and both were not in a mood to listen and decided to take the child for an emergency consultation calling for an ambulance. The Mountain View emergency room doctor recorded vital signs at 23:57 hrs on 15/ 10/23 as Temperature= 98.9°F, Pulse= 124/minute, Respiratory Rate = 21 /minute, Spo2 =99% & BP= 117/82. Laboratory Test done – included multiple (20) Respiratory Panels by PCR which included 5 Respiratory Panels (Not Covid 19), Corona Virus 2019 Panel, (SARS- Cov -2), Human Rhinovirus/ Enterovirus Panel, Human Metapneumo virus Respiratory Panel, Influenza A, B, Respiratory Panel, Para=Influenza Type 1,2,3,4 Respiratory Panels and Respiratory Syncytial Virus Panel. Other Respiratory Panels included Bordetella Pertussis, Chlamydophila Pneumoniae, Mycoplasma Pneumoniae. All Respiratory Panels were Negative except Human Rhinovirus / Enterovirus Panel which was positive.
Urine analysis with Microscopy at 0239 on 16 /01/23, showed no protein or Sugar, Specific gravity 1.019 (NV- 1.001-1.035), PH= 5.5 (NV= 5-8). The tests for Ketone bodies, Bilirubin, Occult blood, Nitrogen and Urobilinogen were negative. Microscopy showed WBC and RBCs within normal ranges of 0-3. Similarly, Urine analysis for Bacterial, Mucous cells and epithelial cell analysis were also in normal ranges. Urine sample was also collected from straight catheter for culture. With a provisional diagnosis of Viral fever with Seizures. The child was administered Tylenol - 4.8 ml (160 mg) at 23:21 hrs and Ibuprofen 5.1 ml (100 mg), at 12:23 on 16/10/23. With some advice to repeat alternately every 4 hours as needed for fever management. They were advised to go to a Paediatrician in the next 3 days for Recheck (Figures 1-3).
A respiratory pathogens (RP) panel checks for pathogens (virus, bacteria, or other organism) that cause an illness in the respiratory tract, made up of parts of the body involved in breathing. Results are available in minutes if analysed onsite as seen in Saahil’s case. Results may take 1 to 3 days or longer with test processing delays if sent to an outside lab. As we see USA has the luxury Respiratory Pathogens Panel Test (Pathology Test) for about 20 Respiratory virus and bacterial panels PCR tests readily available. In India, these are available only in few large laboratories in metropolitan cities and in some medical College hospitals. The average cost of such Tests is in private sector is around INR 8000 (US$ 880).
After about an hour another call reported that the child was examined an emergency duty paediatrician and were told not to be panicky and advised for admitting the child to paediatric hospital for observations and investigations. Three hours later another call came to inform that all investigations ruled out urinary tract infections and suspected only viral fever (RSV?). The baby was discharged and came home around 0430 AM local time with and advised giving Tylenol to syrup every 4 hours, monitor recurrence of seizures and body temperature hourly.
On 18 October the child did not exhibit rise in temperature as he was on 4th hourly Tylenol was up and above playing. The fluid and food intake had decreased. Since 19 he was on
6th hourly Tylenol and on 20th 4th hourly Tylenol with neither temperature rise nor seizures. On 20 October the boy developed Roseola Rashes. The rashes completely vanished by 23 October 2023 and the child is completely recovered.
Discussions
Febrile seizures are seizures or convulsions that occur in young children. They are triggered by fever typically above 101 degrees Fahrenheit (38.3 degrees Celsius). Seizures may happen during illnesses such as a cold, the flu, or an ear infection. In some cases, a child may not have a fever at the time of the seizure but will develop one a few hours later. Most Parents fear that the child has epilepsy. Epilepsy involves repeat seizures that are not triggered by fever. Most febrile seizures last a minute or two. Yet some may only last a few seconds and others may last for more than 15 minutes. Even a first febrile seizure that is prolonged does not boost the risk of having more, as they are generally harmless on their own, but they do carry an increased risk of developing epilepsy. Febrile seizures are among the leading causes of Paediatric hospital admissions and affect almost 25% of all young children. Young children between the ages of about 6 months and 5 years old are the most likely to have febrile seizures. Children are at the greatest risk of having a febrile seizure at around 2 (1.5-3) years.
Population studies in Western Europe and the USA report a cumulative incidence of 2–5%. The incidence elsewhere in the world varies between 5–10% (India), 8.8% (Japan), and 14%. The incidence rates in India are comparable to those in the developed world. The Yelandur survey estimated the prevalence to be 3.28-5.71/1000 [3] whilst the more recent Uttarakhand survey [4] found a prevalence of 2.27 per 1000 population.
A hospital based prospective study in department of paediatrics, in Tiruppur, Tamil Nadu government hospital for a period of 6 months with children below 12 years, reported that out of a total of 150 patients (85 male & 65 female), 66 patients were below age of 3. Simple generalised seizures were found in about 38% patients within 12-24 hours of fever. In 90% of the cases aetiology was an infection- commonest being Acute Respiratory Infection= 96, Acute Gastro- Enteritis= 24, Malaria = 5, Otitis Media =4 and Enteric Fever= 8. For most of the kids it was first episode (125) followed by 2nd episode (20), 3rd episode (4) and 4th episode (1) [5]. Gogoi A, et al. Tauhid Iqbali many studies found that generalized seizure is most common type of seizure Renuka D, et al. [6]. Reported peak age of incidence in 1-2 years and Hussain S, et al. [7] reported kids having seizure in 13-24 hours since onset of fever [6]. Most of the Indian studies (75%) indicate rampant use of antibiotics for seizure, while western world with available Pathogen panel Tests uses antibiotics in less than one third of cases.
A child having a febrile seizure shakes all over and may lose consciousness. Alternately child may get very stiff or twitch in just one area of the body. Key symptoms before the seizure include i) Have a fever higher than 100.4 F (38.0 C) in toddlers, and 103° -104°F in school aged children over, ii) Lose consciousness iii) Shake or jerk the arms and legs [1, 2].
Febrile seizures are categorised as
- Simple febrile seizures: The most common type lasts from a few seconds to 15 minutes. They do not recur within a 24-hour period and are not specific to one part of the body.
- Complex febrile seizures: This type lasts longer than 15 minutes, occurs more than once within 24 hours or is confined to one side of your child’s body [2]. Parents need to take emergency consultation if they observe any of the features like: if the seizure lasts longer than five minutes or is accompanied by Vomiting, a stiff neck, breathing problems, or drowsiness [2].
| Simple FS | Complex FS | |
|---|---|---|
| (all the following) | (any of the following) | |
| Age | 6 months to 5 years | 6 months to 5 years but may be younger age |
| Types of seizures | Generalized | Focal |
| Duration of seizure | Less than 15 min | Prolonged, (≥15 min) |
| Occurrence | Once in 24 h | Recurs within 24 h |
| Associated neurological condition | No previous neurologic problem | Developmental delay or focal neurologic signs |
| Post-seizure complication | No postictal pathology | Todd’s paresis may be present, seizure may persist for>30 min |
Table 1: Characteristics of simple versus complex Febrile Seizures [8].
Causes: The fevers that trigger febrile seizures are usually caused by a viral infection, and less commonly by a bacterial infection. The five common infections associated with febrile convulsions are Adenoviruses, Chickenpox and Influenza, enterovirus, and parainfluenza viruses, Roseola Virus, and middle ear infections (otitis media) [1, 2].
Post-Vaccination Seizures: The risk of febrile seizures may increase after some childhood vaccinations. These include the diphtheria, tetanus and pertussis vaccine and the measles-mumps-rubella vaccine. Some children develop a low-grade fever after a vaccination and it is the fever, not the vaccine, that causes the seizure.
Pathogenesis
The pathogenesis of FS as known today from human studies is multifactorial and debatable. Neuronal hyper excitability, developed during inflammatory responses that occur in the initial stages of a fever, provokes seizures. However, the specific role of each cytokine is undefined in terms of the connection between systemic or local inflammation and the central nervous system, and the mechanisms by which cytokines increase neuronal excitability still are unclear. In contrast, the cause of fever in most children with FS is usually mild seasonally prevalent respiratory viruses (e.g., rhinovirus, influenza virus, adenovirus, and enter virus) of seasonal community- acquired respiratory tract infections and therefore, vigorous efforts to identify the causative pathogen of fever in children with FS are not made globally. Most children with FS have benign outcomes. A few cases of complex FS, febrile status epilepticus, consecutive afebrile seizures, and the presence of neurodevelopmental disabilities may require further genetic and neurologic evaluations.
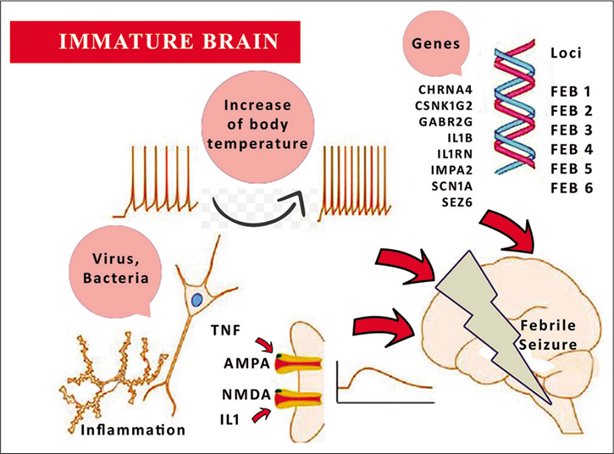
Genetic Predisposition: Genetic predisposition to febrile seizures is well known, though the exact mode of inheritance is not known in most cases. There are many genes that are associated with a febrile seizure and are responsible to play a role in neuronal hyper excitability that participate in neuronal excitation. The facts know are summarised as:
- Among first-degree relatives of children with febrile convulsion, 10–20% of parents and siblings may have a febrile seizure.
- It is considered that there is a higher chance recurrence episode of febrile seizure if one or more of the family members also have a febrile seizure.
- Genetic epilepsy with febrile seizures plus (GEFS+): Febrile seizure is not epilepsy, GFFS+ children may have seizures even without a fever.
They have different types of seizures like head drops, prolonged episodes of starring, or unresponsiveness.
Roseola is one of the very common mild viral contagious illnesses that affect children aged between six months and three years. Roseola is caused by a type of herpes virus that enters the body through the nose and mouth. It is spread when a child breathes in droplets that contain the virus after an infected person coughs, sneezes, talks, or laughs. The fine, raised, red skin rash and high temperature can last from a few hours to three to five days. The rash can sometimes be confused with measles or rubella. Currently there are outbreaks reported in USA.
Differential Diagnosis
For simple febrile seizures, most often the diagnosis is clinical, no tests should be performed unless other symptoms indicate it. First, parents and primary Crae Provider must try to differentiate FS/PPS from Rigors. A rigor is a violent and uncontrollable shivering, sometimes with mild confusion, but the patient remains conscious and can respond to you. A seizure exhibits jerky shiver-like movements, but patients are not aware of their surroundings and do not respond to you. Complex febrile seizures are often a diagnosis of exclusion. A lumbar puncture is indicated if there have been no Hib or pneumococcal vaccinations, and to rule out meningitis or other intracranial infection if there is clinical suspicion [7]. Blood sugar assessment helps in distinguishing the Pyrexia seizure from hyperglycaemia-related seizures. There is no need for an MRI brain or EEG in a child with simple febrile seizures, even if they are multiple. However, children with prolonged febrile seizure, complex febrile seizure, suspected GEFS+ MRI brain, and EEG may be advised.
Full blood count, serum electrolytes, calcium, magnesium, phosphorous and blood glucose levels are not routinely recommended for evaluating febrile seizures. Simple Urine microscopy may be suggested to identify primary cause of infection. If available Respiratory Pathogen Panel of PCR tests are helpful in diagnosis within a few hours.
Chances of Recurrences of Febrile Seizure
Roughly one thirds to 40% of children with febrile seizures will have a recurrence of seizure. The chances of having recurrent episode are higher among those with one or more of the
- Age at the onset before 18 months
- Duration of fever <1 hour before the seizure occurs.
- The seizure occurs at a lower temperature,
- One or more of the parents and siblings with a febrile seizure.
Impact of Febrile Seizure
Febrile convulsions do not affect intelligence or school performance.
Children with prolonged febrile seizure episodes who are prone to future epilepsy may have mild difficulties in their school performance. The risk of epilepsy with simple febrile seizures is 1%, like the risk of developing epilepsy in the general population.
The risk of future epilepsy may increase among those with a complex febrile seizure.
Management of Pyrexial Seizures: Role of Tepid /warm sponging:
There are differences of opinion in clinical practice field and research studies: Some studies do report advantage of tepid sponging with Lukewarm water including an Indian study (12) as was seen in our second case. However, a metanalysis in UK reported no added value.
Before being given Tepid Sponge all children under five experience high temperatures (100%) of 12 respondents, after being given Tepid Sponge one time gift, the temperature of all respondents became normal (100%). Statistical test results showed a significant effect of giving Tepid Sponge to changes in body temperature with p=0.000 (≤0.05) [9].
An India study observed that administration of tepid sponging and antipyretic drug resulted in rapid temperature reduction in the initial 15-30 minutes as compared to antipyretic drug alone; however, by the end of 2 hours both groups had reached the same degree of temperature [10].
A meta-analysis showed the need for re-verification of commonly used practice including the use of tepid massage and proper body temperature measurement [11].
Placating Panicky Parents
Parental anxiety and family dysfunction are the rule following a child’s first febrile seizure. Neither socioeconomic status nor the literacy or an understanding of the low risk of sequelae associated with febrile seizures is strongly predictive during and even two – 4 weeks following a seizure [12].
Whenever parents of a child have a febrile seizure, approach the primary care provider must plead them to stay calm, gently place your child on the floor or the ground, remove any nearby objects to prevent injuries, Place the child on his/her side to prevent choking. Advise to loosen any clothing around their head and neck and watch for signs of breathing problems, including a bluish colour in the lips and face.
What Should Parents Do Next Time if their Child Develops Febrile Seizure
i. If child develops a fever next time, record the temperature using a digital thermometer. ii. To prevent discomfort to the child, avoid overdressing, and choose clothes appropriate for the climatic condition. iii. Ensure adequate intake of fluids to prevent dehydration. iv. Tepid sponging at a temperature of 28–30°C may be considered. v. Paracetamol must be administered in the dosage recommended by a paediatrician. It decreases the temperature, and it will not reduce the risk of febrile seizures. vi. Rectal diazepam (0.5 mg/kg) or buccal (0.4-0.5 mg/kg) or intranasal (0.2 mg/kg) midazolam administration are effective in stopping an ongoing seizure. When intravenous provided for home use in patients with initial prolonged febrile seizure. vii Diazepam or Clobazam (a drug controls seizures) may be administered in selected cases for 2–3 days of fever as per recommendations.
Do’s Give paracetamol as prescribed by your doctor in the beginning of fever. If the child develops convulsions, place your child on the floor. Place the child on his/her side. Loosen the clothes near face and chest. Wipe off any secretions in the mouth. Remove any sharp objects near the child to avoid injury. Record the time the convulsion lasts. Record the event on a mobile phone so that you can show it your doctor. If the convulsion does not stop beyond 3–5 minutes, use midazolam nasal spray as advised by your doctor. Once the convulsions stop, use tepid sponging to reduce the fever.
Don’ts Do not panic. Do not feed anything or give any sips of water. Do not place any object in the mouth to prevent gagging. Do not pinch the nose of the child. Do not place any rod or metallic object in child’s hand who is convulsing, he may injure himself. Do not make him/her smell any unusual objects to abort the convulsions.
Conclusion
Worldwide, PPS is one of the most common age- dependent seizures. Of late Viral aetiology is more common than bacterial aetiology. PPS has genetic predisposition with a notable vulnerability of the developing brain to the effects of fever. Almost one-third of children have chances of recurrence, but they outgrowth the condition after 5 years of age. FS has slightly male preponderance. Low age at onset for FS has appeared a crucial predictor for an RFS. Simple FS are common, benign, and self-limited. Children with complex FS are at risk of developing epilepsy. FS usually does not cause intellectual or neurologic damage. SFS diagnosis is mostly clinical, urinary infections can be diagnosed simple urine microscopy. EEG and neuroimaging are not indicated in the routine evaluation of SFS. If available Respiratory Pathogen Panel Tests are useful in deciding the need to use antibiotics for management apart from Paracetamol, and Ibuprofen. Acute treatments are indicated when seizure is prolonged with oral or rectal Diazepam [13, 14].
References
-
Kaushik JS (2021) IAP guidelines for Parents to care children with Febrile Seizure. Indian Academy of Pediatrics.
-
(2023) Febrile seizure. Disease & Conditions.
-
Goel D, Agarwal A, Dhanai JS, Semval VD, Mehrotra V, et al. (2009) Comprehensive rural epilepsy surveillance programme in Uttarakhand state of India. Neurol India 57(3): 355-356.
-
Sawires R, Buttery J, Fahey M (2021) A Review of Febrile Seizures: Recent Advances in Understanding of Febrile Seizure Pathophysiology and Commonly Implicated Viral Triggers. Frontiers in Pediatrics 9.
-
Rjamathanky H, Varghese G, Keerthana KV, Sajimon L, Kannan BR, et al. (2020) A Prospective Study of Clinical, Etiological, and Demographical Profile of Children with Febrile Seizure in Secondary Care Hospital, Tirupur. International Journal of Recent Scientific Research 11(1): 36997-37001.
-
Renuka D, Surg Capt YAK, Surg Capt DSR (2015) Demographic, Clinical, & Laboratory Profile in Children with Febrile Seizures. Journal of Marine Medical Society 17(1): 44-47.
-
Hossain MM, Saha NC (2021) Clinical review of febrile seizure and updates. Karnataka Paediatric Journal 36(1): 3-12.
-
Mani KS, Rangan G, Srinivas HV, Kalyanasundaram S, Narendran S, et al. (1998) The Yelandur study: A community-based approach to epilepsy in rural South India. Seizure 7(4): 281-298.
-
Hendrawati, Elvira M (2019) Effect of Tepid Sponge on changes in body temperature in children under five who have fever in Dr. Achmad Mochtar Bukittinggi Hospital. Enfermeria Clinica 29(1): 91-93.
-
Thomas S, Vijaykumar C, Naik R, Moses PD, Antonisamy B (2009) Comparative effectiveness of tepid sponging and antipyretic drug versus only antipyretic drug in the management of fever among children: a randomized controlled trial. Indian Pediatr 46(2): 133-136.
-
Lim J, Kim J, Moon B, Kim G (2018) Tepid massage for febrile children: A systematic review and meta-analysis. Int J Nurs Pract 24(5): e12649.
-
Wirrell E, Turner T (2001) Parental anxiety and family disruption following a first febrile seizure in childhood. Paediatr Child Health 6(3): 139-143.
-
Hussain S, Tarar SH, Sabir MUD (2015) Febrile seizrues: demographic, clinical and etiological profile of children admitted with febrile seizures in a tertiary care hospital. Journal of the Pakistan Medical Association 65(9): 1008- 1010.
-
Han JY, Han SB (2023) Pathogenetic and etiologic considerations of febrile seizures. Clin Exp Pediatr 66(2): 46-53.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda