Feasibility and Safety of Performing Day-Surgery Medial Unicompartmental Robotic Prostheses in the Italian Health Care System
Study Purpose: Our study analyzes the feasibility and safety of robotic-assisted medial unicompartmental prostheses performed in day surgery compared to the current standard for a minimum of two nights in the rules of the Italian National Health System, which is mandatory for Diagnosis Related Groups reimbursement of ordinary hospitalization. Two groups of patients undergoing robotic-assisted medial unicompartmental prostheses were compared, of which one group in ordinary hospitalization and one group in day surgery. All patients from both groups underwent Robot-assisted medial unicompartmental prosthesis surgery (RIO® MAKO Stryker surgical corporation). The terms of comparison between the two groups regarding feasibility and safety were: any complications, any transfusions, hospital readmissions, and ER accesses for prosthesis-related reasons within 7 days and within 3 months after surgery. Pain preoperatively, at discharge, 3 months and 1 year after surgery was quantified by Verbal Rating Scale (0 to 4). Method: At the ASL Toscana Sudest in Arezzo, a total of 280 robot-assisted Unicompartmental Knee Arthroplasty (UKA) surgeries were performed during the study period (2014-2018), 259 of which were medial surgeries. The surgical team was always the same with oversight by two experienced senior surgeons. In this study, 259 cases of medial UKA were taken into consideration, while lateral or patellofemoral types were left out. Of the 259 medial UKA, 30 patients were consecutively operated on in day surgery by waiting list progression without any exclusion. The other 229 were all operated on as inpatients. We collected the ASA (American Society of Anesthesiologists) value data of the 30 patients under study namely 9 patients with ASA 1, 19 patients with ASA 2, and 2 patients with ASA 3. The average time for robotic surgery between the first 30 patients operated in 2014 and the last 30 operated in 2018 was studied to evaluate the trend in reduction of operational time by showing improvement in the learning curve of robotic technique with statistically significant result of P<0.01. We assessed patient satisfaction with the surgical course and outcomes of the 30 patients operated for UKA in day surgery, 3 and12 months after surgery with Likert scale quantifying satisfaction from 1 to 5: 1 totally dissatisfied, 2 dissatisfied, 3 neutral, 4 satisfied, 5 completely satisfied. Results: No readmission to the emergency room or ward occurred within 7 and 90 days after surgery for minor or major complications in the two groups. In view of the pain treatment protocol adopted for all UKA operated patients, the results regarding pain were not statistically significant between the two groups. Therefore, there were no differences according to the two types of hospitalization. After 3 and 12 months, 80% and 76% of patients, respectively, in the day-surgery operated group expressed themselves with value 4 and 5 on the Likert scale of satisfaction. Conclusions: In our study, we found no differences between the two groups of 30 patients operated in day surgery and the 229 operated in ordinary hospitalization in terms of transfusions, complications or hospital readmissions within 7 days, nor minor or major complications within 90 days after surgery. We found no statistically significant differences in the VRS pain scale by comparing the two groups; we found a high satisfaction index of the 30 patients undergoing day surgery. The pain scale, compared with values between the same group of 30 patients before surgery and after 3 and 12 months, showed a decrease such that it was statistically significant for P<0.05; an analogous result was obtained by comparing values between the same group of 229 patients for P<0.05. Our study demonstrates that robotic medial UKA can be safely performed in day surgery. Being able to perform this surgery under the assumptions and characteristics of day surgery organization means reduction of surgery costs, of waiting lists, of hospitalization risks, and of patient stress. The resulting organizational proposal is to authorize Italian health facilities to perform partial prosthesis surgery in day surgery with equal DRG reimbursement. Economic savings would result from this opportunity by offsetting the higher cost of the same robotic surgery.
Introduction
Day surgery (or one-day surgery) is an organizational modality that results in a single-day hospitalization excluding overnight. With this setting, surgeries can be performed under general, loco-regional or local anesthesia without risk of complications and without any necessary post-operative overnight follow-up. In Italy, the agreement of the State- Regions Conference of August 1, 2002, “Guidelines for day surgery activities” defines all the organizational and clinical parameters of this activity, which is theoretically possible in all public or accredited private hospitals of the Italian National Health System. There are many surgical procedures that can be organized according to this modality if they do not have an urgent nature and are not high risk according to the American Society of Anesthesiology classification [1]. The organizational clinical pathway consists mainly of 2 phases: a preoperative pathway with clinical, instrumental, and laboratory examinations, anesthesiologic examination, informed consent, and information about the clinical pathway. The second phase consists of hospital admission and surgery, which is always performed in the morning precisely so that adequate and proper postoperative monitoring of all clinical parameters and pain control can be carried out. In the evening, medical records are stored together with discharge of the patient with a letter containing all postoperative instructions.
In Italy at the Orthopaedic Trauma Center in Milan as early as the 1970s, pediatric orthopedics and hand surgery were beginning to be performed in day surgery, followed by knee arthroscopy in the 1980s. With the evolution of anesthesiological techniques, e.g., loco-regional nerve blocks, since the 2000s, other surgeries have been included and authorized with one-day hospitalization. This has happened not only because of the improvement and safety of surgical techniques but also because of better cost-effectiveness and control of healthcare expenditure. Not least, the mentality and habits of the population, especially of working patients, has changed. We will see an increasing demand for prosthetic surgery and joint performance in active, income-producing patients. Firstly, because of the gradual increase in the aging population with a corresponding increase in the demand for health, especially in terms of individual autonomy. Secondly, because more and more of the young-active population is affected by early arthrosis for which they seek joint surgery to remain professionally active. Day-surgery robotic single-compartment prosthesis represents the best health care response in working-active patients with advanced symptomatic arthrosis (Kellegren grade III and IV) of only one compartment of the knee, who no longer respond to conservative therapies [2].
The main factor that has limited the use of day surgery in the past is related to postoperative pain. A 2016 Italian study Campagna S, et al. [3] mentions that one of the key elements for safe home discharge of patients is knowledge of the postoperative course, including pain management. Postoperative pain and medication side effects form the core of the quality of the day surgery program.
In elective prosthetic surgery, epidural anesthesia or continuous peripheral nerve blocks have been used effectively in recent years to treat pain, although there is a need for specific expertise, they have high costs and possible side effects given the variety of drugs used [4]. One of the recent innovations is Local Infiltration Analgesia (LIA), which is especially used in Fast Track or fast recovery surgery. It promotes rapid mobilization and ambulation by limiting the consequences of prolonged immobility such as deep vein thrombosis.
The LIA technique was developed by L. Kohan and D. Kerr in Australia in the mid-2000s. It is part of a multimodal approach for post-surgical knee and hip pain control called “local infiltration analgesia”. It is based on the systematic infiltration of a mixture of ropivacaine, ketorolac, and adrenaline into the periprosthetic tissues to achieve satisfactory local pain control by nullifying the undesirable effects of systemic pain medications. Unlike femoral nerve blocks, the LIA technique permits immediate mobilization and ambulation and earlier discharge from the hospital [5]. LIA is simple, practical, safe, effective, and low cost. In several studies performed on the differences between LIA and continuous femoral nerve block Toftdahl K, et al. [6] or between LIA and continuous epidural infusion Andersen LØ, et al. [7], it was found that patients undergoing LIA had better pain control, better walking ability with lower risk of falls, and shorter hospital stay.
Since the beginning of 2017, the surgical team pertaining to the present study has started to use the LIA technique to speed up patient recovery and limit side effects. This has allowed patients to be discharged as soon as possible, in better clinical condition and especially with excellent pain management.
Compared with total knee replacement, unicompartmental knee replacement is more feasible in day surgery. This is because it is a minimally invasive surgery since, beyond the capsulotomy, preparation of the bone surface for the prosthetic implant is performed while leaving all knee ligaments intact. Conceptually, this is a real partial resurfacing prosthesis with reconstruction of the anatomy and constitutional alignment of the pre-arthritic knee.
All these concepts of UKA are particularly optimized by robotic surgery with MAKO RIO SYSTEM® platform.
The 2022 meta-analysis compares component placement accuracy, complications, survival, cost-effectiveness, learning curves, and Patient Related Outcomes (PROMs) in Mako robot-assisted vs manual medial unicompartmental knee arthroplasty. The conclusion of the meta-analysis was that the Mako Robot was associated with better accuracy of component positioning, but not in the Proms used namely the Knee Society Score scale (KSS) and Womac scale [8].
Foissey’s 2023 study also shows that in medial UKA surgery, robotic assistance results in better accuracy than manual technique regarding tibial implant placement, alignment of the limbs, and joint line restoration, which are all elements that favor the robotic group for implant survival at mid-term follow-up [9].
The robotic technique enables an extremely precise planning of the prosthesis on CT images by considering each patient’s specific anatomy, ligamentous balance of the joint, cartilage thickness, orientation, sliding, and connection between prosthetic components. The robotic arm makes it possible to reproduce on the patient what the surgeon has planned with extreme precision on the software by eliminating any manual error. The best and easiest alignment and positioning of prosthesis components permits a significant reduction in the amount of bone removed during surgery and in the amount of blood lost. In addition to these aspects, which are of considerable importance for operative management, there are also benefits in postoperative management, thanks to an important decrease in pain that enables the implementation of an almost immediate rehabilitation course. This can also be continued and concluded at home with further savings in postoperative costs. In professionally active patients, there is an early resumption of full working capacity with further direct patient and indirect social gain.
Day surgery represents an effective, efficacy and cost- effective management instrument and a way to give quality to the offer in the surgical field, according to the new philosophy that inspires modern medical care namely that of operating better and safely, in the interest of the patient, at lower cost and with short hospitalization [10].
The prospective payment system based on DRG dates to the 1970s from Yale University in the U.S. and was transposed in Italy approximately in the mid-1990s by contributing to implement the 1992/93 health care reform. The reform was intended to implement health care efficiency and to develop resource monitoring programs for a better management of the quality of care and an improved operational performance of hospitals. The DRG system was thus created to ensure better cost-benefit of health care.
Technologies that provide a minimally invasive approach such as UKA with reduced blood loss, greater guarantees of tissue tightness, low recovery times and cost-effective prosthetic costs assume a fundamental role that, however, the current DRG system has not yet acquired. The progressive innovation of surgical techniques with the introduction of robotic prosthetics, for example in orthopedics, makes it necessary to adjust the DRG system, which, as currently conceived, is out of date due to the deficient remuneration that is linked to a greater use of technology (e.g., rental or purchase of the robotic system, consulting and/or engineering assistance, etc.) [11]. In addition, it would also be desirable to evaluate the clinical results obtained regarding the survival of the implants and thus the well- being of patients, as advocated by the Italian Arthroplasty Registry project.
As we have been increasingly witnessing new technologies in health care resulting in changing concepts and attitudes, we asked ourselves some questions.
- It’s possible to obtain feasibility, safety, clinical benefits, health care cost containment, and patient satisfaction in day surgery?
- Can we spend less while offering the same quality of care?
- Is there a possibility of discharging the patient on the same day of surgery even though in the past hospitalization was prolonged for several days?
- Can the patient happily accept discharge on the same day of surgery?
In scientific literature we find many studies on the advantages of day surgery in general. Some of these are related to the patient namely shorter waiting time with reduced waiting lists, less distance from the family environment and minimal disruption of living habits, decreased risk of infection due to less hospital stay, decreased stress of hospitalization, reduced period of disability. Other benefits are related to predetermination of costs, decrease in shifts and less demand on nursing and medical staff, higher productivity, more quality and consideration of the patient himself, faster patient turn over, and lowering of inpatient costs. By freeing hospitals of a percentage of ordinary inpatients, they would be able to devote more human resources to more important diseases that require longer hospitalizations. On the other hand, as for the disadvantages, there may be the difficult acceptance of the patient who feels more protected with hospitalization even at night or increasingly rare but possible complications such as nausea and vomiting or inadequate pain control, such that rest at home is insufficient and with a greater burden on the family [12, 13, 14].
In Richter and Diduch’s 2017 study, outpatient UKA is shown to be feasible and cost-effective by reducing inpatient bed occupancy with the prerogative of investing the saved resources in other more necessary areas. As in our study, no differences are reported between the groups of inpatients and day-surgery inpatients in terms of complications or readmissions to the hospital [15].
The semiactive Robotic Arm interactive orthopaedic System (RIO® MAKO Stryker surgical corporation) was used for the robotic surgical procedure of the single-compartment knee replacement in our study. The introduction of robotic systems is intended to compensate for the imperfections of traditional surgery that can lead to complications by increasing the revision rate [16].
The single-compartment prosthesis, in the appropriate indication, is becoming increasingly popular because of the advantages over total prosthesis namely reduced surgical risk, shorter hospitalization, better kinematics, faster recovery and thus lower costs [17]. In addition, the increasing demand for minimally invasive approaches has led to the development of robot-assisted techniques by improving gesture and surgical precision, as well as component alignment [18]. Lately, the Australian registry Smith PN, et al. [19] is reporting better survival of robot-assisted implanted unicompartmental prosthesis than those with traditional technique.
In the 1990s’ the 10-year failure rate was 35% [20].
Today in the robotic field, on the other hand, the accuracy, precision of the surgical gesture, minimal possibility of error and safety of the system offer greater potential for robotic UKA [21]. In the study by Bell, Anthony et alt. it is emphasized that the use of the MAKO RIO® robot leads to greater accuracy of UKA implant placement than that performed by traditional manual method. Implant accuracy was verified and confirmed after 3 months by postoperative computed tomography to assess the accuracy of component placement in axial, coronal, and sagittal planes [22]. This concept is reinforced by Jiyan Lin’s study in which they emphasize the best results in implant accuracy, soft tissue balance, patient satisfaction and quality of life scales, complication rates, and learning curve in short-term outcomes [16].
In the work of Bradley, Middleton et alt. it is underlined that patients who were discharged on the same day of surgery without complications also had a high level of satisfaction, and for the health care system there was a better management of resources and cost savings [23]. Other works emphasize that since UKA with traditional technique is associated with a higher revision rate, the initial cost benefit gained from shorter hospital stay and faster rehabilitation is automatically cancelled later [24].
Regarding the type of complications after UKA there are sometimes redness, tenderness, swelling or pain that is not getting better or is getting worse, stiffness, deep vein thrombosis, and rarely, wound infection , pulmonary embolism, progression of arthritis in the controlateral compartment, medial collateral ligament injury, impingement, infection, arthrofibrosis, and failure due to unexplained pain. The most common complication after UKA is dislocation of the mobile bearing. Operative time was found to independently predict increased risk of non-home discharge, increased surgical site infection, blood transfusion, myocardial infarction, extended length of stay, and rarely mortality [25, 26, 27].
Further studies are needed to examine the complications and revision rate of UKA procedures implanted with a robotic system and compare the results with all other non-robot- assisted UKA procedures.
Materials and Methods
In the study, regional data of hospital discharge form and Mako® Robot System archival data of medial-only UKA operated patients in hospitals in the Asl Toscana Sudest of the Arezzo District were collected. In the inclusion criteria there were all patients operated on electively for osteoarthritis or osteonecrosis of the medial condyle of femur from July 1, 2014 to December 31, 2018. The dates were determined by when surgery using the Mako robotic technique was started in the Arezzo District of the Vast Area Toscana Sudest in June 2014.
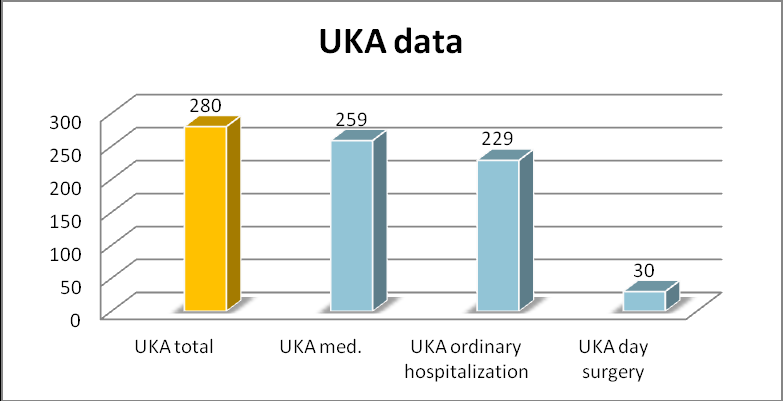
A total of 280 robot-assisted UKA surgeries were performed during the study period, 259 of which were medial surgeries. The surgical team was always the same with oversight by two experienced senior surgeons, who were both Directors of a Complex Structures.
In this study we considered 259 cases of only medial UKA surgeries. 30 patients of these 259 were operated on in day surgery by waiting list progression without any exclusion; the other 229 were operated on in ordinary regime.
We assessed the differences between the two groups in transfusion, minor or major complications with hospitalization within 7 days from discharge and within 90 days after surgery to determine the feasibility and safety of partial knee replacement in day surgery. We assessed pain with Verbal Rating Scale in the two groups before surgery, at discharge, after 3 and 12 months. The Verbal Rating Scale associates the level of pain present (no pain, mild, moderate, severe, unbearable) with a number from 0 to 4.
Both groups were homogeneous in parameters such as age, sex, comorbidities, ASA, corporate antibiotic protocol [28, 29], corporate pain protocol [30], corporate blood management [31], and corporate rehabilitation protocol [32]. All data were collected by an independent practitioner who was not involved in the study.
The collected biographical and clinical data of the operated patients were: age at the time of surgery, male- female gender, laterality. We then had data on days of ordinary hospitalization, transfusions performed between the two groups of patients in the postoperative period, postoperative complications, and readmissions to the emergency department and/or hospitalization in the 7 days after surgery, and data inherent in hospital readmissions for minor or major complications in the two groups in the 90 days after surgery.
We collected the ASA value data of the 30 patients under study namely 9 patients with ASA 1, 19 patients with ASA 2, and 2 patients with ASA 3.
Furthermore, we assessed patient satisfaction with the surgical course and outcomes of the 30 patients operated for UKA in day surgery, 3 and 12 months after surgery with Likert scale quantifying satisfaction from 1 to 5: 1 totally dissatisfied, 2 dissatisfied, 3 neutral, 4 satisfied, 5 completely satisfied.
The average time for robotic surgery between the first 30 patients operated in 2014 and the last 30 operated in 2018 was then studied to assess the learning curve of the technique over this period.
In addition to this, it was evaluated after how many cases the best performance was achieved in terms of confidence level and minimum learning curve time.
The results of all collected data were compared with descriptive analysis to determine any baseline differences between the two groups with ordinary hospitalization and day surgery.
Descriptive statistics were used for data of participants. One sample and independent sample T tests were used to assess eventual differences within and between groups for the continuous variables that are presented with their mean and standard deviation (SD). The significance threshold was set up at P < 0.05.
Results
The study shows that from June 2014 to December 2018, 280 UKAs, of which 259 medial (92.5 %) and 21 lateral UKAs (7.5 %) were performed in the Arezzo area of the Asl Toscana Sudest by two senior surgeons as the first operator and by the same surgical team.
As shown in the bar chart below, 30 patients representing 11.58% underwent medial UKAs (group A), which were performed in day surgery by waiting list progression without any exclusion and 229 patients representing 88.41% underwent medial UKAs (group B) and were operated on as inpatients (Figure 1).
The average age of patients is 69.9; in group A it is 71.7, in group B it is 68.1.
Regarding gender, there were 17 females (56.66%) and 13 males (43.33%) in group A, while 108 females (47.16%) and 121 males (52.83%) in group B.
In total 125 females (48.26%) and 134 males (51.73%) of medial UKA.
For laterality, there were 15 right side (50%) and 15 left side (50%) in group A, and 126 right side (55.02%) and 103 left side (44.97%) in group B.
Regarding hospitalization data, group A stayed 12 hours in day surgery, while the average number of days of ordinary hospitalization in group B was 6.2 days.
Ordinary hospitalization, which technically would be two nights, in group B sample also included days for functional re-education and rehabilitation with a discharge that aimed for complete autonomy with Barthel scale between 95 and 100 (Barthel scale from 0 min to 100 max functionality) and Activities of Daily Living (ADL) with a value between 5 and 6 (it ranges from 0 min to 6 max functionality). Patients in day surgery were discharged in the evening with walking autonomy with aids at least for a short distance; for this study sample, functional re-education and rehabilitation was arranged in another modality. Patients were assisted by telephone by the hospital rehabilitation service in the daytime hours following discharge and then taken over by territorial physiotherapy clinics.
The mean hemoglobin value in group A before surgery was 13.84 while at discharge it was 12.18. In group B, the mean hemoglobin value before surgery was 14.0 while at discharge it was 11.8. This difference in hemoglobin at discharge between the two groups is surely due to the longer ordinary hospitalization with quantification of hidden leaks occurring on postoperative days.
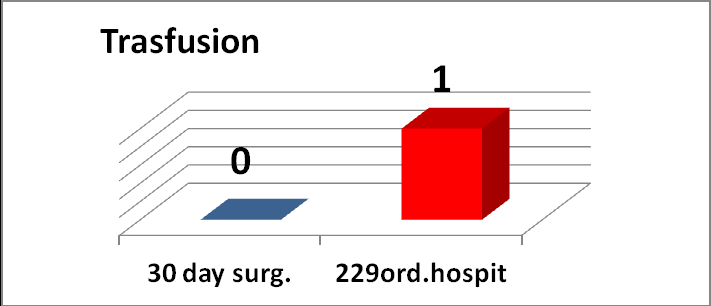
There was only one transfusion performed during hospitalization in the ordinary hospitalization group (Figure 2).
The only transfused patient belonged to the ordinary hospitalization group B. She was a 67-year-old woman with medial femoral condyle necrosis with positive oncological history for lymphoma who was transfused on the third day with a hemoglobin of 8.5 having a starting hemoglobin of 10.5.
- As shown in Table 1, no minor or major complications occurred within 7 and 90 days after surgery or hospital readmissions in the two groups examined.
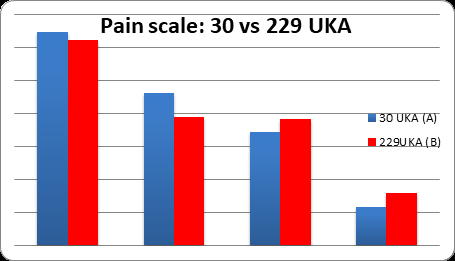
- With regard to pain, the Verbal Rating Scale was administered before surgery (group A: 3.23(SD 2,84), group
- B: 3.11(SD 2,04) for P=0.7735), at discharge (group A: 2.31, group B: 1.95 for P=0.3882), 3 months (group A: 1.72, group
- B: 1.91 for P=0.6487) and 12 months (group A: 0.58, group B:
- Pain Scale ( from 0 to 4)
- 30 UKA (A)
- 229UKA (B)
- P<0,05
- Pre Surgery
- 3,23(SD 2,84)
- 3,11(SD 2,04)
- P=0,7735
- Discharge
- 2,31
- 1,95
- P=0,3882
- After 3 Months
- 1,72
- 1,91
- P=0,6487
- After 1 Year
- 0,58
- 0,8
- P=0,5978
Table 1: Pain Scale Average - Group A vs Group B.
| Group A (30 pt) | Group B (229 pt) | Total (259) Group A+B | |
|---|---|---|---|
| Age at Surgery | 71,7 | 68,1 | 69,9 |
| Num.Male | 13(43,33%) | 121(52,83 %) | 134(51,73%) |
| Num.Female | 17(56,66% | 108(47,16 %) | 125(48,26 %) |
| Laterality | 15 R - 15 L | 126 R- 103 L | 141 R – 118L |
| Days In Hospital | 12hours | 6,2 days | |
| Hb Before Surgery | 13,84 | 14,0 | |
| Hb After Surgery | 12,18. | 11,8 | |
| Trasfusion | 0 | 1 | 1 |
| Complications After 7 Days | 0 | 0 | 0 |
| Complications After 90 Days | 0 | 0 | 0 |
- As shown in Table 1, no minor or major complications occurred within 7 and 90 days after surgery or hospital readmissions in the two groups examined.
- With regard to pain, the Verbal Rating Scale was administered before surgery (group A: 3.23(SD 2,84), group
- B: 3.11(SD 2,04) for P=0.7735), at discharge (group A: 2.31, group B: 1.95 for P=0.3882), 3 months (group A: 1.72, group
- B: 1.91 for P=0.6487) and 12 months (group A: 0.58, group B:
- Pain Scale ( from 0 to 4)
- 30 UKA (A)
- 229UKA (B)
- P<0,05
- Pre Surgery
- 3,23(SD 2,84)
- 3,11(SD 2,04)
- P=0,7735
- Discharge
- 2,31
- 1,95
- P=0,3882
- After 3 Months
- 1,72
- 1,91
- P=0,6487
- After 1 Year
- 0,58
- 0,8
- P=0,5978
Table 1: Pain Scale Average - Group A vs Group B.
0.80 for P=0.5978) after surgery. In the T Student test, there was no statistical difference between the two groups, so they were also considered homogeneous in terms of pain (Tables 2 and Figure 3).
At 2-year follow-up, complications in the 280 cases in the total UKA series were: -1 infection (0.3%) with subsequent 2-stage revision with total prosthesis and healing. -2 UKA with persistent pain (0.7%) (1 medial, 1 lateral) and revision with total prosthesis and healing. -No DVT.
Overall, 3 failures out of 280 with a two-year revision rate of 1%. Of considerable interest is the study of the learning curve regarding operative time.
The curve indicates the achieved level of surgical goals and organization of the surgical team with the robot, after having obtained the Mako robotics certifications and the right training. This obviously also depends on factors related not only to the skill of the surgeon but also to multiple organizational factors.
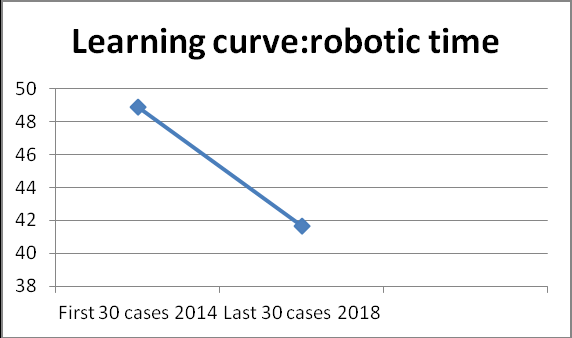
The surgical time meant as robotic time was evaluated to examine the learning curve between the first 30 cases in 2014 and the last 30 cases in 2018. The result was that the learning curve decreased as the years went by and thus as the surgeon and surgical team became more experienced to settle at an average value [33].
The difference in the averages between the first 30 cases and the last 30 cases was statistically significant for P<0.01. In 2014 the mean was 48.9 minutes (SD 10.38) while in 2018 the mean dropped to 41.66 minutes (SD 10.28) (Table 3, Figure 4 & 5).
| FIRST 30 Ukas IN 2014 | LAST 30 Ukas IN 2018 | |
|---|---|---|
| Average | 4,89,000 | 4,16,667 |
| Stand.Dev. | 1,03,835 | 1,02,833 |
| P = 0,0088 |
Table 3: Dataset of UKAs in 2014 vs UKAs in 2018.
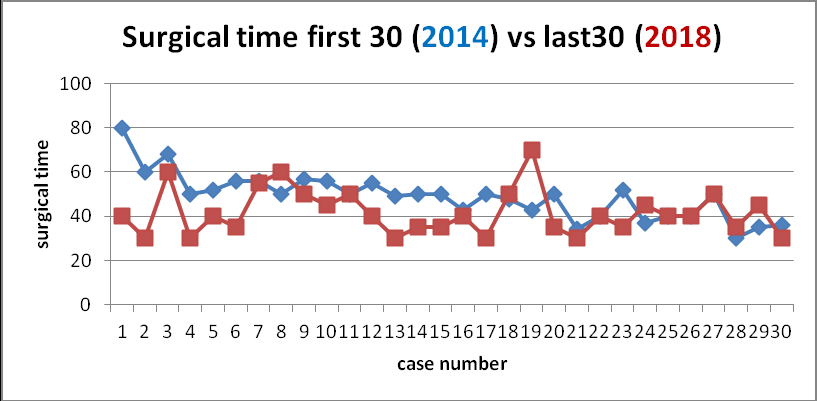
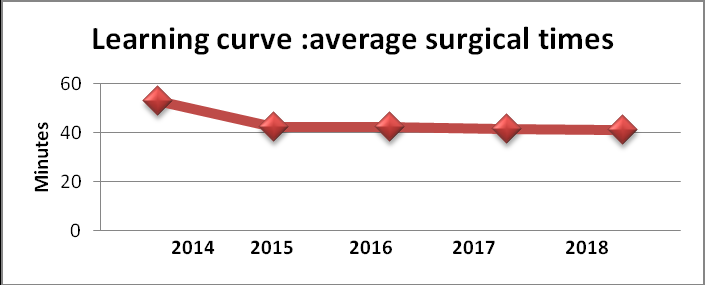
The average operating time in minutes, intended as global skin-to-skin time, of UKA Mako surgeries from 2014 to 2018 year by year was also evaluated to see how the line on the curve indicating the learning rate of robotic time directly related to the surgeon and of the global skin-to-skin time related to the entire operating team, decreases. The average surgical time decreased from 52.71 mins in 2014, to 42.21 mins in 2015, 42.31 mins in 2016, 41.28 mins in 2017, and 40.90 mins in 2018 (Figure 6).
We found few studies in the scientific literature that address this topic, not about surgical accuracy but surgical time. Studies report that surgical time is reduced after performing 5 to 10 procedures, with constant time reached after 8 cases [34]. Other studies Kayani B, et al. [35, 36] show a learning curve after 6 cases to achieve optimal and consistent surgical time with a confidence level of the surgical team for robotic UKA but not for implant accuracy.
In our study, we found that the level of confidence and stabilization of surgical time was 9 cases (p<0.05), which was necessary for the achievement of an optimal learning curve with statistical significance. Thus, in our experience robotic UKA had a learning curve of 9 surgical cases for achieving consistent and optimal minimal operative time.
Regarding satisfaction with the surgery and results, a Likert scale of 1 to 5 (1 totally dissatisfied, 2 dissatisfied, 3 neutral, 4 satisfied, 5 completely satisfied) was administered 3 and 12 months after surgery to patients operated on in day surgery as part of orthopedic specialist follow-up. Of the 30 patients, 29 responded to the required questionnaire. This showed that while 3 months after surgery about 80% of patients were both completely satisfied and satisfied (Likert scale value 4 and 5), after 1 year the average stood at 76%. At one-year follow-up, only 3.44% of operated patients remained strongly dissatisfied (Likert scale value 1) (Table 4). The precise reason for this change after 1 year is not apparent from the questionnaire administered [37, 38].
| After 3 Months | n.Pt. | % | After 12 Months | n.Pt. | % |
|---|---|---|---|---|---|
| 1strongly dissatisfied | 0 | 1 strongly dissatisfied | 1 | 3,44% | |
| 2 dissatisfied | 0 | 2 dissatisfied | 3 | 10,34% | |
| 3 neither dissatisfied nor satisfied | 6 | 20,68% | 3 neither dissatisfied nor satisfied | 3 | 10,34% |
| 4 satisfied | 5 | 17,24% | 4 satisfied | 6 | 20,68% |
| 5 strongly satisfied | 18 | 62,06% | 5 strongly satisfied | 16 | 55,17% |
Table 4: Likert scale from 1 to 5.
Discussion
Unicompartmental prosthesis is a viable solution for healing grade IV arthrosis of only one compartment of the knee or painful necrosis of the femoral condyle. It is a procedure on only one anatomical compartment that permits sparing of the healthy compartments with sparing of the cruciate ligaments by promoting the natural kinematics of the knee. Although there is controversial evidence on the mid- and long-term survival success of partial versus total prosthesis, partial prosthesis is definitely a technique that has a better chance of success if performed by experienced surgeons [39] and because of this, conclusions in the scientific literature often differ depending on personal surgical experience.
The review cited earlier that shows us 10 conundrums of medial UKA leads to the conclusion that many factors have led to the revival of UKA in the past 10 years. Among these, there are superior functional outcomes, cost-effectiveness, and improved implant survival. Therefore, UKA should be considered as an integral part of surgical options for the treatment of knee osteoarthritis by orthopedic surgeons. UKA surgery should be performed optimally by carefully selecting patients to increase their survival and reach their true potential [24]. The possibility of performing UKA by robotic technique has certainly improved the radiological and clinical outcomes reported in the scientific literature: accuracy of implantation, speed of recovery, less pain, and shorter hospitalizations. Lately, prosthetic registries are also showing higher survival of mono-robotic prostheses than those performed with manual technique. (AOANJ Report 2023, Figure KP15)[19].
In our study, there were no differences in the two groups between the 30 patients operated in day surgery and the 229 operated in ordinary regime in terms of transfusion, complications or readmissions to emergency department and/or hospital within 7 days, nor minor or major complications within 90 days after surgery, nor in terms of pain, besides patient satisfaction. Therefore, it is clear that day surgery can be performed for its safety, cost-saving and feasibility, as well as for clinical benefit and absolute saving of hospital days with reduction of both direct and indirect costs. Thus, there are no significant differences that would justify UKA surgery in ordinary regime, and consequently, there is ample evidence that UKA surgery can be performed in day surgery.
We answer in the affirmative to all our initial questions namely: you can spend less while offering the same quality of care, you can discharge the patient on the same day of surgery, and the patient can accept with satisfaction discharge on the same day of surgery. We know that for the National Health System optimizing bed occupancy is crucial; therefore, being able to reduce inpatient days would lead to a reduction in indirect costs per surgery with a likely increase in their number. In orthopedics the inpatient stay costs about €808.56, the average stay is 6 days compared to the few hours in day surgery (€808.56 x 5nights =4042.8); therefore we have a significant indirect cost savings per surgery.
Even if we consider only the economic difference of two days per inpatient days between day surgery and ordinary hospitalization without a rehabilitation program, there is still a savings of €1,617.12 (808.56 x 2). This is even more so as functional rehabilitation of a mono-robotic is definitely low impact both organizationally and economically with outpatient or home setting. Reduced costs are associated with increased surgical productivity [40], both in terms of reduced bed occupancy [41], improved bed turnover and, consequently, reduced waiting list. (Figure 7-8 by Dt. Caldora P, et al. [40])
Conclusions
UKA surgery represents the best surgical solution for end-stage unicompartmental knee arthrosis. The application of robotic technology, in the face of higher costs, particularly in this surgery, has significantly improved the radiographic, clinical, and survival outcomes of mono-robotic prostheses compared with the manual technique. These data confirm and justify the use of robot in mono for a faster functional recovery with a short to medium-term reduction in the revision rate of these prostheses. These last two parameters justify even more the use of robot in young and active, income-producing patients undergoing a single-compartment prosthesis. The possibility of performing this robotic surgery in day surgery seals the advantages of the technique by further reducing the surgery costs related to hospitalization days and by reducing the stress of hospitalization for patients with faster return to daily activities, as well as work. The elimination of the cost of ordinary hospitalization alone (808.56 Euros for 2) with higher bed turnover leads to substantial economic savings whose savings figure per surgery offsets the higher robotic cost per surgery. To this should be added the lower social costs of faster recovery of working capacity for active patients and the indirect costs of reducing the number of necessary revisions over time.
In our study, we found no differences between group A of patients operated in day surgery and group B of patients operated in ordinary inpatient care about the number of transfusions, complications or hospital readmissions within 7 days, nor minor or major complications within 90 days after surgery. We found no statistically significant differences in the VRS pain scale between the two groups while we found a high satisfaction index of patients undergoing day surgery. After 3 months, 80% and after 12 months, 76% of patients in the day-surgery operated group expressed themselves with value 4 and 5 on the Likert scale of satisfaction.
Our study shows that robotic medial UKA can be safely performed in day surgery. Being able to perform this surgery under the assumptions and characteristics of day surgery organization means reduction of surgery costs, waiting lists, hospitalization risks, and of patient stress. The resulting organizational proposal is to authorize Italian health facilities to perform partial prosthesis surgery in day surgery with equal DRG reimbursement. Maintaining the same prosthetic DRG with the opportunity of day surgery would act as an organizational stimulus for hospitals with the purpose of economic savings related to hospitalization with automatic improvement of bed occupancy rates, reduction of waiting lists, greater patient satisfaction and involvement in the care process, and the possibility of investment in new technologies of which orthopedic robots are a part.
Our study has some limitations. The day surgery sample had a small number so further studies with large numbers are needed.
This study makes some point that need to be evaluated more carefully. One question is why after 1 year follow up in the day surgery sample about 14% remained strongly dissatisfied or dissatisfied. No reason from the questionnaire administered. PROMs don’t always give exhaustive answer.
The second thing is to have available more detailed analysis of patient demographics and more information on the cost analysis and potential economic impact of implementing day-surgery UKA in the Italian healthcare system but it was not possible in this study.
Further researches are needed in order to report functional outcomes, data on survival of the prosthesis, complications, cost-effectiveness but also studies with regard to long-term PROMs i.e. beyond 10 years. One thing is clear: robotic-assisted surgery is now being increasingly used in medical practice.
References
-
(2002) Guidelines for day surgery activities. State- Regions Conference of 1 August 2002.
-
Confalonieri N, Musso M, Ongaro D (2002) Management model of autonomous orthopedic day surgery operating unit Orthopedic Day surgery free unit–Management model. GIOT 28: 233-44.
-
Campagna S, Antonielli D’Oulx MD, Paradiso R, Perretta L, Viglietti SR, et al. (2016) Postoperative Pain, an Unmet Problem in Day or Overnight Italian Surgery Patients: A Prospective Study-Pain Res Manag 2016: 6104383.
-
Fischer HB, Simanski CJ, Sharp C, Bonnet F, Camu F, et al. (2008) A procedure-specific systematic review and consensus recommendations for postoperative analgesia following total knee arthroplasty. Anaesthesia 63(10): 1105-1123.
-
DR Kerr, Kohan L (2008) Local infiltration analgesia: a technique for the control of acute postoperative pain following knee and hip surgery: a case study of 325 patients. Acta Orthopaedica 79(2): 174-183.
-
Toftdahl K, Nikolajsen L, Haraldsted V, Madsen F, Tønnesen EK, et al. (2007) Comparison of peri- and intraarticular analgesia with femoral nerve block after total knee arthroplasty A randomized clinical trial. Acta Orthopaedica 78(2): 172-179.
-
Andersen LØ, Kehlet H (2014) Analgesic efficacy of local infiltration analgesia in hip and knee arthroplasty: a systematic review. British Journal of Anaesthesia 113 (3): 360-374.
-
Zhang J, Nathan Ng, Scott CEH, Blyth MJG, Haddad FS, et al. (2022) Robotic arm-assisted versus manual unicompartmental knee arthroplasty: a systematic review and meta-analysis of the MAKO robotic system. Bone Joint J 104-B(5): 541-548.
-
Foissey C, Batailler C, Vahabi A, Fontalis A, Servien E, et al. (2023) Better accuracy and implant survival in medial imageless robotic-assisted unicompartmental knee arthroplasty compared to conventional unicompartmental knee arthroplasty: two- to eleven- year follow-up of three hundred fifty-six consecutive knees. Int Orthop 47(2): 533-541.
-
Sturniolo G, Bonanno L, Lo Schiavo MG, Tonante A, Taranto F, et al. (2007) Day-surgery as a factor in reducing hospital stay. Chir Ital 59(1): 41-52.
-
Dallapiccola B (2019-2021) Reflections and perspectives on the use of DRGs: a new model of application and development. Ministry of Health Working Group, Superior Council of Health.
-
(2023) Annual report on the hospitalization activity hospital. Italian Society of Outpatient Surgery and Day Surgery.
-
(2003) Best Evidence based practice information sheets for health professionals. Practice supplement 8(1).
-
Richter DL, Diduch DR (2017) Cost Comparison of Outpatient versus Inpatient Unicompartmental Knee Arthroplasty. Orthop J Sports Med 5(3): 2325967117694352.
-
Lin J, Yan S, Ye Z, Zhao X (2020) A systematic review of MAKO-assisted unicompartmental knee arthroplasty. Int J Med Robot 16(5): 1-7.
-
Lonner JH, Klement MR (2019) Robotic-assisted Medial Unicompartmental Knee Arthroplasty: Options and Outcomes. J Am Acad Orthop Surg 27(5): e207-e214.
-
Luo TD, Hubbard JB (2020) Arthroplasty Knee Unicompartmental. Treasure Island (FL): StatPearls Publishing.
-
Smith PN, Gill DR, McAuliffe MJ, James D, Christopher J, et al. (2023) Hip, Knee and Shoulder Artrhroplasty : 2023 Annual Report. Australian Orthopedic Association.
-
Marmor L (1988) Unicompartmental arthroplasty of the knee with a minimum ten-year follow-up period. Clin Orthop Relat Res (228): 171-177.
-
Batailler C, White N, Ranaldi FM, Neyret P, Servien E, et al. (2019) Improved implant position and lower revision rate with robotic-assisted unicompartmental knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 27(4): 1232-1240
-
Bell SW, Anthony I, Jones B, MacLean A, Rowe P, et al. (2016) Improved Accuracy of Component Positioning with Robotic-Assisted Unicompartmental Knee Arthroplasty: Data from a Prospective, Randomized Controlled Study. J Bone Joint Surg Am 98(8): 627-635.
-
Bradley B, Middleton S, Davis N, Williams M, Stocker M, et al. (2017) Discharge on the day of surgery following unicompartmental knee arthroplasty within the United Kingdom NHS. Bone Joint J 99-B(6): 788-792.
-
Mittal A, Meshram P, Kim WH, Kim TK (2020) Unicompartmental knee arthroplasty, an enigma, and the ten enigmas of medial UKA. J Orthop Traumatol 21: 15.
-
Mergenthaler G, Batailler C, Lording T, Servien E, Lustig S (2021) Is robotic-assisted unicompartmental knee arthroplasty a safe procedure? A case control study. Knee Surg Sports Traumatol Arthrosc 29(3): 931-938.
-
Held MB, Boddapati V, Sarpong NO, Cooper HJ, Shah RP, et al. (2021) Operative Duration and Short-Term Postoperative Complications after Unicompartmental Knee Arthroplasty. J Arthroplasty 36(3): 905-909.
-
Cregar WM, Goodloe JB, Lu Y, Gerlinger TL (2021) Increased Operative Time Impacts Rates of Short- Term Complications after Unicompartmental Knee Arthroplasty. J Arthroplasty 36(2): 488-494.
-
(2013) Tuscany Region: Clinical risk management center - Address of the regional therapeutic commission for greater appropriateness of use of antibacterial chemotherapeutics.
-
(2017) National Plan to Combat Antimicrobial Resistance (PNCAR) 2017-2020. Ministry of Health.
-
(2009) Tuscany Region: Regional project for the fight against pain: approval of training courses: Resolution n°1029 of 27/12/2007. Management of analgesia in trauma. CSR opinion.
-
Guidelines for the PBM program of the Ministry of Health of 2/11/2015 (LG CNS 05, Rev.0 of 27/10/2016), National Blood Center.
-
Protocol for rehabilitation interventionRev.n°3 of 11/28/2017; IDT-Rehabilitation paths - update 2013; P.T. rehabilitation protocol after PTG and PTA surgery Rev.n°4 of 11/21/2017.
-
Redmond JM, Gupta A, Hammarstedt JE, Petrakos AE, Finch NA, et al. (2015) The learning Curve associated with robotic-assisted total hip arthroplasty. J Arthroplasty 30(1): 50-54.
-
Clement ND, Al-Zibari M, Afzal I, Deehan DJ , Kader D (2020) A systematic review of imageless hand-held robotic-assisted knee arthroplasty: learning curve, accuracy, functional outcome and survivorship. EFORT Open Rev 5(5): 319-326.
-
Kayani B, Konan S, Pietrzak JRT, Huq SS, Tahmassebi J, et al. (2018) The learning curve associated with robotic- arm assisted unicompartmental knee arthroplasty: a prospective cohort study. Bone Joint J 100-B(8): 1033- 1042.
-
Begum FA, Kayani B, Morgan SDJ, Ahmed SS, Singh S, et al. (2020) Robotic technology: current concepts, operative techniques and emerging uses in unicompartmental knee arthroplasty. EFORT Open Rev 5(5): 312-318.
-
Dretakis K, Igoumenou VG (2019) Outcomes of robotic-arm-assisted medial unicompartmental knee arthroplasty: minimum 3-year follow-up. Eur J Orthop Surg Traumatol 29(6): 1305-1311.
-
Pearle AD, van der List JP, Lee L, Coon TM, Borus TA (2017) Survivorship and patient satisfaction of robotic- assisted medial unicompartmental knee arthroplasty at a minimum two-year follow-up. Knee 24(2): 419-428.
-
Johal S, Nakano N, Baxter M, Hujazi I, Pandit H, et al. (2018) Unicompartmental Knee Arthroplasty: The Past, Current Controversies, and Future Perspectives. J Knee Surg 31(10): 992-998.
-
Caldora P, D’Urso A, Banchetti R, Arniani S, Colcelli D, et al. (2020) Blood trasfusion, hospital stay and learning curve in robotic assisted total hip arthroplasty. Journal of biological regulators & homeostatic agents 34(4): 37-49.
-
Banchetti R, Dari S, Ricciarini ME, Lup D, Carpinteri F, et al. (2018) Comparison of conventional versus robotic- assisted total hip arthroplasty using the Mako System: An Italian retrospective study. Journal of Health and Social Sciences 3(1): 37-48.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda