Spontaneous Necrosis of Hepatocellular Carcinoma and Necrosis Partial of Lymphatic Metastasis: Reported Case
We present the case of a 57 years old woman with chronic HCV infection in non-cirrhotic liver with casual detection of a space-occupying lesion (SOL) with loco regional adenopathies of atypical features. Since radiological characteristics were not conclusive, a biopsy and subsequent surgical resection of the lesion and the multiple adenopathies were needed to establish diagnosis. The histological analysis showed complete necrosis of the SOL, with a focus of poorly differentiated hepatocellular carcinoma (HCC) in two of the adenopathies. We report the evolution of a histologically confirmed rare case of hepatocellular carcinoma, proposing a pathophysiological hypothesis and the possible implications that may have for his future treatment.
Introduction
Hepatocellular carcinoma (HCC) is the most frequent malignant liver tumor and one of the main causes of death due to cancer in the world, especially in Asian countries. Its incidence continues to increase over time all over the world and in parallel with mortality [1]. This is so, because, in spite of the recommendations of screening in patients with cirrhosis of any etiology and in those with HCV infection and advanced fibrosis, more than half of the cases are diagnosed in advanced stages, which results in worse prognosis, with no possibility of curative treatment [2]. The spontaneous regression of cancer was first described in 1956 by Cole and Everson [3] as the partial or complete disappearance of a malignant tumor in the absence of specific treatment. It has been described in cases of renal tumor, neuroblastoma, melanoma, HCC…. However, the spontaneous regression of HCC is still considered a rare event, with a reported incidence of 1 per 140,000 cases [4], without underlying cause identified in the majority of cases. Several mechanisms have been suggested to explain regression including tumorischemia (thrombosis, rapid neoplastic growth, gastrointestinal bleeding), fever, various procedures (transfusion, angiography), consumption of medicinal herbs, alcohol withdrawal and the activation of the immune system [5]. Ischemia and immune activation mechanisms are considered the most frequently responsible. However, in the majority of cases regression mechanisms are unknown due to the lack of histological studies.
Clinical Case
We present the case of a 57 old year’s woman with chronic HCV infection in follow-up for many years. She had been treated with peg interferon and ribavirin for 48 weeks showing recurrence of infection after six months. She underwent hemithyroidectomy few months before due to the presence of a nodule that showed no sign of malignancy after histologic analysis. She continued treatment with lithium for bipolar disorder, hormone replacement for hypothyroidism and amiloride for HT. Transition elastography (Fibroscan™) showed 10 Kpa (F3) with normal abdominal ultrasounds until the end of 2015. A new abdominal ultrasound showed a poorly demarcated space-occupying lesion hepatic of 28 x 29 mm, without acquisition with color Doppler. The study revealed the presence of pathological adenopathies (prior to the portal vein a hypoechogenic adenopathy of 35x14 mm and another similar of 21 x15.6 mm). The study was completed with chest CT scan that showed no alterations and MRI of the liver where a liver lesion of 3 cm was found in segment VIII, of low signal on T1 and T2, with restrictions on the diffusion and minimum intravenous contrast uptake in relation to hypovascular lesion and without portal hypertension (Figures 1 & 2).
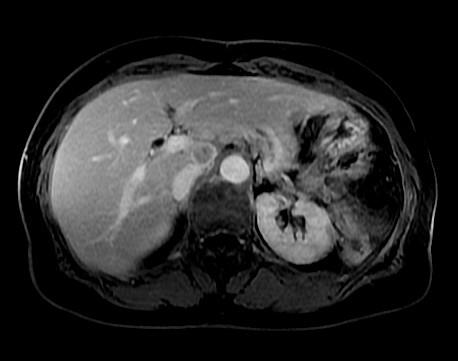

Figure 2: MRI of the liver showing the presence of a pathological hilar adenopathy of about 13 mm, suspicious of necrosis and with peripheral capsule effect, similar to the primary liver lesion. The analytical study showed thrombocytopenia 118,000 platelets/mm3, normal coagulation study, GOT 26 U/L, GPT 28 U/L, GGT, 30 U/L, Falc 75 U/L, BRB total 0.61 mg/dl; ferritin 275 mg/dl and Alpha fetoprotein 6.38 ng/ml. A biopsy of the hepatic lesion was scheduled, obtaining a cylinder of liver parenchyma with presence of cytokeratins suggestive of neoplasicnecrosis and without viable tumor cell population. The hepatic segment VIII, the gallbladder and adenopathies of the celiac trunk and the hepatic artery were resected. The immunohistochemical profile, of a cluster of lymph nodes located at the hepatic hilum and another adenopathy in the aortocavalinter-space, were consistent with nodal metastasis of poorly differentiated carcinoma compatible with HCC (Figure 3). It expressed cytokeratin AE1/AE3, 18 cam5.2, CK, CK 19 (focal), arginase deficiency (cytoplasmic droplets), AFP, Heppar-2 (focal), glypican-3 (focal) and TTF-1 (cytoplasmic). The lesion hepatic showed complete tumor necrosis with free surgical margins and the adjacent hepatic parenchyma showed a portal chronic hepatitis with minimal fibrosis.
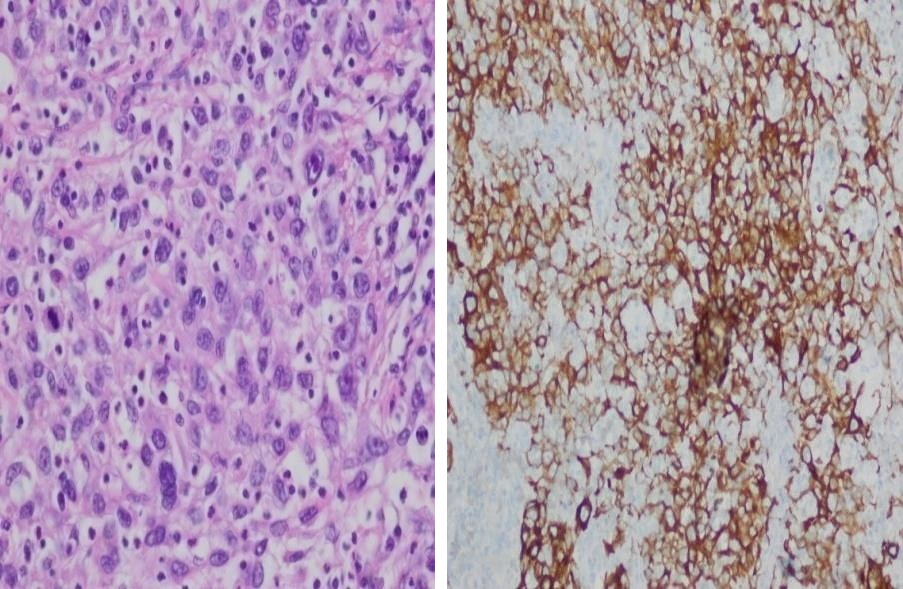
Figure 3: Histological and immunohistochemical analysis of lesions. Left panel shows the nodal metastasis of poorly differentiated hepatocellular carcinoma. Right panel, immunehistochemical stainings showing CK18 expression. Two months after the surgery, new focal lesions we’re not visible, in the liver by MRI, but at least two adenopathies of significant size had grown in the portacaval and retropancreatic space. Based on the evidence of progression and the recommendations of the experts to carry out a treatment similar to that of typical HCC, the patient was treated with the inhibitor of angiogenesis, Sorafenib. She developed a constitutional syndrome with poor control of hypertension and skin erythema on palms and soles, followed by painful erythroderma and desquamation of skin and/or development of bullous lesions, despite the reduction of sorafenib doses to half. After two months of intermittent treatment with poor tolerance, the treatment was suspended to include the patient in a clinical study for second-line therapy.
Discussion
The majority of the cases of HCC develop from cirrhosis or chronic liver disease with advanced fibrosis (F3) associated with viral infection (HCV, HBV), consumption of alcohol or fat deposition disease (NASH) [1]. For this reason, clinical guidelines recommend screening for HCC by ultrasound every six months in this group of patients [6]. However, it is not exceptional to find cases of HCC on non-cirrhotic livers, especially in patients with NASH or with HBV infection, which makes more difficult the diagnosis and the possibility of treatment in early
stages. Our case had an HCV infection of long evolution with mild fibrosis as determined by biopsy. However the study by transient elastography showed a more advanced fibrosis (F3) and the patient was included in the screening program. Even so, at the time of diagnosis presented disseminated neoplasm, indicating a rapid evolution. The diagnosis of HCC is usually based on the detection of a hepatic mass of great size and/or multifocal hypervascular liver nodules, in patients with chronic liver disease (asymptomatic), and generally cirrhotic. It is accepted by different clinical guidelines to perform the diagnosis by hyper enhancement in arterial phase with early washing in the portal phase and hyperintensity on T2-weighted MRI and CT, without the realization of histological study [6, 7]. The cases of spontaneous regression of HCC described in the literature are scarce, and they are considered a possible but unlikely evolution of hepatocellular carcinoma as in our clinical practice. The clinical description varies widely among the different studies, including the complete or partial remission of single or multiple lesions and its association or not with extra hepatic metastases. In more than 40% of the cases it is not possible to determine the cause of regression since histological studies are generally not available or, as in our case, when available they do not show conclusive findings about the possible etiology because of insufficient cell sample.
Ischemia has been described among the factors involved in regression; in fact some of the cases described above showed the presence of vascular thrombi, a peripheral capsule or large lesions with rapid neoplastic growth and insufficient blood supply to a tumor with a high metabolic rate [8]. In other cases the activation of certain types of cells involved in the hostdefense (CD163+ macrophages, T lymphocytes cytotoxic) directed against tumor specific antigens (eg. GPC3) point to an immune origin [8, 9]. Our patient showed simultaneously necrosis of the hepatic lesion and partial necrosis of the adenopathies without prior treatment, consumption of herbal products or procedures which might have a low output. The poorly differentiated HCC found in the adenopathies allowed establishing the diagnosis, but not the cause of regression as lesions had a low cellular component. It has been described regression of metastases after resection of the primary tumor due to the disappearance of the immune suppression induced by the original tumor. In our case the necrosis of the lesions could be secondary to a recovery of the immune response, but we do not know the stimulus that could have triggered. Hepatocytes and other non-parenchymal cells play a regulatory immune role acting as antigen-presenting cells (APCS). It is postulated that after a liver damage, altered hepatocytes can express molecules of the type II major his to compatibility complex (MHC) presenting antigen to "naive" T lymphocytes. Due to the absence of appropriate interaction with a coactivator, this antigen presentation may induce tolerance in T lymphocytes toward mutant and/or aberrant tumor-associated antigens. This could be a mechanism by which HCC evades the endogenous immune response [9]. One of the identified tumor associated antigens target for immunotherapy in HCC is the membrane linked heparan sulfate proteoglycan glypican-3(GPC3). It is expressed in more than 80% of HCC and is associated with lower survival and therefore worse prognosis. In our case it was possible to determine the presence of this antigen in focal form, thus confirming the initial poor prognosis. This microenvironment of immune tolerance that suppressed the function of the effector cells may be modified by immune adjuvant therapy to restore the function of these lymphocytes and to limit and suppress tumor progression [8]. Nowadays, the immunotherapy treatments are based on this mechanism induced by the use of antigen-specific human or humanised monoclonal antibodies directed against different targets such the GPC3.This immunotherapy in addition a direct antitumor effect can increase the susceptibility of HCC to chemotherapy (sorafenib) when both treatments are combined. Studies with the use of different monoclonal antibodies (tremelimumab, nivolumab) are being carried out, with promising results in the response and control of HCC [10]. It is important to increase the knowledge of the inflammatory response associated with the tumor and the mechanism that enables to restore an effective immune response. A more detailed analysis of all cases in which the histological studies are available can help us to improve this broad field, increasing the therapeutic possibilities for metastatic HCC.
References
-
El Sherag HB (2012) Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology 142(6): 1264-1273.
-
Varela M, Reig M, De la Mata M, Matilla A, Bustamante J, et al. (2010) Treatment approach of hepatocellular carcinoma in Spain. Analysis of 705 patients from 62 centers. Med Clin (Barc) 134(13): 569-576.
-
Everson TC, Cole WH (1956) Spontaneous regression of cancer: preliminary report. Annals of Surgery 144(3): 366-383.
-
Tamiko Saito, Masafumi Naito, Yuki Matsumura, Hisaaki Kita, Tomoyo Kanno, et al. (2014) Spontaneous regression of a large Hepatocellular Carcinoma with multiple lung metastases. Gut and liver 8(5): 569-574.
-
Shunichi Matsuoka, Akinori Tamura, Mitsuhiko Moriyama, Hirotoshi Fujikawa, Kenji Mimatsu, et al. (2015) Pathological evidence of the cause of spontaneous regression in a case of resected hepatocellular carcinoma. Internal Medicine 54: 25- 30.
-
European Association for the Study of the Liver, European Organization for Research and Treatment of Cancer (2012) EASL- EORTC clinical practice guidelines: management of hepatocellular carcinoma. Journal of Hepatology 56(4): 908-943.
-
Heimbach JK, Kulik LM, Finn R, Sirlin CB, Abecassis M, et al. (2017) AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology.
-
Wang Z, Ke ZF, Lu XF, Luo CJ, Liu YD, et al. (2015) The clue of a possible etiology about spontaneous regression of hepatocellular carcinoma: a perspective on pathology. Onco targets and therapy 8: 395-400.
-
Miamen AG, Dong H, Roberts LR (2012) Inmunotherapeutic approaches to hepatocellular carcinoma treatment. Liver Cancer 1(3-4): 226-237.
-
Trojan J, Waidmann O (2016) Role of regorafenib as second-line therapy and landscape of investigational treatment options in advanced hepatocellular carcinoma. Journal of Hepatocellular Carcinoma 3: 331-36.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey