First-Line Sodium Glucose Co-transporter 2 Inhibitors: Physicochemical Properties and Measurement in Biological Fluids
Sodium glucose co-transporter 2 (SGLT 2) inhibitors represent a new class of glucose-lowering drugs that act through the inhibition of glucose reabsorption at the proximal tubular cells of the kidney. The objective of the study was to provide most current information on the physicochemical properties and analytical methods of determination in biological matrices of the first-line sodium glucose co-transporter 2 (SGLT 2) inhibitors. The methodology of literature search entailed obtaining information from published works in scientific journals, official books and the internet websites. The results of the study show that these first-line therapeutic agents selectively inhibit the reabsorption of glucose in the kidney by almost 30-50 percent. Apart from their effects on carbohydrate homeostasis, they also affect human metabolism by decreasing blood pressure, arterial stiffness, body weight, serum concentrations of insulin. They increase glucagon concentration thus shifting energy metabolism towards the utilization of fatty acids and ketone bodies. They have also been found to preserve renal function in patients with type 2 diabetes mellitus and established cardiovascular disease. In conclusion, these therapeutic agents exhibit significant cardio-protective and renoprotective effects by their mechanism of action.
Introduction
Glucose reabsorption in the proximal tubule of the renal system occurs through two distinct sodium-dependent glucose transport systems, one with higher affinity and lower capacity for glucose (sodium glucose co-transporter 1, SGLT 1) and the other with relatively low affinity and high capacity (sodium glucose co-transporter 2, SGLT 2) [1, 2, 3]. Sodium glucose co-transporter 1 is found at high levels in the intestine and is also located in the kidney, heart, and skeletal muscle whereas sodium glucose co-transporter 2 is found almost exclusively in the kidney [1]. Renal sodium glucose co- transporter 2 is observed to increase in humans with type-2 diabetes mellitus [4]. Type 2 diabetes mellitus is a chronic disease of the endocrine system caused by progressive β cell dysfunction in the presence of chronic insulin resistance, leading to increase glucagon secretion, renal glucose reabsorption, gluconeogenesis, decrease in incretin response and a progressive decrease in plasma glucose homeostasis [5]. It leads to excessive morbidity and premature mortality. Insulin resistance, insulin insufficiency (due to secretory defects) and increased renal glucose reabsorption play major roles in the pathogenesis of hyperglycemia in patients with type 2 diabetes mellitus. The renal glucose reabsorption at the proximal tubule is antagonized by sodium glucose co- transporter 2 inhibitors. The sodium glucose co-transporter 2 inhibitors are a new class of anti-diabetes drugs that inhibit renal glucose reabsorption at the proximal tubular cells of the kidney leading to reductions in plasma glucose concentrations as well as increase in renal excretion of glucose in patients with type-2 diabetes mellitus [6, 7]. These inhibitors are related to phlorizin in their basic chemical structures. Phlorizin is a potent SGLT 2 inhibitor but not clinically used because of poor oral absorption, and the formation of phloretin by metabolism.
Canagliflozin, dapagliflozin, empagliflozin are the first- line sodium glucose co-transporter 2 inhibitors. However, ipragliflozin, luseogliflozin, topogliflozin are other sodium glucose co-transporter 2 inhibitors that have been approved for the treatment of type 2 diabetes mellitus [8]. Ertugliflozin, janagliflozin and sotagliflozin are still undergoing clinical trials. These first-line SGLT 2 inhibitors may have some (i) weight lowering effect (as a result of increased fatty acid oxidation, loss of calories due to glucosuria, natriuresis and osmotic diuresis-induced volume depletion), (ii) reduction in blood pressure (resulting from decrease in sympathetic nervous system activity, local inhibition of the renal renin- angiotensin system, decrease of glucose levels and insulin resistance, decrease in serum uric acid levels, decrease in body weight etc, (iii) small increase in serum electrolytes (such as potassium, magnesium, phosphate) and (iv) cardioprotective properties. Adverse effects reported for these inhibitors include polyuria and potential for volume depletion, hypotension (due to intravascular volume depletion), genitourinary infections, and increase in the incidence of bladder cancer [9]. They are contraindicated in patients with severe renal impairment or ketoacidosis.
The monitoring of these first-line SGLT 2 inhibitors utilized in the treatment of type 2 diabetes mellitus in biological fluids is important in order to understand their pharmacokinetics, pharmacodynamics, and metabolism. The biological fluids of interest are usually whole blood, serum or plasma; urine; saliva [10, 11]. However, other fluids such as cerebrospinal fluid (CSF); amniotic fluid; ocular fluid; pleural fluid (from the sac surrounding the lungs); pericardial fluid (from the sac surrounding the heart); peritoneal fluid (also called ascitic fluid; from the abdomen) and synovial fluid (fluid that is found in joint cavities) could be analyzed for parent drug(s) concentration levels.
As the physicochemical properties of drug molecules influence the rate at which the drug dissolves and crosses the gastrointestinal cell membranes and hence its plasma concentration, we considered it necessary to incorporate the information in this study. Plasma drug concentration determination at any period provides indirectly the rate and extent the active drug is absorbed from the gastrointestinal tract and becomes available at the site of action [12]. The pharmacokinetic profiles of first-line SGLT 2 inhibitors have shown that they have low plasma concentration levels. Therefore, therapeutic monitoring of these inhibitors becomes inevitable in order to adjust the drug dose to individual need and to minimize the risk of dose-related toxicity. In addition, due to the chronic and debilitating nature of the metabolic disorder, SGLT 2 inhibitors are often given in combination with other antidiabetic agents. Thus, it requires accurate, precise, sensitive, selective and specific analytical methods to accurately quantify these SGLT 2 inhibitors in biological fluids.
Literature search has revealed that spectroscopic and chromatographic methods are the analytical methods often used to determine these first-line SGLT 2 inhibitors in biological fluids. However, chromatographic methods are mostly used due to their sensitivity, selectivity and specificity. These chromatographic methods are utilized either as hyphenated or non-hyphenated system. Hyphenation is a speciation of a separation technique and one or more spectroscopic detection techniques. In the present paper, we attempt to provide information on the chemical structures, physicochemical properties as well as the analytical methods needed to quantify these first line SGLT 2 inhibitors in biological fluids. The provided information will help to minimize the time spent by research scientists searching for such relevant information on these drugs in the literature.
The information include
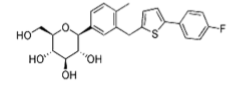
Canagliflozin
Chemically defined as (2S,3R,4R,5S,6R)-2-[3-[[5-(4- fluorophenyl)thiophen-2-yl]methyl]-4-methylphenyl]-6- (hydroxymethyl)oxane-3,4,5-triol. The drug has a molecular formula and molecular weight of C24H25FO5S and 444.5 g/ mol respectively. Its chemical structure is given in Figure 1. It melts at 68-72 deg C. Canagliflozin is practically insoluble in water (0.558 mg/L), soluble in methanol, acetone, chloroform. The logarithm partition coefficient in octanol- water is 3.44 and has estimated pKa value of 12.57.
Analytical methods to quantify Canagliflozin in biological fluids:
- Human Plasma
- Igbal, et al. [13] non-hyphenated chromatographic system (HPLC) consisting of RP-C18 column, isocratic separation at room temperature using 20 mM potassium dihydrogen orthophosphate and acetonitrile (45 : 55, v/v) at a flow rate of 1 ml/min, a total run time of about 6.0 min and a calibration range of 16.13-6000 ng/ml. Internal standard was telmisartan. Detection was done using fluorescence detector (280 and 325 nm for excitation and emission respectively). Sample preparation was by liquid-liquid extraction using diethyl ether as extracting solvent.
- Mohamed, et al. [14] hyphenated chromatographic system (LC-MS/MS) consisting of RP-C18 column, isocratic separation at room temperature composing of 0.1% formic acid and acetonitrile (60:40, v/v) as mobile phase at a flow rate of 0.5 ml/min, a total run time of about 5 min and a calibration range of 10-1000 ng/ml. Internal standard was propranolol HCl. Detection was carried out on a triple quadrupole mass spectrometer using electrospray ionization technique, operating in multiple reaction monitoring (MRM), with the transitions of m/z 462.3 → 191.0 in the positive ion mode. Sample preparation was by protein precipitation induced by acetonitrile followed by liquid-liquid extraction using ethyl acetate.
- Devineni, et al. [15] hyphenated chromatographic system (LC-MS/MS) consisting of RP-C18 column, isocratic separation at room temperature composing of 30% ammonium acetate (0.01 M) and 70% methanol as mobile phase and a calibration range of 5-10,000 ng/ml.
Internal standard was 13C6-canagliflozin. Detection was carried out on a triple quadrupole mass spectrometer using electrospray ionization technique, operating in multiple reaction monitoring (MRM), with the transitions of m/z 462.1→267.0 in the positive ion mode. Sample preparation was by liquid–liquid extraction using tert‐butylmethylether.
- Dudhe and Kamble [16] non-hyphenated chromatographic system (HPLC) consisting of RP- C18 column, isocratic separation at room temperature using 36.46 mM acetate buffer: acetonitrile: methanol (30:50:20, v/v), adjusted to pH 4,5 with acetic acid at a flow rate of 1 ml/min, a total run time of about 6.0 min and a calibration range of 33.33 – 233.33 ng/ ml. Detection was done using ultraviolet detector (290 nm). Sample preparation was by protein precipitation method using methanol as extracting solvent.
- Mabroukab, et al. [17] non-hyphenated chromatographic system (HPLC) consisting of RP-C18 column, isocratic separation at room temperature consisting of acetonitrile 0.1% - trifluoroacetic acid pH 2.5, (40:60, v/v), at a flow rate of 1 mL/min, a total run time of about 6.0 min and a calibration range of 1-2500 ng/ ml. Detection was done using diode array detector (210 nm). Sample preparation was by ultrasound-assisted dispersive liquid–liquid microextraction (UA-DLLME) using methanol as protein precipitating agent/disperser and 1-dodecanol as extracting solvent.
- Human Urine
- Devineni, et al. [15] Urine canagliflozin concentration was determined using the same sample preparation and LC–MS/MS methods under plasma determination above.
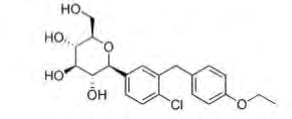
Dapagliflozin
Chemically defined as (2S,3R,4R,5S,6R)-2-[4-chloro- 3-[(4-ethoxyphenyl)methyl]phenyl]-6-(hydroxymethyl) oxane-3,4,5-triol. It has a molecular formula and molecular weight of C21H25ClO6 and 408.9 g/mol respectively. The chemical structure is given in Figure 2. It melts at 65-66 deg C. Dapagliflozin is slightly soluble in water (ca.0.173 mg/ml), soluble in methanol, acetone and other organic solvents. The logarithm partition coefficient in octanol-water is 2.7.
Analytical methods to quantify dapagliflozin in biological fluids:
- Human plasma
- JI, et al. [18] hyphenated chromatographic system (LC- MS/MS) consisting of Acquity UPLC (HSS T3) column; gradient separation at 45 deg. C using: A-water:1M ammonium acetate: acetonitrile (74.5:0.5:25), B-water:1M ammonium acetate: acetonitrile (4.5:0.5:95) at a flow rate of 1 ml/min, a total run time of about 6.0 min and a calibration range of 0.2-100 ng/ml. Detection was by quadrupole mass spectrometer using electrospray ionization technique, operating in selective reaction monitoring (SRM), with the transitions of m/z 467 → 329in the negative ion mode. Sample preparation was by protein precipitation method using acetonitrile as extracting solvent.
- Mabroukab, et al. [17] Analytical procedure is the same as canagliflozin except that the calibration (linearity) range was 3.5-2500 ng/ml.
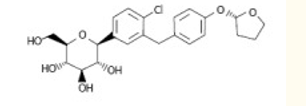
Empagliflozin
Chemically defined as (2S,3R,4R,5S,6R)-2-[4-chloro- 3-[[4-[(3S)-oxolan-3-yl]oxyphenyl]methyl]phenyl]-6- (hydroxymethyl)oxane-3,4,5-triol.Empagliflozinhas a molecular formula and molecular weight of C23H27ClO7 and 450.9 g/mol respectively. The chemical structure is given in Figure 3. It has aqueous solubility of 0.111mg/ml, soluble in organic solvents. The logarithm partition coefficient in octanol-water is 1.66 and has estimated pKa value of 12.57.
Analytical methods to quantify empagliflozin in biological fluids:
- Human Plasma
- Wattanwar, et al.[19] hyphenated chromatographic system (LC-MS/MS) consisting of RP-C18 column, isocratic separation at room temperature consisting of methanol and 10 mM ammonium trifluoroacetate (90:10, v/v) as mobile phase and a calibration range of 10.09–403.46 ng/ ml. Internal standard was empagliflozin D4. Detection was carried out on quadrupole mass spectrometer using electrospray ionization technique, operating in multiple reaction monitoring (MRM), with the transitions of m/z 468.073 → 355.100 in the positive ion mode. Sample preparation was by solid-phase extraction technique.
- Mabroukab, et al. [17] Analytical procedure is the same as canagliflozin except that the calibration (linearity) range was 2-2500 ng/ml. Although, the study has limited itself to first-line sodium glucose co-transporter 2 inhibitors, the chromatographic analytical methods discussed could also be applied in the quantification of other sodium glucose co-transporter 2 inhibitors probably with slight modification of analytical conditions.
Conclusion
Sodium glucose co-transporter 2 inhibitors are the current drugs of choice in the management of diabetes mellitus probably because of their efficacy and tolerance. These first-line SGLT 2 inhibitors have favorable physicochemical properties and their concentrations in biological fluids can easily be quantified by spectroscopic and chromatographic analytical methods. Chromatographic methods are preferred over spectroscopic methods because of their sensitivity, selectivity and specificity.
References
-
Wright EM, Loo DDF, Hirayama BA (2011) Biology of human sodium glucose transporters. Physiol Rev 91(2): 733-794.
-
Vick H, Diedrich DF, Baumann K (1973) Reevaluation of renal tubular glucose transport inhibition by phlorizin analogs. Am J Physiol 224(3): 552-557.
-
Turner RJ, Moran A (1982) Heterogeneity of sodium dependent D-glucose transport sites along the proximal tubule: evidence from vesicle studies. Am J Physiol 242(4): 406-414.
-
Rahmoune H, Thompson PW, Ward JM, Smith CD, Hong G, et al. (2005) Glucose transporters in human renal proximal tubular cells isolated from the urine of patients with non-insulin-dependent diabetes. Diabetes 54(12): 3427-3434.
-
Goldenberg R, Punthakee Z (2013) Definition, classification and diagnosis of diabetes, prediabetes and metabolic syndrome. Can J Diabetes 37: S8-S11.
-
Mohamed D, Elshahed MS, Nasr T, Aboutaleb N, Zakaria O (2019) Novel LC–MS/MS method for analysis of metformin and canaglifozin in human plasma: application to a pharmacokinetic study. BMC Chemistry 13(1): 82-92.
-
Sanagapati M, Dhanalakshmi K, Nagarjuna RG, Sreenivasa S (2014) Development and validation of stability- indicating RP-HPLC method for determination of dapagliflozin. Journal of Advanced Pharmacy Education & Research 4(3): 350-353.
-
Tahara A, Takasu T, Yokono M, Imamura M, Kurosaki E (2016) Characterization and comparison of sodium- glucose cotransporter 2 inhibitors: Part 2. Antidiabetic effects in type 2 diabetic mice. J.Pharmacol Sci 131(3): 198-208.
-
Tsimihodimos V, Panagiotopoulou T, Tzavella E, Elisaf M (2017) Clinical pharmacology of sodium glucose cotransporter 2 inhibitors. Hell J Atheroscler 8(2): 61- 72.
-
Gai MN, Pinilla E, Paulos C, Chavez J, Puelles V, et al. (2005) Determination of prednisolone and prednisone in plasma, whole blood, urine, and bound-to-plasma proteins by high-performance liquid chromatography. J Chromatogr Sci 43(4): 201-206.
-
Tonic-Ribarska J, Haxhiu A, Sterjev Z, Kiteva G, Suturkova L, et al (2012) Development and validation of a bioanalytical LC-UV method with solid-phase extraction for determination of valproic acid in saliva. Acta Pharm 62(2): 211-220.
-
Flanagan RJ, Brown NW, Whelpton R, Flanagan R, Wing B (2008) Therapeutic drug monitoring (TDM). CPD Clinical Biochemistry 9(1): 3-21.
-
Igbal M, Khalil NY, Alanazi AM, Al-Rashood KA (2015) A simple and sensitive high performance liquid chromatography assay with a fluorescence detector for determination of canagliflozin in human plasma. Analytical Methods 7: 3028-3035.
-
Mohamed D, Elshahed MS, Nasr T, Aboutalab N, Zakarla O (2019) Novel LC–MS/MS method for analysis of metformin and canagliflozin in human plasma: application to a pharmacokinetic study. BMC Chemistry 13(1): 82-92.
-
Devineni D, Curtin CR, Polidori D, Gutierrez MJ, Murphy J, et al. (2013) Pharmacokinetics and pharmacodynamics of canagliflozin, a sodium glucose co‐transporter 2 inhibitor, in subjects with type 2 diabetes mellitus. The Journal of Clinical Pharmacology 53(6): 601-610.
-
Dudhe PB, Kamble MC (2016) RP-HPLC method development and validation forthe determination of canagliflozin in human plasma. Int J Pharm Tech Res 9(8): 174-181.
-
Mabroukab MM, Solimanc SM, El-Agizyc HM, Mansourab FR (2020) Ultrasound-assisted dispersive liquid–liquid microextraction for determination of three gliflozins in human plasma by HPLC/DAD. J Chromatogr B, pp: 1136.
-
JI QC, Xu X, Ma E, Liu J, Basdeo S, et al. (2015) Selective reaction monitoring of negative electrospray ionization acetate adduct ions for the bioanalysis of dapagliozin in clinical studies. Anal Chem 87(6): 3247-3254.
-
Wattanwar T, Mungantiwar A, Halde S, Pandita N (2019) Development of simultaneous determination of empagliflozin and metformin in human plasma using liquid chromatography-mass spectrometry and application to pharmacokinetics. Eur J Mass Spectrometry 26(2): 117-130.
- Spectrophotometric Determination of Lanthanum (III) and Some Rare Earths with Xylenol Orange
- Introduction and Sources of Molluscicides
- Trimetazidine: An Antianginal Drug and Not Only!
- Nature Inspired Discovery and Development of Antibacterials: An Update
- Fungal Biodegradation of Polycyclic Aromatic Hydrocarbons (PAHs)
- Recent Approaches of Impurity Profiling in Pharmaceutical Analysis: A Concise Review