Ultrasound Diagnosis in Assessment of Structures and Functional Disorders in Distal Gastric Cancer
Objective: To evaluate the diagnostic possibilities of transabdominal ultrasonography for evaluation of severity of structures and functional disorders in distal gastric cancer (DGC). Materials and Methods: An analysis of transabdominal ultrasonography of 48 patients with distal gastric carcinoma was performed. 29 (60,4%) cases were males (mean age 61.9 years) and 19 (39,6%) females (mean age 58.2 years). All patients were on surgical treatment. All patients underwent preoperative X-ray, virtual gastroscopy techniques, multidetector computed tomography and transabdominal ultrasonography (USG). Results: Histologically, in 45 (93,8%) cases adenocarcinoma, in 3 (6,2%) – ring-cell carcinoma (cricoidal) gastric cancer was established. Ulcerating infiltrating forms in 35 (72,9%) cases and diffusely infiltrating – in 13 (27,1%) cases was diagnosed. The stage of T2 – in 6 (12,5%) cases, the stage of T3 – in 23 (47,9%) cases and the stage of T4 – in 19 (39,6%) cases were identified. In 41 (85.4%) cases, pyloric stenos was diagnosed - of them in 9 (22.0%) it was compensated, in 24 (58.5%) - sub compensated and in 8 (19.5%) - decompensated. Conclusions: 1. The expansion of the depth and extent of tumor infiltration is accompanied by an increase in the severity of pyloric stenosis. 2. At the compensation stage, the evacuation rate, the amplitude of peristalsis, the volume of stomach contents on an empty stomach increases to 50 ml. 3. During decompensation, the stomach volume of fasting is more than 120ml, the amplitude of peristalsis and the rate of evacuation decrease sharply. 4. The use of the color Doppler method in the upright position of the patient immediately after taking the liquid made it possible to visualize the pylorus as a colored tubular structure.
Introduction
Gastric carcinoma (GC) is one of the most common causes of cancer-related death worldwide. Surgical resection is the only cure available and is dependent on the GC stage at presentation, which incorporates depth of tumor invasion, extent of lymph node and distant metastases. Accurate preoperative staging is therefore essential for optimal surgical management with consideration of preoperative and/or postoperative chemotherapy [1]. Though a marked reduction has been observed in the incidence of gastric carcinoma in North America and Western Europe in the last 50 years, 5-year survival rates are less than 20%, as most patients present late and are unsuitable for curative, radical surgery. That is an aggressive carcinoma with 5-year survival rates ranging from 3% in the case of stage IV tumors to 85– 90% in the case of stage I tumors. The most commonly used staging system for GC was developed by the American Joint Committee on Cancer (AJCC) [2, 3]. Gastric cancer is the fourth most common cause of cancer-related death in the world, and it remains difficult to cure in Western countries, primarily because most patients present with advanced disease [4]. In the United States, stomach malignancy is currently the 15th most common cancer. Japan and South Korea, two countries that have high rates of the disease, screen for stomach cancer [5]. Gastric adenocarcinoma is a malignant epithelial tumour, originating from glandular epithelium of the gastric mucosa. Stomach cancers are overwhelmingly adenocarcinomas (90%) [6]. Adenocarcinomas account for 95% of all gastric cancers (GCs). Based on the level of invasion, GCs are divided into early gastric cancer (EGC) and advanced gastric cancer (AGC). EGC or the superficial form is limited to the mucosa and submucosa, regardless of the presence or absence of lymph node metastases and can appear as a small circumscribed, sometimes ulcerated thickening of the gastric wall. AGC involves the muscularis propria or beyond and can be polypoid, ulcerating, ulcerating infiltrating and diffusely infiltrating. Histologically, GC is usually classified into intestinal or diffuse histologic forms. The intestinal type is presumed to arise from intestinalized gastric mucosa and they are usually nodular, polypoid, or fungating. The diffuse type is grossly ill defined and may have the appearance of a plaque or linitis plastica [7]. Upper gastrointestinal endoscopy is the preferred technique for detection of GC which is also useful in obtaining histological confirmation of suspicious gastric lesions. However, up to 6.7% of GCs may be missed when an endoscopy shows no initial cancer findings [8]. Imaging techniques are useful for staging the already detected GC but can also occasionally detect unsuspected cancers. Several studies have reported accuracy up to 90% or more with MDCT for detection of GC with the use of multiplanar reconstruction (MPR) and virtual gastroscopy (VG) techniques [9, 10, 11, 12]. Tumor lesions of the distal stomach are often enough. Pyloric tumors are slightly less antral and occupy approximately 6-14% of cases from all carcinomas of the stomach. The distal localization of cancer contributes to the early appearance of obstruction symptoms even in small tumor sizes. The appearance of "early" clinical symptoms makes the patients consult a doctor. At the same time, a predominantly infiltrative form of cancer with an endophytic location prevents their detection during radiography and endoscopy. For a long time, the diagnosis of these tumors becomes difficult. Very often, with such a localization of cancer, a peptic ulcer is falsely diagnosed, which is mistakenly considered the cause of pyloric stenosis. At this time, the tumor continues to increase in thickness and aggravates stenosis. In all this, a significant role is played by cancers such as linitis plastic [13]. The most frequent complaints of patients with distal stomach cancer are pain and a feeling of heaviness in epigastrium, toshnata, deterioration of appetite and weight loss. Thanks to the early appearance of complaints, patients turn to the doctor earlier than when the cancer is localized, for example, in the area of the body and the large curvature of the stomach. Therefore, the results of subtotal resection of the stomach in distal cancer are better than in other localizations. However, the presence of pyloric stenosis significantly worsens the prognosis. The results of the studies by Chen J.N. et al. (2007) showed that 5-year survival in patients with distal cancer in combination with pyloric stenosis was significantly worse than without pyloric stenosis. In the presence of pyloric stenosis, invasion of the surrounding tissue is much deeper, and these patients often have metastasis to the lymph nodes in the retropancreatic zone [14]. One of the peculiarities of distal stomach cancer is that, due to deformity of the stomach, narrowing of the lumen makes it difficult to carry out endoscopy and receive a biopsy material, which is very important for the oncologist. In such cases, the X-ray examination is also complicated, since the stenosis of the outlet is accompanied by ectasia of the stomach with the presence of food, liquid, and mucus in it. In this case, it becomes impossible to tightly fill the gastric outlet with excessive barium suspension, which reduces the effectiveness of diagnosis [15]. Currently, ultrasonography for the study of the stomach is not yet used in connection with a skeptical attitude to the possibilities of the method. However, in separate publications, the role of transabdominal ultrasonography in the visualization of the stomach walls, the differentiation of wall layers and the diagnosis of adenocarcinoma of the antrum by gastic cancer is shown [16, 17, 18, 19]. Objective: To evaluate the diagnostic possibilities of transabdominal ultrasonography for evaluation of severity of structures and functional disorders in distal gastric cancer.
| MPR: Multiplanar Reconstruction; VG: Virtual | |
|---|---|
| Gastroscopy. |
Materials and Methods
An analysis of transabdominal ultrasonography of 48 patients with gastric carcinoma was performed. 29 (60,4%) cases were males (mean age 61.9 years) and 19 (39,6%) females (mean age 58.2 years). All patients were on surgical treatment at the Kharkov Regional Oncology Center (Ukraine). Histologically, in 45 (93,8%) cases adenocarcinoma, in 3 (6,2%) – ring-cell carcinoma (cricoidal) gastric cancer was established. In all cases advanced gastric cancer (AGC) of diffuse forms was diagnosed. Ulcerating infiltrating forms in 35 (72,9%) cases and diffusely infiltrating – in 13 (27,1%) cases was diagnosed. According to the classification of the American Joint Committee on Cancer (AJCC) [3], the stage of T2 – in 6 (12,5%) cases, the stage of T3 – in 23 (47,9%) cases and the stage of T4 – in 19 (39,6%) cases were identified. The clinical symptoms of the pyloric stenosis was registerede in 43 (89,6%) cases – in T2 stage of tumor in 1 (2,1%) case and in all cases of T3 and T4 stages (Table 1). All patients underwent preoperative X-ray and multi detector computed tomography with the use of multiplanar reconstruction. Virtual gastroscopy was performed in 41 patients, because in 7 patients due to severe pyloric stenosis it was not possible to hold an endoscope in the pyloric department. Normal ultrasound semiotics was studied in 36 patients without gastric pathology. Ultrasound was carried out in the frequency range 4-7 MHz in B and color Doppler in the patient's position lying on his back, on his side, standing, on an empty stomach and after filling 500 ml with warm boiled water.
- Distal cancer
- Clinical symptoms of
- Stage of carcinoma pyloric stenosis
- 48
- 43 (89,6±4,4%)
- T2
- 6 (12,5±4,8%)
- 1 (2,1±2,1%)
- T3
- 23 (47,9±7,2%)
- 23 (47,9±7,2%)
- T4
- 19 (39,6±7,1%)
- 19 (39,6±7,1%)
Table 2: Localization and stage of distal gastric cancer
Results
After contrasting, the unchanged stomach wall has a layered structure 2.5 mm thick in the body, up to 4-5 mm in the antrum. In the anterior wall of the abdominal part of the esophagus, there is also a false "thickening" caused by projection distortion. At the time of peristaltic waves, there is also a thickening of the wall, which disappears after a few seconds. The layered structure of the stomach in the antrum and the body was noted in all cases. In the fundus and greater curvature, due to the projection distortion and the depth of the object's location, the layers of the stomach wall were not differentiated, at the same time there was no local thickening (Figure 1).
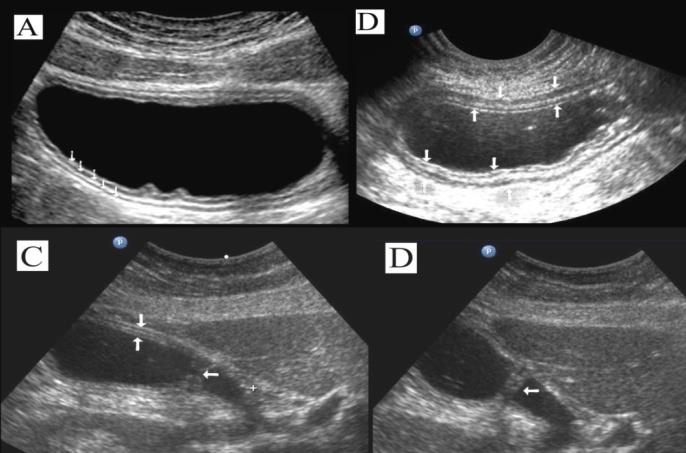
Figure 1: Ultrasonogram of the stomach for various projections of scanning and degree of filling. A: The arrows show all layers of the stomach wall at the body level in the transverse section. B: Partial emptying of the stomach, all layers of the wall is clearly differentiate. С: The vertical arrows show the anterior wall of the antrum, the horizontal arrows – pyloric, which is not fully open. D: The same, pyloric is closed. To diagnose distal stomach cancer and assess the degree of stenosis, the following echographic symptoms were used:
- Presence of parietal formations protruding into the cavity of the stomach outside peristaltic waves.
- Deterioration or absence of differentiation of the layers of the stomach wall.
- Local thickening of the stomach wall more than 6 mm.
- Local reduction or absence of peristaltic waves.
5. Amplitude of peristaltic waves above the area of damage. 6. The maximum thickness and extent of the affected area of the stomach. 7. The maximum diameter of the pyloric canal in the vertical position of the patient. In healthy individuals, all layers of the stomach wall were differentiated clearly. The thickness of the wall at the level of the body of the stomach was 3-4 mm, at the level of antrum 4-6 mm, the length of the pylorus before the evacuation of the liquid 18-22 mm, the width of the pylorus more than 16 mm, the evacuation rate 21 ± 3 cm / s, the peristalsis amplitude 11±2 mm. After 25-30 minutes after receiving the liquid, the stomach volume averaged 246±19 ml, after an hour - 138±27 ml. Ulcerative infiltrative forms of gastric cancer was recorded in 34 cases: the stage of T2 – in 4 (11,8±5,5%) cases, T3 – in 17 (50,0±8,6%) cases and T4 – in 13 (38,2±8,3%) respectively. Diffuse infiltrative forms of gastric cancer was recorded in 14 cases: the stage of T2 – in 2 (14,3±9,4%) cases, T3 and T4 in 6 (42,9±13,2%) respectively. Virtual gastroscopy (GS) was performed in 41 patients, because in 7 patients due to severe pyloric stenosis it was not possible to hold an endoscope in the pyloric department. GS was performed in 4 (11,8 ± 5,5%) cases of stage T2, in 16 (47,1 ± 8,6%) cases of T3 and in 9 (26,5 ± 7,6%) cases of T4 stage of ulcerative infiltrating forms of stomach cancer. Among the patient of diffuse infiltrating form of gastric cancer GS was performed in 2 (14,3±9,4%) cases of T2, in 5 (35,7±12,8%) cases of T3 and T4 stages respectively (Table 2).
| Diffuse forms (n=94) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Stage of | ||||||||
| Ulcerative infiltrating forms (n=34) | Diffuse infiltrating forms (n=14) | |||||||
| carcinomas | ||||||||
| Ultrasonography | Gastroscopy | Ultrasonography | Gastroscopy | |||||
| T2 (n=10) | 4 (11,8±5,5%) | 4 (11,8±5,5%) | 2 (14,3±9,4%) | 2 (14,3±9,4%) | ||||
| T3 (n=38) | 17 (50,0±8,6%) | 16 (47,1±8,6%) | 6 (42,9±13,2%) | 5 (35,7±12,8%) | ||||
| T4 (n=45) | 13 (38,2±8,3%) | 9 (26,5±7,6%) | 6 (42,9±13,2%) | 5 (35,7±12,8%) |
Table 3: Ultrasonographic and Gastroscopic diagnosis of different hystological forms and stage of gastric carcinomas. In 41 cases
Table 2: Ultrasonographic and Gastroscopic diagnosis of different hystological forms and stage of gastric carcinomas. In 41 cases pyloric stenosis was diagnosed - of them in 9 (22,0%) it was compensated, in 24 (58,5%) - subcompensated and in 8 (19,5%) - decompensated. The layers of the wall were not differentiated in all patients with gastric cancer. With compensated pyloric stenosis, the thickness of the affected area was
9,8±2,7mm, the length was 26,7±5,9mm, the diameter of the pylorus was 8,2±0,9mm, the evacuation rate was 31±3cm/s, the stomach volume on an empty was 39±6ml, 30 minutes after taking the fluid - 263±24ml, after an hour - 214±18ml, the amplitude of peristalsis - 19±3mm, respectively (Figures 2 & 3).
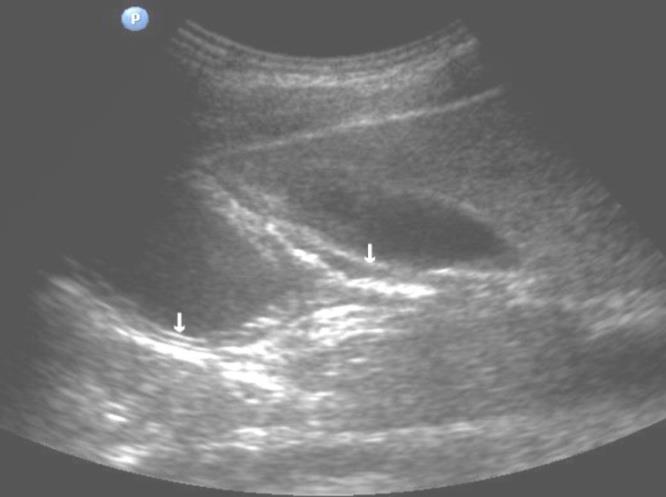
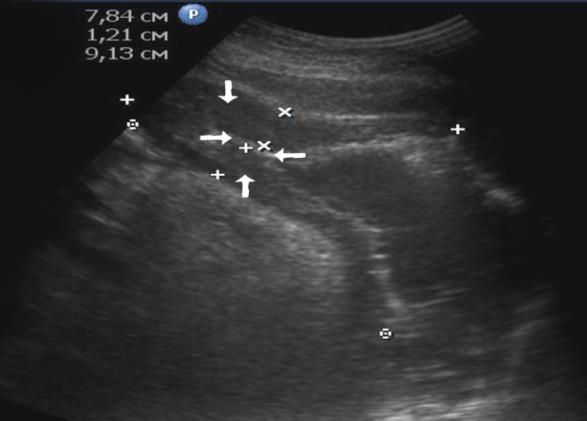
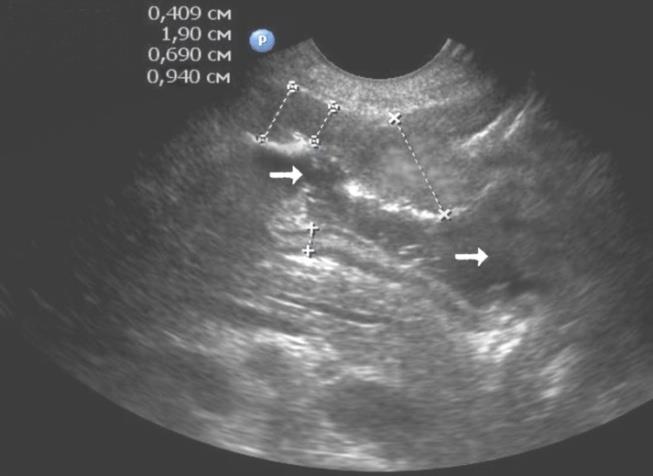
Figure 3: Echogram of the patient with the antrum adenocarcinoma with compensated pyloric stenosis. The thickness of the intact section of the stomach is 0,409cm, the anterior wall of the antrum is 0.94cm, the stenotic region is 0.69cm, and the peristalsis amplitude is 1.90cm. The arrows show the gastric cavity. Among patients with sub compensated pyloric stenosis, the thickness of the stomach wall was 19,2±3,8mm, the length was 42,8±4,3mm, the pyloric diameter was 4,5±1,2mm, the evacuation rate was 34±5cm/s, the volume of fasting contents 137±31ml, after 30 minutes after fluid intake - 294±31ml, after an hour - 265±27ml, the amplitude of peristalsis - 13±4mm, respectively.
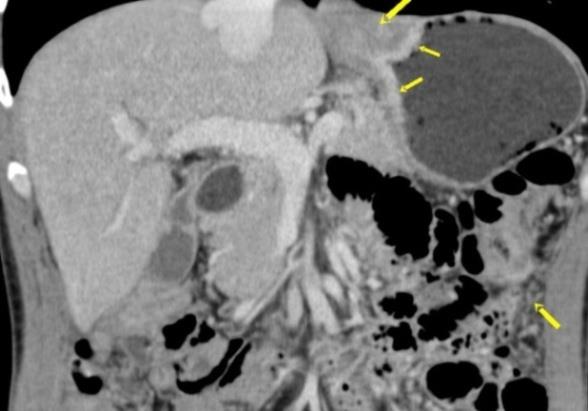
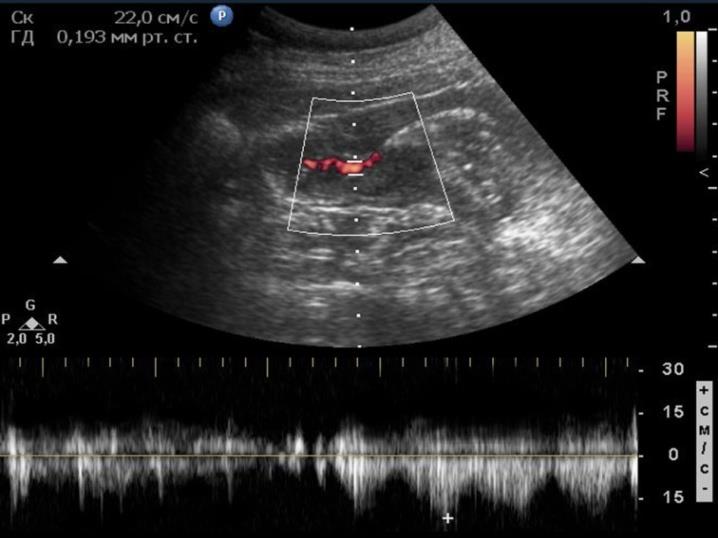
The thickness of the affected region of the outlet part of the stomach with decompensated pyloric stenosis was 31,2±4,8mm, the length was 59,7±8,1mm, the pyloric diameter was 2,4±0,9mm, the residual volume of the stomach on an empty stomach was 335±32ml, 30 minutes after receiving fluid - 351±29ml, after an hour - 305±32ml, the amplitude of peristalsis is 3,7±1,4mm, the evacuation rate was 20±3cm/s. With decompensated pyloric stenosis, the pylorus in two-dimensional ultrasound mode and computed tomography is very poorly identified. In color Doppler mode, in the vertical position of the patient after receiving fluid, one can see a very narrow stream of fluid flow through a significantly stenosed pylorus (Figures 4-7).

| Stage of gastric | Computed | |||||||
|---|---|---|---|---|---|---|---|---|
| Ultrasonography | ||||||||
| carcinoma | tomography | |||||||
| T2 (n=7) | 6 (85,7±13,2%) | 5 (71,4±17,1%) | ||||||
| T3 (n=36) | 36 (100,0±1,7%) | 36 (100,0±1,7%) | ||||||
| T4 (n=41) | 38 (92,7±4,1%) | 41 (100,0±1,6%) |
Table 4: Comparison of results of ultrasonography and computed tomography in the diagnosis of gastric carcinoma.
Discussion
Gastroscopy is a method of choosing a diagnosis of gastric carcinoma [17]. However, the method does not allow visualizing the layers of the stomach wall, which is necessary for determining the stage of the tumor process. Computed tomography is the main method of diagnosing the stage and prevalence of stomach cancer on the surrounding organs - the liver, pancreas, lymph nodes, lungs and others [20]. The conducted researches in recent years show the wide possibilities of ultrasonography in the differentiation of the stomach wall layers, in the diagnosis of infiltrative forms of gastric carcinoma [21]. At T3 and T4 stages of stomach cancer, the layers of its wall do not differentiate. We compared the possibility of ultrasonography and computer tomography in assessing the thickness and extent of distal gastric cancer, and there were no statistically significant differences between their results. At T4 stages of gastric cancer, metastases to the pancreas and par pancreatic lymph nodes were better diagnosed using computed tomography. With decompensated pyloric stenosis, ultrasonography in B mode and computed tomography did not allow the pylorus to be determined accurately. The use of the color Doppler method in the upright position of the patient immediately after taking the liquid made it possible to visualize the pylorus as a colored tubular structure.
Conclusions
- The expansion of the depth and extent of tumor infiltration is accompanied by an increase in the severity of pyloric stenosis.
- At the compensation stage, the evacuation rate, the amplitude of peristalsis, the volume of stomach contents on an empty stomach increases to 50 ml.
- During decompensation, the stomach volume of fasting is more than 120ml, the amplitude of peristalsis and the rate of evacuation decrease sharply.
- The use of the color Doppler method in the upright position of the patient immediately after taking the liquid made it possible to visualize the pylorus as a colored tubular structure.
References
-
James Thomas Patrick Decourcy Hallinan, Sudhakar Kundapur Venkatesh (2013) Gastric carcinoma: imaging diagnosis, staging and assessment of treatment response. Cancer Imaging 13(2): 212-227.
-
Jemal A, Bray F, Center MM, Ferlay J, Ward E, et al. (2011) Global cancer statistics. CA Cancer J Clin 61(2): 69-90.
-
Edge SB, Compton CC (2010) The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 17(6): 1471-1474.
-
Orditura M, Galizia G, Sforza V, Gambardella V, Fabozzi A, et al. (2014) “Treatment of gastric cancer”. World Journal of Gastroenterology 20(7): 1635-1649.
-
(2014) World Cancer Report 2014. World Health Organization. pp: 630.
-
Kumar (2010) Pathologic Basis of Disease. 8th (Edn.), Saunders Elsevier, pp: 784.
-
Hallinan JT, Venkatesh SK (2013) Gastric carcinoma: imaging diagnosis, staging and assessment of treatment response. Cancer Imaging 13: 212-227.
-
Raftopoulos SC, Segarajasingam DS, Burke V, Ee HC, Yusoff IF (2010) A cohort study of missed and new cancers after esophagogastroduodenoscopy. Am J Gastroenterol 105(6): 1292-1297.
-
Kim YH, Lee KH, Park SH, Kim HH, Hahn S, et al. (2009) Staging of T3 and T4 gastric carcinoma with multidetector CT: added value of multiplanar reformations for prediction of adjacent organ invasion. Radiology 250(3): 767-775.
-
Yang DM, Kim HC, Jin W, Ryu CW, Kang JH, et al. (2007) 64 multidetector-row computed tomography for preoperative evaluation of gastric cancer: histological correlation. J Comput Assist Tomogr 31(1): 98-103.
-
Yan C, Zhu ZG, Yan M, Zhang H, Pan ZL, et al. (2009) Value of multidetector-row computed tomography in the preoperative T and N staging of gastric carcinoma: a large-scale Chinese study. J Surg Oncol 100(3): 205-214.
-
Moschetta M, Stabile Ianora AA, Anglani A, Marzullo A, Scardapane A, et al. (2010) Preoperative T staging of gastric carcinoma obtained by MDCT vessel probe reconstructions and correlations with histological findings. Eur Radiol 20(1): 138-145.
-
Cabebe EC, Mehta VK, Fisher G, Talavera F, Movsas M, et al. (2014) “Gastric Cancer”. Medscape Reference.
-
Chen JN, Cheng Ven Wu, Lo SS, Lui WY, MC Hsieh, et al. (2007) Outcome of distal gastric cancer with pyloric stenosis after curative resection. European Journal of Surgical Oncology 33(5): 556-560.
-
Portnoy LM, Vyatchanin OV, Stashuk GA (2004) New views on radiation diagnostics of stomach cancer (methodological-semiotic and organizational aspects, OOO Vidar-M Publishing House, pp: 278.
-
Abdullaev R Ya, Vinnik Yu A, Spuzyak MI, Gapchenko VV (2009) Ultrasonography of the stomach and duodenum. Kharkov, pp: 104.
-
Thrumurthy SG, Chaudry MA, Hochhauser D, Ferrier K, Mughal M, et al. (2013) The diagnosis and management of gastric cancer. British Medical Journal 347: f6367.
-
Virmani V, Khandelwal A, Sethi V, Fraser-Hill M, Fasih N, et al. (2012) Neoplastic stomach lesions and their mimickers: Spectrum of imaging manifestations. Cancer Imaging 12(1): 269-278.
-
Bakkelund KE, Nordrum IS, Fossmark R, Waldum HL (2012) Gastric Carcinomas Localized to the Cardia. Gastroenterology Research and Practice 2012(2012): 6.
-
Lim JS, Yun MJ, Kim MJ, Hyung WJ, Park MS, et al. (2006) CT and PET in stomach cancer: preoperative staging and monitoring of response to therapy. Radiographics 26(1): 143-156.
-
Abdullaev R Ya, Kryzhanovskaya IV, Dynnik OB, Mechev DS (2014) Features of ultrasound diagnosis of gastric and colon cancer. Radiation diagnostics, radiation therapy 4: 27-33.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey