The Modified Two-By-Two Fixed Orthodontic Appliance for Anterior Cross Bite in Primary Dentition: A Case Report
Background: Anterior teeth are the mirror of facial appearance plays a vital role in developing facial beauty, self-confidence, attractive personality even in growing child. 1.6 to7.9 % out of 27 % is the total prevalence rate of anterior cross bite. Various treatment modalities and options have been incorporated, but the major draw is treatment time consumption and patient compliance. To date modified continuous arch wires are used to correct cross-bites. Case presentation: A 4 years girl presented with Class I canine relation and mesial step occlusion transplant relation with anterior cross bite, concave face. Treatment involved placement of blue bite turbo's on lower deciduous second molars and two by two fixed orthodontic continuous arch wire in maxillary teeth. Conclusion: The design of this modified 2 by 2 appliance allows buccal tipping of anterior teeth, it provides light and continuous force for physiological orthodontic movement with minimal root resorption; the treatment of anterior cross bite is corrected in 12 days.
Introduction
Anterior teeth are the mirror of facial appearance plays a vital role in developing facial beauty, self-confidence, attractive personality even in growing child; any abnormality in positioning of anterior teeth can disturb developing normalcy of oro-facial growth and development [1, 2]. Most often anterior cross-bite is seen in primary and mixed dentition period [1, 2]. Graber has defined cross-bite as a condition where one or more teeth may be abnormally malposed either lingually or labially with reference to opposing teeth [3].
Ferguson et al reported that 1.6 to 7.9 % is the prevalence rate of anterior cross bite caused due to various factors as skeletal, dental and functional. Skeletal anterior cross-bite can be genetic, hereditary or discrepancy in maxilla and mandibular length. Dental anterior cross bite associated with localized tipping of teeth with normal jaw relationship. Functional anterior cross-bite is due to premature occlusal contact with opposing jaw and deviate mandible [3].
The potential adverse effects of anterior cross-bite are concave facial appearance, enamel wear, gingival recession, thinning of alveolar bone, mobility, jaw deviation and temporomandibular pain dysfunction [3, 4]. Thus early correction of such malocclusion in primary dentition phase can prevent potential associated adverse effects and facilitates normal cranio-facial growth. However, previous case reports have reported that 50% of anterior cross-bite is self-correcting anomaly, and do not get significant benefits from earlier intervention [4]. But, most of the case series and studies have reported that in patients with the self-corrected anterior cross-bite maintains the skeletal abnormalities resulting in craniofacial asymmetry, Undesirable esthetics, condylar deviation & TMJ sounds, Loss of arch integrity, and Abnormal speech patterns [3, 4].
The rationale for early treatment, prevention is better than cure, and it provides an ideal platform to use various removable and fixed appliances; a privileged pace of success especially in young patients without skeletal discrepancy. The removable appliances as Catlan’s appliance, removable appliances with z-spring(s), expansion screw, and tongue blade can be used to correct anterior cross bite. Fixed appliances as quadhelix with extended anterior arms, fixed brackets, reverse crown, fixed composite resin. The major disadvantage is prolonged treatment period, patient compliance issue, tedious lab work, and frequent patient appointments [1, 2, 3].
This article aimed to present a case report of successful correction of anterior cross bite using modified 2 X4 appliance as a 2 X 2 fixed orthodontic appliances with rubber sleeve, blue bite turbo on deciduous second molars. The merits of this technique are acceptable patient compliance can achieve faster results and provides an alternative treatment modality to correct anterior cross bite.
Case Report, History and Clinical Examination
A good obliging 4-year-old girl was referred to orthodontic clinic for treatment of anterior cross bite. The general appearance and examination of the head and neck were unremarkable. Intraoral examination revealed a primary dentition with anterior crossbites. The occlusal relationship of the primary molars was a mesial step; primary canines established a Class I relationship and 2mm of reverse over jet 4mm of deep bite. Generalized spacing or primate space was present. On extra oral examination facial profile was straight, horizontal growth, deep mentolabial sulcus, and competent lips with reduced lower third of facial heights. The intra-oral examination oral facial appearance is illustrated in figure 1. The Lateral cephalometric analysis data is illustrated in table 1, and revealed a , SNA 78.50, SNB 790.ANB -.5, Li-NA 27/5mm, Li-NB 23/6.5 mm. Upper lip -2 mm, and lower lip 4 mm.
| Parameter | Pre treatment | Post -treatment | |
|---|---|---|---|
| 1 | SNA | 78.5° | 79 |
| 2 | SNB | 79 | 79 |
| 3 | ANB | 0.5 | 0 |
| 4 | CONVEXITY | -1.5 | 0 |
| 5 | FACIAL ANGLE | 85° | 86° |
| 6 | Y-ANGLE | 62 | 62 |
| 7 | GO-Gn-SN | 35 | 37 |
| 8 | OCC-SN | 18 | 16 |
| 9 | Pog-Nb | 1mm | 2mm |
| 10 | Li-NA | 27/5mm | 29/6mm |
| 11 | Li-NB | 23/6.5mm | 21/6.5mm |
| 12 | I-I | 122 | 123 |
| 13 | Wit's | 3mm | 2mm |
| 14 | Soft tissue Upper lip Lower lip | -2mm 3mm | 0mm 3mm |
Table 1: Pre and Post Cephalometric Analysis at 4years.

Treatment Objectives
The primary treatment objective is to correct the anterior cross bite and reverse over jet.
Treatment Alternatives
Different treatment modalities and various treatment options are given in table 2.
| S.No | Treatment options | |
|---|---|---|
| Primary dentition phase | Mixed dentition phase | |
| 1 | Tongue blades | Reversed stainless steel crowns, |
| 2 | Fixed acrylic planes | Expanders |
| 3 | Catalan’s appliance | Fixed composite resins |
| 4 | Removable appliance with z- spring | Inclined preformed crowns, w- spring, fixed wire |
Table 2: Different treatment modalities and various treatment options.
Case Strap Up
After subsequent clinical examinations and cephalometric analysis, the decision was made to treat with 2X2 fixed appliance. Treatment protocol was explained to parents and written informed consent was taken. The labial surface of the upper incisors and primary second molars were polished with rubber cups using pre formed polishing paste (prime dent pumice-polish paste, India) and teeth were cleaned with water using three way syringe. The teeth were etched with 37% phosphoric acid (Etch- 37 with BAC, Bisco, USA) for 15 seconds rinsed and dried. An adhesive system (Enlight ortho bond Ormco USA) was applied and cured for 3 seconds using a high intensity light unit (Woodpecker, Guilin medical instrument Co,Ltd, China ) Composite resin (Enlight, Ormco USA) was used to bond MBT TM 022 X028 slot bracket and convertible molar tubes. Bonding of incisor bracket and molar tube was bonded at same distance such that wire slots lay is same line. On lower second primary molars turbo’s were placed using blue bite composite and anterior bite 2mm of bite opening was made. Detail Illustration is given in figure 1.
Treatment Progress
A preformed 016 Niti arch wire was placed to check the slot levels; 2X2 appliance was fabricated using .016” AJ Wilcock premium plus wire. The figure 1 shows 2X2 appliance with sleeves.
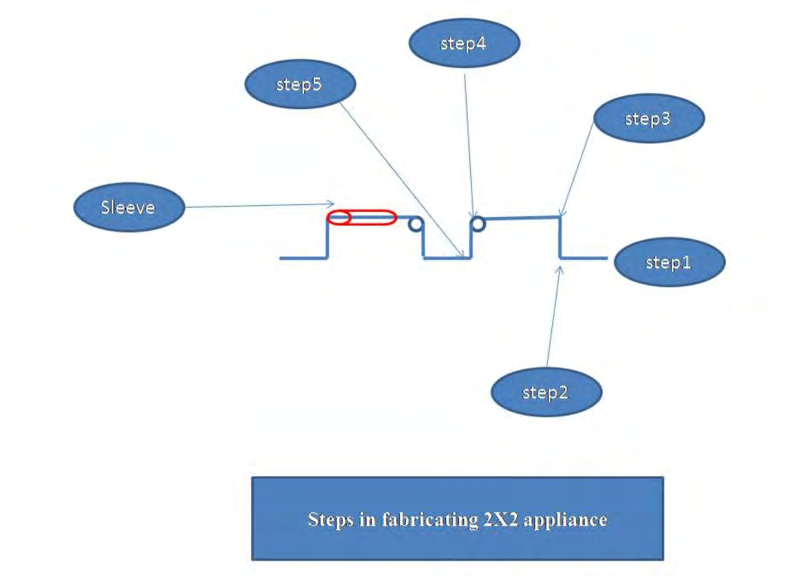
Construction of 2X2 arch wire (figure 3) [5]
The 2X2 appliance is continuous arch wire extends across both buccal segments covering only four teeth .i.e. two central incisor and two primary second molars. Figure number 3 is illustrating detail steps of 2x2 appliance fabrication. Steps in fabrications of appliances Step 1:- On study models using 016” AJ Wilcock premium plus wire U – shape arch was made Step 2:- 3mm away from mesial side/ entry of molar tube a marking was made on arch wire Step 3:- From the markings a perpendicular bend was given 5mm towards sulcus and Maintaining 5 mm height wire was extended toward anterior till deciduous lateral incisor. Step 4:- 3mm internal diameter helix was incorporated at junction between mesial to lateral Incisor and from helix a 5mm perpendicular bend was given towards incisor edge. Step 5:- At the incisor bracket slot perpendicular wire was bend parallel to occlusal plane and Passes toward other side of arch passively from incisor brackets, similar wire bending was performed. Step 6:- A sleeve was inserted before placing wire in mouth.
Mode of activation
There are two ways of activation of 2X2 appliance, first, place the appliance in secure with modules in anterior portion and cinch back at distal wire tightly ; with the help of three prong pliers 5mm away from mesial side of tube a V bend is given. Second, give V bend check that anterior portion of wire should touch base of buccal sulcus [5].
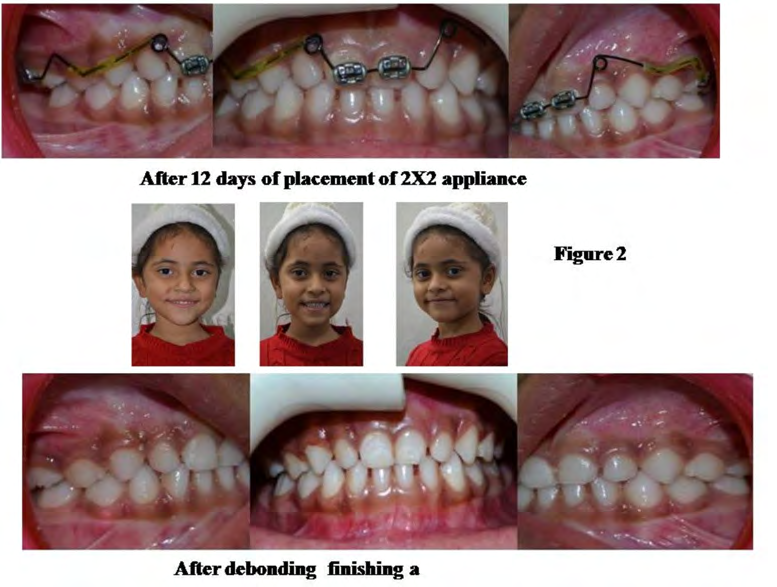
Once the appliance is activated, it intrudes the anterior; but during intrusion as the force of application is away from the centre of resistance teeth get flared. In addition, we have incorporated helix which flares teeth buccal side. Treatment Outcome Total treatment time was 12 days, this is fairly related to the short treatment time required to totally correct anterior cross-bite in primary dentition. Post treatment records confirm that the treatment objectives were accomplished. Facial photographs illustrate an enhanced profile and an attractive smile. Complete pictorial illustration of treatment out is given in figure 2.
Pre-treatment occlusion was maintained i.e. Class I canine and mesial step in transplane occlusion. Reverse ovejet and overbite was correct to its idyllic relation. Suitable alignment and nice gingival contour were accomplished.
The post-treatment lateral cephalometric radiograph
demonstrates a fair facial profile.Cephalometric investigation confirm a Class I skeletal relationship, the ANB angle reduced to ideal, as did the nasolabial angle. Dental measurements potentially have changed, and a functional and good-looking occlusal result was achieved and maintained. Most significant part is that the patient and her parents were pleased with her teeth and profile.
Discussion
One of the prime objectives of pediatric dentistry is to maintain ideal growth and development of craniofacial region guiding through developing dentition4. Any delay in diagnosis and treatment of primary dentition malocclusion during period of primary or mixed dentition results in facial deformity [4, 2].
The period of primary dentition offers the greatest opportunity to correct occlusal disturbance future growth modification; delay at this stage may become more complicated treatment at later stage of maturity [4, 3],. Thus goal of our treatment is to tip the affected maxillary teeth labially to correct cross bite and establish normal overjet/ overbite relationship The 12 days of treatment time may seem shorter than average, but patients with anterior cross bite especially palate erupted two primary central incisors are perceived to be more time-consuming to treat than average patients. It is of extreme significance in this case is to avoid detrimental side effects like the extrusion of primary second molars, and root resorption.
The turbo’s with blue bite was placed on lower primary second molar to control the extrusive movement of upper primary second molars and it opens anterior bite facilitating speed correction. With placid, cautious placement of helix in arch wire and careful activation of activation with three prong pliers intrudes and proclains anterior teeth helps in achieving primary objective of treatment [4, 5].
The aim of our treatment was to correct anterior cross bite and has been achieved with buccal tipping / flaring. Utmost care has taken to avoid root torque which may alter the path of eruption permanent dentition. Thus, only round wire was used.
Despite the shortest treatment time, the potential root resorption was observed. The overall treatment time and the biological result achieved were well worth. This appliance can use in permanent dentition, if the appliance fabricate with 16’X22 ‘blue Elgiloy wire can induce root torque. Further, incorporation of 3mm internal diameter helix reinforces protrusion initiated with 2X2 appliance and it avoids extrusion of anchor teeth. Scope for the case report is to compare the results with round and rectangular wires.
Conclusion
The above mentioned cases report well describe that 2X2 appliance is a suitable alternative for correction of anterior dental cross bite instead of complicated fixed orthodontic tooth movements. In this report primary objective of correcting anterior cross bite was achieved in 12 days. The design of this modified 2 by 2 appliance allows buccal tipping of teeth, helix can provide light and continuous buccal tipping force with minimal root resorption.
Why this Case Report is Important
- Maxilla follows the neural growth pattern, it completes at the age of 6-7 years; the developing cranial base influence maxillary growth. (Either drift or displacement mode).
- In anterior cross-bite, the growing maxilla exerts forces directly on mandible resulting in anterior displacement of chin develops concave profile; this process occurs at primary dentition phase or pre-pubertal phase and at this age (4-9 years) patient consults to pediatric dentist.
- This appliance can be fabricated with any round wire, but if use of AJ wilcock provide light and continuous force; ease of fabrication, safety, less time consumption, least patient compliance requires.
References
-
Vadiakas G, Viazis AD (1992) Anterior crossbite correction in the early deciduous dentition. Am J Orthod Dentofacial Orthop 102(2): 160-162.
-
Kocadereli I (1998) Early treatment of posterior and anterior crossbite in a child with bilaterally constricted maxilla: report of case. Journal of Dentistry for Children 65(1): 41-46.
-
Tsai HH (2001) Components of anterior crossbite in the primary dentition. Journal of Dentistry for Children 68(1): 27-32.
-
Proffit WR (2007) The Biological Basis of Orthodontic Therapy. 4th (Edn.), In: Contemporary Orthodontics. St. Louis: Missouri, pp: 331-358.
-
Naidu S, Suresh A (2018) The Applications of 2 x 4 Appliances during Mixed Dentition Treatment. Acta Scientific Dental Sciences 2(11): 49-51.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey