About 54 Cases of Neuromeningtic Cryptococcosis on HIV Infection
Introduction: The advent of antiretrovirals has reduced the prevalence of neuroméningated cryptococcosis (CNS) in patients living with HIV (PLHIV). Objectives: Epidemiological-clinical, paraclinical, therapeutic and evolutionary analysis of 54 cases of CNM in PVVIH. Patients and methods: A retrospective study reporting cases of CNM in patients living with HIV (PLWHIV) collected between January 01, 1993 and June 30, 2017 at the national reference center for the management of HIV infection; EHS service B El Hadi Flici ex EL KETTAR, Algiers. Results: In a group of 1289 PPVIH, 4.2% presented a CNM. The mean age was 39 ± 2years with a sex ratio of (3.15). The CNM was inaugural of HIV infection in 41%. The dominant picture: meningoencephalitis in 50% of cases, febrile headache 28%, fevers isolated 11%, headache isolated 9% and one asymptomatic case. The stiffness of the neck found in fourteen patients. Note that 04 patients developed disseminated form. In 51 lumbar punctures performed, the cephalospinal fluid (LCS) was pathological in 61%, with a clear appearance of 86%. Mean cytoracy: 60 cells / mm3 predominantly lymphocytic in 19 patients. Hyperproteinorachia was found in 18 patients with an average of 0.73 g / l. Hypoglycorachia in 14 patients with an average of 0.36 g/l. direct examination with Indian ink staining identifies Cryptococcus neoformans in 61% of cases, culture on Sabouraud medium supplemented with chloramphenicol positive 80.3%. The search for soluble cryptococcal antigens by the latex agglutination test was positive in 70.6%. In the context of the dissemination report: 63% positive antigenemia, two positive blood cultures, two antigenurias and direct urine tests for cryptococcus were positive, and a skin biopsy performed in one patient was positive. In the induction phase, amphotericin B was prescribed as monotherapy in 87% of cases whereas fluconazole was only prescribed in 7.4% (n = 4)of cases, the combination of both was indicated only in 1.8% and two patients (3.7%) died within 24 hours of diagnosis without receiving antifungal therapy. It is noted that Fluconazole alone at 200 mg / day was initiated at the maintenance phase until the recovery of CD4. The average time after the start of ARVs after beginning the management of the CNM 15 ± 4 days. The result was favorable in 61%, relapse 14.8% and 39% (n = 21) of reported deaths. Conclusion: This study reveals that morbidity and mortality are closely related to the early diagnosis and the initiation of adequate antifungal therapy.
Introduction
Neuromeningeal cryptococcosis (CNM) is a subclinical or chronic cosmopolitan mycosis caused by Cryptococcus neoformans; a levuriform fungus with a tropism for the central nervous system. In patients living with HIV it represents a real problem of diagnosis of the nonspecific part of the clinical manifestations and of the ignorance of the serological status which makes the police wander and retarder. Since 1985, the CNM has remained a major cause of HIV-related mortality. It is estimated each year, nearly 1 million cases worldwide with more than 600 000 deaths. Sub-Saharan Africa pays the annual tax of more than 720,000 cases per year compared with 1 case per million in the United States [1, 2]. The advent of triple antiretroviral therapy and the use of fluconazole for oral candidiasis have significantly reduced this figure although this therapy may reveal latent cryptococcosis or cause relapse [2, 3].
Patients and Methods
This is a retrospective study conducted at the level of the national reference center (CDR) for the treatment of HIV infection: the hospital specialized in infectious diseases El Hadi Flici, service B of Algiers. This study included CNM cases in patients living with HIV (PLHIV) who were identified between January 01, 1993 and July 30, 2017. Patients who presented CNM on a non-HIV site were excluded. The synthesis of the medical files allowed and epidemiological, paraclinical, therapeutic and evolutionary analysis. The diagnosis of CNM is retained by the isolation of cryptococcus in cerebrospinal fluid (CSF) on direct examination after staining with Indian ink, Sabouraud medium culture supplemented with chloramphenicol and the search for antigen cryptococcal capsular soluble by latex agglutination test. For systemic or disseminated extra meningeal forms, antigenemia, blood culture, antigenuria, direct examination of other body fluids, and histopathological examination were performed in a variable manner in our patients.
Results
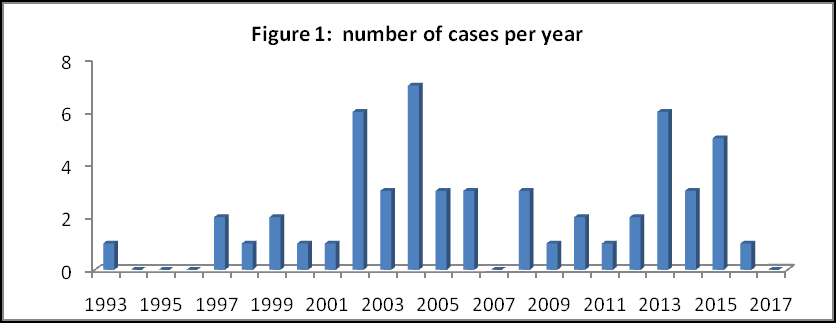
Over a period of 23 years and a half (01 January 1993 - 31 June 2017), 54 cases of CNM were recorded in a cohort of 1289 hospitalized HIV patients, an average frequency of 4.2%. The mean age of our patients is 39 ± 2 years [18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84] with a sex ratio 3.15 (41 men and 13 women). The average prevalence is 3 cases per year. 48 patients were Algerian and 06 foreign (Figure 1).
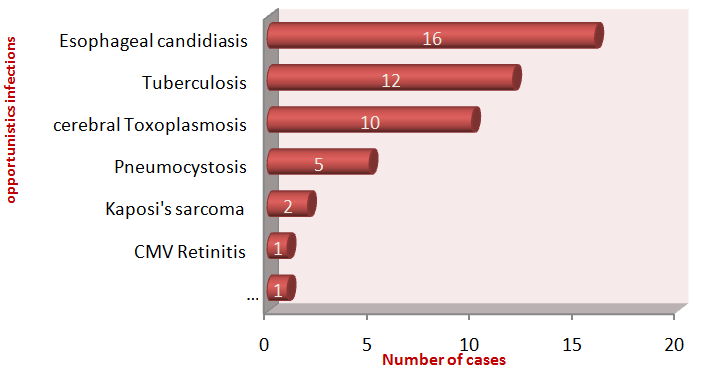
The CNM revealed HIV infection in (n = 22) 41% of cases. It occurred in (n = 13) 24% in patients who have not yet received ARV treatment with recent HIV seropositivity, in (n = 6) 11% in patients lost to clinical escape, (n = 6) 11% in virologic failure and / or immunological and (n = 7) 13% of the MNC was manifested as part of an inflammatory syndrome immune restitution (SRI). At the time of diagnosis; twelve of our patients had co-infection: hepatitis C (n = 6), hepatitis B (n = 1), syphilis (n = 5). Forty-three patients had one or more associated opportunistic infections (OIs): Sixteen cases of oral-esophageal candidiasis. Twelve cases of tuberculosis: five pulmonary, one ganglionic and six with associated lung and lymph node involvement, ten cases of cerebral toxoplasmosis, five cases of pneumocystosis, 02 cases of cutaneous mucosal kaposi, 01 cases of CMV retinitis and 01 cases of visceralleishmaniasis (Figure 2).

![Figure 4: Cutaneous cryptococcosis mentally healing nodule after antifungal treatment. TCD4 lymphocyte typing was done in 33 (61%) patients with an average rate of 30 cells / mm3 [0-222 cells / mm3]. Viral load was performed in 25 (46.3%) patients with a mean 2.15 log10 copies / ml [undetectable - 7.51 log10 copies / ml] (Table 1).](/fulltextimages/1766/fig_4.jpeg)
| CD4 Rates | N | % | ||||||
|---|---|---|---|---|---|---|---|---|
| <50 | 23 | 42 | ||||||
| 50-100 | 2 | 4 | ||||||
| 101-200 | 6 | 11 | ||||||
| >200 | 1 | 2 | ||||||
| No fait | 22 | 41 | ||||||
| Total | 54 | 100 |
Table 1: Table of Variability of CD4 Rates. Out of 51 lumbar punctures performed, the cephalospinal fluid (LCS) was pathological
Table 1: Table of Variability of CD4 Rates. Out of 51 lumbar punctures performed, the cephalospinal fluid (LCS) was pathological in (n = 31) 61%. Of clear appearance in (n = 44) 86%, opalescent (n = 3) 6%, disorder (n = 3) 6% and haematic in (n = 1) 2% of cases. An average cytistachia with 60 elements / mm3 variegated predominantly lymphocytic in 19 (37%) patients [1 - 540 elements / mm3]. Hyper proteinorachie was found in 18 (35%) patients with an average of 0.73 g / l [0.25-1.65g / l]. Hypoglycorachia in 14 (24%) patients with an average of 0.36g / l [0.10-0.89 g / l]. The direct examination with Indian ink staining identifying Cryptococcus neoformans in (n = 31) 61% is of considerable contribution. The search for soluble cryptococcal antigens by the latex agglutination test supports the diagnosis in (n = 36) 70.6% of cases [1/10 - 1/1000000]. The culture on Sabouraud medium supplemented with chloramphenicol is conclusive in (n = 41) 80.3% of the cases (Figures 5 & 6).

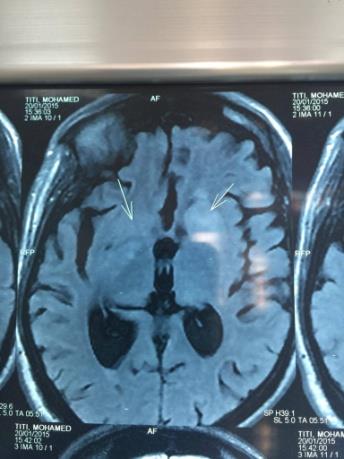
Figure 6: Cryptococcal cultured. As part of the extension assessment, cryptococcal antigenemia is contributive in (n = 34) 63%., two positive blood cultures. Direct urine examination and antigenuria are positive in (n = 2) 3.7%. Cutaneous involvement confirmed after biopsy in a single patient. Brain imaging (CT and / or magnetic resonance imaging) performed in 31 patients showed radiological abnormalities in 21 cases, of which eleven are micro-and macro-nodular hypodense images in the white matter in relation to probable cryptococomas, five in favor of cortico-cortical atrophy, and three are hydrocephalic and two are encephalitis. In 9 patients she returned normal (Figures 7 & 8).
![Figure 8: Hydrocephalus. The average duration of hospitalization is 30 ± 06 days [01 - 120 days]. In the induction phase, amphotericin B is prescribed as monotherapy at a dose of 0.7 mg / kg / d in (n = 47) 87%, fluconazole in (n = 4) 7.4%, the N Age sex SAD ART Opportunistic infection CD4 Tuberculose](/fulltextimages/1766/fig_8.jpeg)
1 41 M 2 mois No
2 36 M 4 mois No Tuberculose ganglionnaire NF Bonne 3 mois 5 mois et ½ Echec I D
3 30 M 3 ans No / NF Mauvaise 6 mois / Inobservance G
4 56 F R No / 222
5 53 M 14 ans AZT/3TC/I4d / NF Mauvaise 5 mois Non précisée Echec I G
6 34 M R No Kaposi cutanéo- combination of both is indicated that in (n = 1) 1.8% and two patients (3.7%) died before the start of treatment, then fluconazole at 400 - 800 mg / d in the consolidation phase and 200 mg / d in the maintenance phase. Seventeen patients had intolerance to amphotericin B, eight of whom had severe anemia, three had pancytopenia and seven had acute renal failure. The average time to start ARVs after the start of CNM treatment is 15 ± 4 days [9 - 56 days]. The evolution is favorable for 33 (61%) patients. (n = 6) 14, 8% relapses. The most common causes are nonobservance of fluconazole prophylaxis (n = 2), immunological failure on ARV treatment (n = 2), SRI and discharge against medical advice. 21 (39%) reported deaths including 47.6% within 2 weeks of diagnosis, either by CNM or another opportunistic infection (Table 2).
Compliance with
1ere 2eme Probable
maintenance E relapse relapse causes
ART
pulmonaire NF Indéterminée 3 mois / Inobservance G Pneumocystose
Sortie contre avis
3 mois / Arrêt de toute thérapeutique D
médical après 05 semaines de trt muqueux 3 Indéterminée 3 mois / SRI G
E: évolution/ M: Masculin/ F: Féminin / NF: Non fait / R: revealed/ Echec. I: Echec immunology/ AZT: zidovudine/ 3TC: Epivir/ I4d: / SRI: syndrome de restauration immune/ G: good/ D: death
| Deaths | Males | Females | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number | 18 | 3 | 21 | ||||||||
| Median age | 39±6 ans [28-84] | 49±3 ans [38-56] | 39±2 ans[18-84] | ||||||||
| Mean CD4 cells/mm3 | 25 [19-164] | 222 [n=2 non fait] | 35 [19-222] | ||||||||
| Viral load log10 copies | 4.9 [4 - >5] | 7 [n=2 non faite] | 5.12 [4- 7] | ||||||||
| Opportunistic infections | |||||||||||
| Tuberculosis | 26.7% (n= 4) | 0% | 19% (n=4) | ||||||||
| Cerebral toxoplasmosis | 33% (n=5) | 33%(n=1) | 28.6% (n=6) | ||||||||
| Pneumocystosis | 6.7% (n=1) | 0% | 5% (n=1) | ||||||||
| Candidosis | 6.7% (n=1) | 0% | 5% (n=1) | ||||||||
| Co-infections |
Table 2: Caracteristic of patients with relapses.
| Hepatitis C | 13% (n=2) | 0% | 9.5% (n=2) |
|---|---|---|---|
| Hepatitis B | 0% | 33%(n=1) | 5% (n=1) |
| Syphilis | 6.6% (n=1) | 0% | 5% (n=1) |
| Cryptococcosis revealing HIV infection | |||
| No | 33% (n=6) | 67%(n=2) | 38% (n=8) |
| Yes | 67% (n=12) | 33%(n=1) | 62% (n=13) |
| ART | |||
| No | 66.7% (n=12) | 33% (n=1) | 62% (n=13) |
| Yes | 16.7% (n=3) | 67% (n=2) | 24% (n=5) |
| Lost to follow- up | 16.6% (n=3) | 0% | 14% (n=3) |
| Symptoms and signs | |||
| Headache | 39% (n=7) | 67% (n=2) | 43% (n=9) |
| Fever | 50% (n=9) | 100% (n=3) | 57% (n=12) |
| Vomiting | 14% (n=3) | 0% | 14% (n=3) |
| Neck stifness | 24% (n=5) | 33% (n=1) | 28.5% (n=6) |
| Neurological signs | 47.6% (n=10) | 100% (n=3) | 62% (n=13) |
| Laboratory characteristics | |||
| CSF | |||
| No abnormalities | 39 %(n=7) | 67 %(n=2) | 43% (n=9) |
| India ink positive | 67% (n=12) | 67% (n=2) | 67% (n=14) |
| Culture positive | 100% (n=18) | 100% (n=3) | 100% (n=21) |
| cryptococcal antigen | 78% (n=14) | 67% (n=2) | 76% (n=16) |
| positive | |||
| Positive blood culture | 6.6% (n=1) | 0% | 5% (n=1) |
| Positive antigenaemia | 50% (n=9) | 67% (n=2) | 52% (n=11) |
| Positive antigenuria | 6.6%(n= 1) | 0% | 5% (n=1) |
| Antifungal Treatment | |||
| Amphotericin B | 89% (n=16) | 100% (n=3) | 90.5% (n=19) |
| Ampho B + fluco | 0% | 0% | 0% |
| Fluconazole | 0% | 0% | 0% |
| No | 13% (n=2) | 0% | 9.5% (n=2) |
| Median survival time | |||
| > 3 months | 5,5% (n= 1) | 33% (n= 1) | 4,7% (n= 2) |
| < 3 months | 94% (n= 17) | 67% (n= 2) | 90,4% (n= 19) |
| Median | 12±3 jours | 26± 6 jours | 15±4 jours |
| < 2 weeks | 55,5% (n= 10) | 0% | 47,6% ( n= 10) |
Table 3: Caracteristic of patients with relapses.
ART: antiretroviral treatment CSF: cerebro-spinal fluid. Table 2: Caracteristic of patients with relapses.
Discussion
Our study showed that the number of cases of CNM has increased significantly for two decades with resurgence in the last six years CRD Algiers in connection with the increase in the number of PLWHA followed in our institution. The average frequency is 4.2%, this result is higher than reported in Tunisia 3.47%, Morocco 1.4%, India 1.32% and Cote d'Ivoire 0.6% and lower than that of the Central African Republic 6.5% [4, 5, 6, 7, 8]. The mean age in our patients is 39 ± 2 years [18-84years] and the sex ratio 3.15 (41 males and 13 females) are consistent with what was reported in previous studies or the young age testifying to an active sex life and the masculine gender predominate because men by their work and their activities outside are more exposed to the germ [4, 9]. 76% of our patients are diagnosed at the AIDS stage (the CNM is revealing in 41%, occurring in 24% after a recent HIV seropositivity and in 11% in patients lost to follow-up) like the majority of African patients confirming the problem of HIV testing and care in Algeria, despite awareness-raising campaigns and the free provision of ARVs since 1998 [8, 10]. In our series, the average delay between the onset of clinical signs and hospitalization of 34 ± 8 days is distinctly greater than reported in the literature or is 10 to 15 days on average [5, 6, 11]. In more than one third of the cases the CNM occurred in patients whose seropositivity is unknown, the bacterial origin is then mentioned in the first place and it is only in the absence of clinical improvement under antibiotic treatment that a fungal etiology is sought. Half of our patients presented with meningoencephalitis as well as with Dromer et al., unlike Antinori et al. where more than 70% of patients had signs of meningitis [9, 12]. The progressive onset marked by isolated or febrile headaches (n = 20) in our series are often trivialized by the patient and the physician, hence the delayed diagnosis [4, 13, 14, 15]. Frankish meningeal syndrome is rarely complete with a stiff neck stiffness observed only in 26% of cases in our series against 85.9% in Gbangba-Ngai, et al. [8]. The disseminated form is found only in 4 (7.4%) patients, the cutaneous involvement which is the second metastatic site after the central nervous system is observed in 5% - 10% of cases, rarely primitive representing only 0.5% of cryptococcal infections, most often in immunocompetent [16, 17, 18, 19]. However, it is found in only two (3.7%) of our patients taking the appearance of a necrotic center-aligned umbilical nodule corresponding to what is described in the literature even if the appearance of molluscum contagiosum is the more observed [19, 20]. The average CD4 cell count at 30 cells / mm3 is indicative of profound immunodepression at the time of diagnosis [4, 13]. However, in our study, one patient presented a CNM with a CD4 count greater than 200 cells / mm3, the same finding is reported in other studies where CNM is observed at a moderate immunodepression stage [7, 9, 13, 21]. The normal LCS in 39% of the cases is at the origin of the diagnostic wandering [14]. It is mostly clear what is classical with low lymphocyte predominance in only 37% of cases [6]. Atypical LCS with cytological discordance noted in our series are reported in some studies [7, 15]. Hypoglycorachia is only found in 24% with an average of 0.36g / l, this rate is lower than that of kilani et al and Aoussi et al. and hyperproteinorachie in 35% with an average of 0.73 g / l is inferior to that of Kilani, et al. [4, 13]. Direct examination with Indian ink staining identifies Cryptococcus neoformans in 61% which is consistent with the literature or is positive in 50 - 87% [29, 30] and the search for cryptococcal antigen is positive in 70.6%, its positivity can precede by several months the direct examination, which allowed to support the diagnosis when the latter was negative [26, 28] the culture is conclusive in 80,3%, this result is inferior to those reported in the literature [4, 5, 22, 23, 24, 25]. Two prostatic lesions confirmed by the direct examination of urine and antigenuria whose negativation must be verified after the start of antifungal treatment because the prostate is considered a reservoir of cryptococcus and source of relapse [7]. In our series, only one skin biopsy made positive. The exploration of visceral involvement in disseminated forms is very limited in Algeria either by the weakness of the technical platform or the discrimination of the medical profession vis-à-vis PLHIV by dramatizing the risks of contagiousness. The measurement of intracranial pressure was not performed in our patients despite its high prognostic value due to lack of necessary device at our facility. In our study, brain imaging is normal in 29% of what is commonly described and the observed abnormalities are frequently attributed to HIV-associated infections [26, 27]. Micro and nodule images of the white matter, cortico- subcortical atrophy and the signs of hydrocephalus observed are considered suggestive but not specific to CNM [28]. An average hospital stay of 30 ± 06 days, almost similar to that of African studies; justified by the delay of sterilization of the LCS, the seriousness of the contemporary IOs of the CNM and the difficulty of the management of the secondary effects related to the therapeutics [13, 14, 29]. The treatment is based on amphotericin B or fluconazole for at least 2 weeks, relayed by fluconazole 800-400 mg / day for 8 to 10 weeks according to the adopted Algerian consensus [30]. In the absence of 5- fluorocytosine because of its high cost, amphotericin B is used as monotherapy in 87% of patients with a good evolution in 61% of cases contrary to what is observed in Brouwer, et al. [31]. However, it is responsible for side effects and not least with acute renal failure, severe anemia and pancytopenia determining the need for supply by liposomal amphotericin B. Six patients had relapses within 3-6 months of the first episode. As a cause, prophylactic fluconazole was discontinued in three cases, immunological failure due to non-compliance with ARV treatment in two cases and SRI in one case; these results corroborate the need for routine prophylactic treatment with fluconazole until a clear and stable immune recovery> 100-200 CD4 has been achieved by ARVs for 6 months [32, 33]. Should be ensured by good counseling for PLHIV. 39% of patients experienced a fatal outcome. This mortality rate is very much lower than that of African series, or 83.3% in Tunisia, 60% in Morocco, 42.6% in Burkina Faso and South America, with 51.8% in Africa [4, 5]. Brazil but close to a European series with 31% of deaths in Portugal [34, 35]. The mean ARV initiation delay after the start of antifungal therapy was 15 ± 4 days longer than that of Kambugu, et al. 35 ± 13 days [36]. Our study allowed us to shed light on this fungal infection that remains widespread in Algeria due to the increase in the number of patients followed for HIV infection and to know its epidemiological, clinical, paraclinical, therapeutic and progressive characteristics. . But it is limited by its retrospective aspect, the absence of computerized and complete data in the medical files and the restricted nature of the studied cohort established in a single department of the hospital which must be widened to the whole national territory for the purpose of to evaluate the incidence of the CNM among PLWHA in Algeria and to cope with this scourge which has a significant [37, 38].
Conclusion
Our study showed that neuromeningeal cryptococcosis is a topical fungal infection in our country revealing HIV infection in 42% of cases. Early diagnosis and proper care with respect for the prophylaxis fluconasole improves infection prognosis and reduced mortality.
References
-
Park BJ, Wannemuehler KA, Marston BJ, Govender N, Pappas PG, et al. (2009) Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS 23(4): 525-530.
-
Mirza SA, Phelan M, Rimland D, Graviss E, Hamill R, et al. The changing epidemiology of cryptococcosis: an update from population-based active surveillance in 2 large metropolitan areas, 1992-2000. Clin Infect Dis 36(6): 789-794.
-
Bicanic T, Harrison TS (2005) Cryptococcal meningitis. Br Med Bull 18(72): 99-118.
-
Kilani B, Ammari L, Marrakchi C, Tiouiri H, Kanoun F, et al. (2005) Étude rétrospective des cas de cryptococcose neuromé- ningée chez des patients atteints de sida { l’hôpital La Rabta { Tunis. Journal de Mycologie Médicale 15(2): 114-115.
-
Dollo I, Marih L, Fane MEl, Es-sebbani M, Sodqi M, et al. (2016) Étude rétrospective de la cryptococcose neuroméningée chez les patients infectés par le VIH dans le service des maladies infectieuses du CHU de Casablanca, Maroc. Journal de Mycologie Médicale 26(4): 331-336.
-
Ravinder KS, Shivani R, Aman S, Ajay W, Arunaloke C, et al. (2012) A Retrospective Study of AIDS- Associated Cryptomeningitis. Aids Research and Human Retroviruses 28(10): 1220-1226.
-
Kadjo K, Ouattara B, Adoubryn KD, Kra O, Niamkey EK. Aspects actuels de la cryptococcose neuroméningée chez des sujets adultes infectés par le VIH dans le service de médecine interne du CHU de Treichville d’Abidjan. J Mycol Med 21(1): 6-9.
-
Gbangba-Ngai E, Fikouma V, Mossors-Kpinde CD, Tekpa G, Ouavene JO, et al. (2014) La cryptococcose neuroméningée au cours de l’infection { VIH { Bangui, { l’ère du traitement antiretroviral. Bull Soc Path Exot 107(2): 106-109.
-
Antinori S, Ridolfo AL, Fasan M, Magni C, Galimberti L, et al. (2009) AIDS-associated cryptococcosis: a comparison of epidemiology, clinical features and outcome in the pre- and post-HAART eras Experience of a single centre in Italy. HIV Medicine 10(1): 6-11.
-
Kerbal H, Ouzriat B (2015) L'épidémiologie du VIH/SIDA en Algérie. L’Institut Pasteur d'Alger (LNR/_IPA_).
-
Gomerep SS, Idoko JA, Ladep NG, Ugoya SO, Obaseki D, et al. (2010) Frequency of cryptococcal meningitis in HIV-1 infected patients in north central Nigeria. Niger J Med 19(4): 395-399.
-
Dromer F, Mathoulin-Pélissier S, Launay O, Lortholary O, French Cryptococcosis Study Group (2007) Determinants of disease presentation and outcome during cryptococcosis: the CryptoA/D study. PLoS Med 4(2): 297-308.
-
Aoussi EF, Ehui E, Dembélé JP, Kolia-Diafouka P, Elloh NF, et al. (2012) Cryptoccocal meningitis and HIV in the era of HAART in Côte d’Ivoire. Med Mal Infect 42(8): 349-54.
-
Minta DK, Dolo A, Dembele M, Kaya AS, Sidibe AT, et al. (2011) La cryptococcose neuro-méningée au Mali. Med Trop 71(6): 5891-6595.
-
Ouattara B, Eholie SP, Adoubryn KD, Kra O, Tia H, et al. (2007) Retrospective study of bacterial and cryptococcal meningitis occurring in HIV adult patients in Abidjan (Ivory Coast). J Mycol Med 17: 82- 86.
-
M El Fane, L Badaouil, Ouladlahsen A, Sodqi M, L Marih, et al. (2015) La cryptococcose au cours de l’infection { VIH Cryptococcosis during HIV infection. Journal de mycologie médicale 25(4): 249-322.
-
Christianson JC, Engber W, Andes D (2003) Primary cutaneous cryptococcosis in immunocompetent and immunocompromised hosts. Med Mycol 41(3): 177- 188.
-
Goonetilleke AKE, Krause K, Slater DN, Dev D, Wood ML, et al. (1995) Primary cutaneous cryptococcosis in an immunocompromized pigeon keeper. Br J Dermatol 133(4): 650- 652.
-
Datsis AC, Tsintoni A, Tasoula A, Roupas N, Trahalios H, et al. (2009) Isolated cutaneous cryptococcosis in an immunocompromised patient cured without antifungals. Int J Dermatol 48(4): 440-441.
-
Faith M Durden, Boni Elewski (1994) Cutaneous involvement with Cryptococcus neoformans in AIDS. J Am Acad Dermatol 30(5): 844-848.
-
Soumare M, Seydi M, Ndour CT, Dieng Y, Diouf AM, et al. (2005) Aspects actuels de la cryptococcose neuro- méningée à Dakar. Med Trop 65: 559-562.
-
Sato Y, Osabe S, Kuno H, Kaji M, KüIzumI (1999) Rapid diagnosis of cryptococcal meningitis by microscopic examination of centrifuged cerebrospinal fluid sediment. J Neurol Sei 164(1): 72-75.
-
Darras Joly C, Chevret S, Wolff M, Longuet P, Casalino E, et al. (1996) Cryptococcosis neoformans infection in France: Epidemiologie features of and early prognostic parameters for 76 patients who were infected with human immunodeficiency virus. Clin Infect Dis 23(2): 369-376.
-
Marukutira T, Huprikar S, Azie N, Quan SP, Meier- Kriesche HU, et al. (2014) Clinical characteristics and outcomes in 303 HIV-infected patients with invasive fungal infections: data from the Prospective Antifungal Therapy Alliance registry, a multicenter, observational study. HIV AIDS (Auckl) 6: 39-47.
-
Karaouzen M, Khaldi S (2007) Etude biologique rétrospective des meningites à Cryptococcus neoformans chez l’immunodéprimé. Archives de L’Institut Pasteur d'Alger (_IPA_)
-
Powderly G William (1993) Cryptococcal Meningitis and AIDS. Clinical Infectious Diseases 17(5): 837-842.
-
Revest M, Decaux O, Frouget T, Gazalets C, Albert TD (2006) Cryptococcal infection in non-HIV patients. Study on four cases and review of literature Rev Med Int 27: 2003-2008.
-
Lortholarya O, Fontanetb A, Memain N (2005) Incidence and risk factors of immune reconstitution inflammatory syndrome complicating HIV-associated cryptococcosis in France. AIDS 19(10): 1043-1049.
-
Bamba S, Barro-Traoré F, Sawadogo E, Millogo A, Guigerndé RT (2012) etude rétrospective des cas de cryptococcose neuromeningée au centre hospitalier universitaire de Bobo Dioulasso depuis l’accécébilité au antirétroviraux au burkina Faso. J Mycol Med 22: 30-34.
-
Guide de la prise en charge de l’infection { VIH en Algérie (2010).
-
Brouwer EA, Rajanuwong A, Chierakul W, Griffin GE, Larsen RA, et al. (2004) Combination antifungal therapies for HIV associated cryptococcal meningitis: a randomised trial. Lancet. 363(9423): 1764-1767.
-
Jarvis JN, Meintjes G, Williams Z, Rebe K, Harrison TS (2010) Symptomatic relapse of HIV-associated cryptococcal meningitis in South Africa: The role of inadequate secondary prophylaxis. S Afr Med J 100(6): 378-382.
-
World Health Organization (2011) Rapid advice: prevention, diagnosis and management of cryptococcal meningitis in HIV-infected adults, adolescent and children. _34._ Beatriz Consuelo Quinet Leimann, Rosalina Jorge Koifman (2008) Cryptococcal meningitis in Rio de Janeiro State, Brazil, 1994-2004. Cad Saúde Pública 24(11): 58-62.
-
João Figueira-Coelhoa, Teresa Martinsb, João Machadob, Fernando Maltez (2010) Cryptococcosis in HIV-infected patients: A report of 84 cases (1985– 2008)”. European J Internal Med 21(3): e16.
-
Kambugu A, Meya DB, Rhein J, O'Brien M, Janoff EN, et al. (2008) Outcomes of cryptococcal meningitis in Uganda before and after the availability of highly active antiretroviral therapy. Clin Infect Dis 46(11): 1694-1701.
-
JM Mbuagbaw, Biholong, AK Njamnshi (2006) La Cryptococcose Neuro-Méningée et l'infection au VIH dans le service de medecine du centre hospitalier et universitaire de Yaounde, Cameroun. African J Neurological sci 25 (2): 13-20.
-
Murakawa GJ, Kerschmann R, Berger T (1996) Cutaneous Cryptococcus infection and AIDS. Report of 12 cases and review of the literature. Arch Dermatol 132(5): 545-548.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey