Obstructive Jaundice with Acute Pancreatitis Following Elective Laparoscopic Cholecystectomy in Immediate Postoperative Period-A Rare Presentation
Laparoscopic cholecystectomy (LC) is one of the most common surgical procedures performed worldwide. The spectrum of complications post LC may differ from those that occur after open surgery. Retained CBD stones and bile duct injuries are the most common causes of early post LC jaundice. Transient obstructive jaundice post LC is almost always due to spontaneous passage of retained CBD stones or sludge. Post cholecystectomy pancreatitis is a rare entity. We report a case of coincident obstructive jaundice and acute pancreatitis following elective LC.
Introduction
Cholecystectomy is one of the most common surgical procedures performed worldwide. Laparoscopic cholecystectomy (LC) has emerged as the gold standard for management of gallstone disease and accounts for 86% of all the cholecystectomies. National Institute of Health (NIH) in 1992 endorsed LC for almost all patients with symptomatic gallstones keeping with its safety and proven efficacy [1]. It has evolved from a relative contraindication in the 90s to the preferred surgical management of acute cholecystitis in the SAGES guidelines [2].
While it offers the benefits of a minimally invasive procedure, the gamut of complications in laparoscopic approach differ considerably from that of open surgery [3]. LC related complications like bile duct injury (BDI) are more common in incidence, proximal in location and are often associated with concomitant vascular injury compared to open procedure.
Obstructive jaundice following LC is an extremely worrisome complication and may require an invasive intervention, either immediate or delayed [4]. Post- cholecystectomy jaundice has traditionally been attributed to missed CBD stones, bile duct injuries, biliary strictures or medical causes of jaundice.Retained CBD stones and unrecognized BDIs are among the most common causes of early post cholecystectomy jaundice.Rarely, obstruction may be due to an obscure, self-limited inflammation of the bile duct [4, 5].
Stones in cystic duct can spill into the CBD and cause pancreatitis following cholecystectomy [6]. Ramirez et al. in a retrospective study of more than 4000 elective LC showed postoperative pancreatitis is a relatively rare complication and has an incidence of 0.1%. Z’graggen, et al. reported acute pancreatitis after a completed LC in 0.34% cases, of which biliary origin was established in 12%, most often due to retained CBD stones [7].
We report a rare case of coincident obstructive jaundice and acute postoperative pancreatitis following elective laparoscopic cholecystectomy [8].
Case Report
A 65 year old female underwent elective LC for chronic calculus cholecystitis. Prior to the procedure, biochemical tests and imaging were done. Liver function tests were within normal limits. Serum amylase and lipase were 58 U/L and 35 U/L respectively. USG Abdomen showed contracted gallbladder with WES sign and multiple hyperechoic foci casting posterior acoustic shadow with a normal calibre CBD.
Intra-operatively, omentum was adhered to the gallbladder and hepatocystic triangle. Gallbladder was distended, inflamed and edematous causing intraoperative hemorrhage, which justified placement of a subhepatic tube drain.
Drain output was 40mL and 10mL, serous in nature on the first and second postoperative days respectively and drain was removed on POD2. On POD3, patient complained of pain abdomen, constipation and developed icterus. Liver function tests showed a total bilirubin of 7.2 mg/dL with direct fraction of 4.9 mg/dL. Liver enzymes were SGOT- 384 U/L, SGPT- 341 U/L, ALP- 2680 U/L and GGT- 711 U/L. Serum amylase and lipase were 378 and 161 U/L respectively (Table 1).
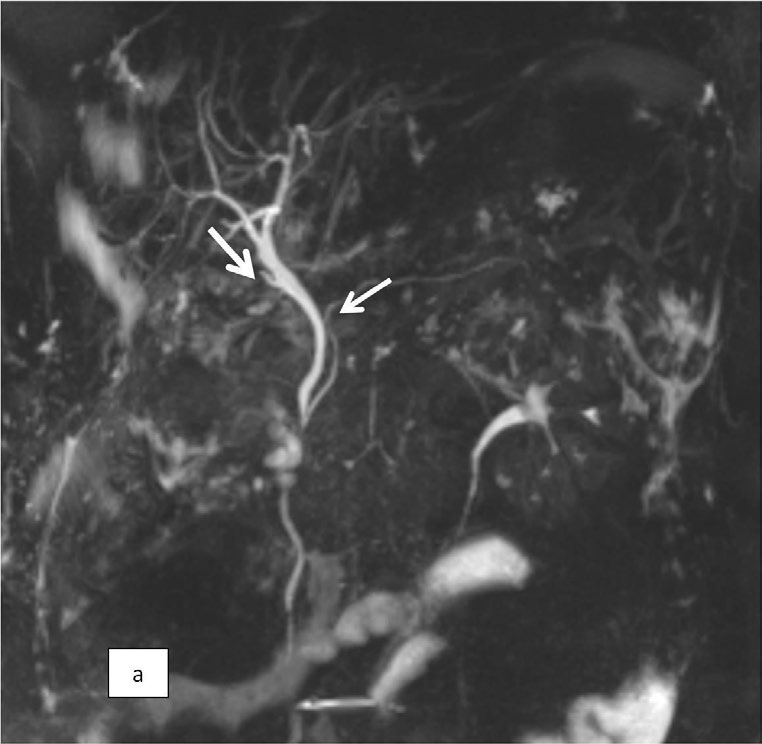
USG Abdomen was done and bilioma, CBD or intrahepatic biliary radicle dilatation was ruled out. MRCP was done which revealed a normal calibre CBD and MPD without any intra-luminal filling defects (Figure 1). CBD diameter was measured as 6.4mm.
Diagnosis of obstructive jaundice with mild acute pancreatitis was made and patient was managed conservatively. Patient improved symptomatically and liver function tests, amylase and lipase levels also normalised over the next few days (Table 1) and patient was discharged satisfactorily on POD8.
| Pre-op | POD3 | POD5 | POD7 | |
|---|---|---|---|---|
| Total Bilirubin (mg/dL) | 0.42 | 7.22 | 2.13 | 1.29 |
| Direct Bilirubin (mg/dL) | 0.21 | 4.9 | 1.28 | 0.72 |
| SGOT (U/L) | 21.5 | 384 | 132.7 | 148.6 |
| SGPT (U/L) | 23.8 | 341 | 249.2 | 62 |
| ALP (U/L) | 200.2 | 2680 | 1325 | 959.2 |
| GGT (U/L) | 24.3 | 711 | 712 | 238.7 |
| Serum Amylase (U/L) | 57.7 | 378.1 | - | 72.1 |
| Serum Lipase (U/L) | 34.5 | 161.4 | - | 68 |
Table 1: Preop LFT and its comparison with day wise post op values.
Discussion
LC has an uneventful postoperative course in most cases. Common early post LC complications are bile leak and iatrogenic BDI with an incidence of 1.1-4.0% and 0.3-0.5% respectively.Retained CBD stones have an incidence between 0.5-3.4% following LC, of which many pass spontaneously within 6 weeks [9].
In a retrospective study of more than 1400 elective LC, the prevalence of clinically significant retained CBD stones was estimated as 1.84% and time of presentation post LC ranged from 2 months to 2 years [10, 11]. Cox et al. reported the median time of presentation as 4 years with a range of 6 days to 18 years post LC [12]. However, these studies included only those patients who required ERCP clearance for retained CBD stonesv [13]. As many retained stones would have passed spontaneously, the true prevalence could be much higher.
The most common presentation of retained CBD stones is abdominal pain with or without deranged LFT. Rarely retained common duct stones present with more serious complications of obstructive jaundice or cholangitis. Jaundice due to retained CBD stones has been reported in 31% cases in a retrospective study.However we could not find studies comparing the size of gallstone as a predictor of CBD retention post-cholecystectomy [13].
In the era of LC and ERCP, management of CBD stones has become increasingly complex. Suspicion of CBD stone preoperatively is essential as it has significant implications on further management. ASGE classified patients into low risk (<10%), intermediate risk (10-50%) and high risk (>50%) for CBD stones based on the age, liver function tests, CBD diameter and presence of CBD stones on USG.
Our patient was a low risk for CBD stones as per ASGE criteria and thus preoperative MRCP or IOC was not included in the standard of care [14]. Per-op findings also did not raise any suspicion of CBD stones. Risk of retained CBD stones in low risk patients varies between 0.2-2.3%.However, patient developed obstructive jaundice with mild acute pancreatitis in the immediate postoperative period [15]. Post cholecystectomy pancreatitis is an uncommon complication in patients without CBD stones on preoperative evaluation and coincident obstructive jaundice and acute pancreatitis following LC is unreported.
As USG and MRCP ruled out bile leak, CBD stones or BDI and patient’s symptoms and liver functions improved over subsequent days, we postulate a transient obstruction of the common biliopancreatic channel due to retained CBD stones, sludge ball or rarely hemobilia as the cause of obstructive jaundice and acute pancreatitis. Since no obstruction was evident on MRCP and in view of clinical and biochemical improvement, endoscopic intervention was not warranted in this case.
Learning points
- Spontaneous passage of retained CBD stones, sludge or hemobilia can lead to obstructive jaundice post LC and must be differentiated from more worrisome causes such as BDI.
- Post cholecystectomy acute pancreatitis is a rare entity.
- Endoscopic intervention is mandatory in situations where obstruction is evident on MRCP and patient remains symptomatic.
Acknowledgements: Department of Radiodiagnosis and Imaging, AIIMS Rishikesh for MRCP images.
References
-
Borzellino G, Sauerland S, Minicozzi AM, Verlato G, Di Pi- etrantonj C, et al. (2008) Laparoscopic cholecystectomy for severe acute cholecystitis. A meta-analysis of results. Surg Endosc 22: 8-15.
-
NIH consensus conference (1993) Gallstones and laparoscopic cholecystectomy. JAMA 269:1018-1024.
-
The role of Laparoscopic Cholecystectomy- guidelines for clinical application (1993) Society of American Gastrointestinal Endoscopic Surgeons (SAGES). Surg Endosc 7: 369-370.
-
Strasberg SM, Helton WS (2011) An analytical review of vasculobiliary injury in laparoscopic and open cholecystectomy. HPB 13(1): 1-14.
-
Mohammad MS, Yasser HH, Abdou IZ (2019) Management of Postcholecystectomy Obstructive Jaundice. The Egyptian Journal of Hospital Medicine 74(7): 1566-1576.
-
Mansour AY, Stabile BE (2000) Extrahepatic biliary obstruction due to post-laparoscopic cholecystectomy biloma. JSLS 4(2): 167-171.
-
Ramirez JR, Raj P (2010) Acute pancreatitis after elective laparoscopic cholecystectomy: Retrospective study. Presented at the Scientific Session of the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) National Harbor, pp: 14-17.
-
Z’graggen K, Aronsky D, Maurer CA, Klaiber C, Baer HU (1997) Acute postoperative pancreatitis after laparoscopic cholecystectomy. Results of the Prospective Swiss Association of Laparoscopic and Thoracoscopic Surgery Study. Arch Surg 132(9): 1026-1030.
-
Adamsen S, Hansen OH, Funch-Jensen P, Schulze S, Stage JG, et al. (1997) Bile duct injury during laparoscopic cholecystectomy: a prospective nationwide series. J Am Coll Surg 184(6): 571-578.
-
Sanjay P, Weerakoon R, Shaikh IA, Bird T, Paily A, et al. (2011) A 5-year analysis of readmissions following elective laparoscopic cholecystectomy - cohort study. Int J Surg 9(1): 52-54.
-
Anwar S, Rahim R,Agwunobi A, Bancewicz J (2004) The role of ERCP in management of retained bile duct stones after laparoscopic cholecystectomy. NZ Med J 117(1203): U1102.
-
Lee DH, Ahn YJ, Lee HW, Chung JK, Jung IM (2016) Prevalence and characteristics of clinically significant retained common bile duct stones after laparoscopic cholecystectomy for symptomatic cholelithiasis. AnnSurg Treat Res 91(5): 239-246.
-
Cox MR, Budge JP, Eslick GD (2015) Timing and nature of presentation of unsuspected retained common bile duct stones after laparoscopic cholecystectomy: a retrospective study. Surg Endosc 29(7): 2033-2038.
-
Maple JT, Ben-Menachem T, Anderson MA, Appalaneni V, Banerjee S, et al. (2010) The role of endoscopy in the evaluation of suspected choledocholithiasis. Gastrointestinal endoscopy 71(1): 1-9.
-
He H, Tan C, Wu J, Dai N, Hu W, et al. (2017) Accuracy of ASGE high-risk criteria in evaluation of patients with suspected common bile duct stones. Gastrointest Endosc 86(3): 525-532.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey