Knowledge, Attitude and Practices of Radiology Residents of Tertiary Government Hospitals of Peshawar Regarding Biological Hazards Caused by X-Rays
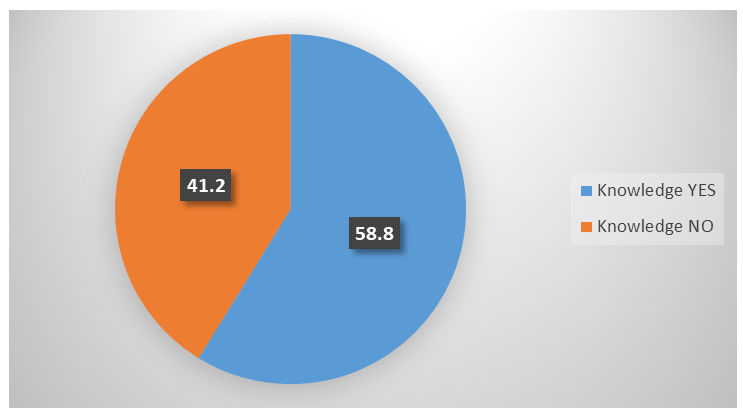
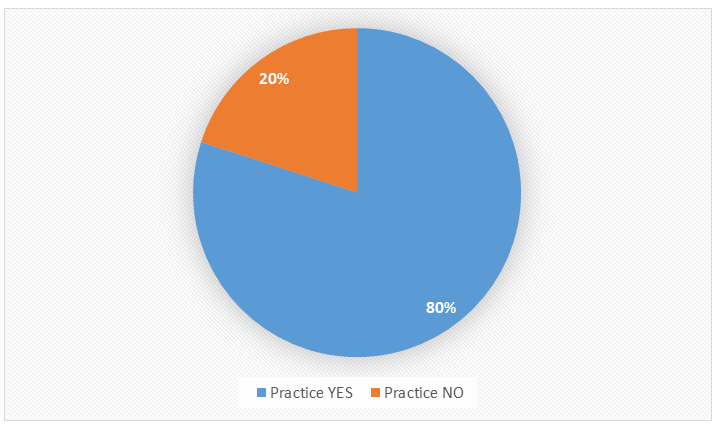
Background and Objectives: Pakistan is facing the problem of safe and quality services due to lack of relevant knowledge towards advance technology in the field of radiology. That’s why, we designed the present descriptive cross-sectional study to focus on the knowledge, attitude and practice regarding biological hazards caused by X-rays among residents in the department of radiology in Tertiary care Government Hospitals of Peshawar. A self-structured questionnaire was used for purpose of data collection. Convenient sampling was used. The collected data was compiled and analyzed by using SPSS version 23.0. Results: A total of 80 (58.8%) residents were found to have adequate knowledge about biological hazards of X ray radiations. While 20% were having adequate attitude and 80 % were having protected practice. Conclusion: The overall knowledge about biological hazards of X-rays among Radiology residents was adequate. However, there was poor attitude and satisfactory practices. There is need of regular training Programs and implementation of national legal law to reduce malpractice in radiations.
Introduction
Radiology has evolved from infancy to a magnitude of maturity after the discovery of X-rays by Roentgen in 1895. The multitude of the imaging modalities that had developed for the last 5 decades includes ultrasonology, radionuclide imaging, computed tomography (CT), magnetic resonance imaging (MRI) and digital subtraction radiography [1].
X-radiation is basically a form of electromagnetic radiation that has a wavelength of the range approximating 0.01 to 10 nm [1]. Diagnostics x rays are one of the biggest contributions to the radiation dose to population from sources that are man-made [2]. X-ray imaging has now attained a vital role in both diagnosis as well as other characterizations like quality assurance, security checks and material research. A leading advantage of X-ray imaging in comparison to other modalities, for example, magnetic resonance imaging (MRI), is that the image can be obtained very quickly, which helps in improved approach to multiple dynamic processes [3].
All ionizing radiations have effects on biological tissues. X rays also, being ionizing radiations, have impact on the biological tissues. These effects arise from the deposition of energy in the tissues that lead to changes in the chemical composition at nuclear and cellular level [4]. Effects of radiations are mainly of two categories, Stochastic and non- stochastic or deterministic. Stochastic effects are those for which there is no given dose threshold and their origin may have a probability in induction of damage to cells in tissues. These effects mainly include mutagenic and carcinogenic changes. The other type of effects is deterministic effects for which there is a probable dose of threshold below which effects are not observed. According to the intensity of the dose above the threshold, the effects re observed [5]. Deterministic effects are also given the name of non-stochastic effect. Variables that are important are time duration of exposure, dose and kind of radiation [6]. Some examples of these are effects on skin like erythema, irreversible damage to skin, loss of hair, sterility, cataracts and even fetal anomalies [7].
It is a one of the foremost responsibilities of a health- care professional to have firsthand knowledge of the hazards of radiological processes as health care provider advises the patients to perform. The knowledge may be a part of undergraduate curriculum in medical colleges. Many studies indicate that primary care providers are unaware of the biohazards that are associated with the use of radiation [8].
There are many studies held worldwide, that assessed that the knowledge, attitude, and practice (RP-KAP) of different health-care workers who work in a radiation environment and came up with different results [9, 10]. In one of the study majority of study participants had appropriate knowledge (72%), positive attitude (70%) but unsafe practices (65.5%) [9]. In a study carried out locally, it was found that about 40% students agreed that radiations are emitted from objects after any X-ray exposure and about the same percentage agreed that protective measures should be taken while performing an X-ray procedure. More than 1/3rd students observed that gamma rays are more harmful than X-rays and about the same number agreed that intravenous contrast used in angiogram also emits radiations. 67% students agreed that nuclear material used in medicine is potentially explosive while 18% were of the opinion that MRI emits ionizing radiation. 28% students agreed that as compared to other medical specialist, a radiologist have a shorter life span [11].
Diagnostic procedures in which ionizing radiations are used to diagnose medical diseases are the main source of radiation exposure to the general public. However, general background radiation on Earth is more as compared to these sources. The risks vs benefits of exposure to radiation for medical imaging must be defined clearly for patients and clinicians. It has been reported by US National Council on Radiation Protection and Measurement that X-rays and nuclear medicine are responsible for 15% of all radiation exposures [12, 13, 14].
Effects of Ionizing Radiations on Body
Radiation directly damages DNA through ionizing effects or indirectly through formation of free radical. When a low dose is delivered through a long duration of time, may give opportunity to the body to repair it. Signs of injury due to radiation may not appear in the short term, however effect may appear later in life. Unavoidable effects e.g. killing of cells can be immediate and have a threshold level above which severity increases with radiation dose. However, it is not necessary that the threshold is the same in every tissue or individual. Healing may results in fibrotic changes and necrosis in internal organs. It may result in acute radiation sickness, cataracts, and sterility. However acute effects require large doses e.g. 1-2 Sv or 1-2 Gy with x-ray exposure RWF of 1.
Effects that occur by chance, without a threshold level of dose, e.g. mutations, can result in cancer and hereditary effects. Induction of cancer may take long time. Estimation of risks of cancer associated with diagnostic x-rays using different tools for epidemiology is difficult because of different x-ray energies used at various institutions, extrapolation to low radiation doses and recall bias. Most of the low-dose ionizing radiation risk in human beings was evidenced from the survivors of explosion of nuclear bomb in Japan. Besides other sources of information are cellular mutation studies in laboratory and different strains of mice.
Regarding the effects of low dose radiation, debate is still going on in the scientists, whether the low dose-response curve is linear or nonlinear, and a threshold of adverse effect exists or not. Committee on Health Effects of Exposure to Low levels of Ionizing Radiations (BEIR VII) has concluded from studies that “biologic data are emerging on phenomena that could affect the shape of the dose-response curve at low doses [15].” It has been found that the latent period for induction of cancer, if it occurs at all, from ionizing radiation exposure of human varies from several years to more than 20 years [16].
Malformations induced during pregnancy from radiation are important examples of unavoidable effects of radiations. Different studies on survivors of nuclear bomb showed that organogenesis period from 3rd to 8th week were actually vulnerable period. Exposure to radiations between 8th to15th weeks can results in malformations of forebrain which results in mental retardation. It was found that the threshold dose during these periods of pregnancy was much lower i.e.100-200 mSv. However, high doses at 0.1 Sv to 1 Sv to the fetus can result in gross malformations or even death. Radiation exposure can also increase the risk of cancer in later childhood. Therefore pregnant women should always avoid ionizing radiations, if possible [6]. However x-ray of pregnant women can be done in certain unavoidable circumstances [17].
Other main side effects of radiation are hereditary effects. Radiation damages the gonads during the reproductive age by producing mutations in the gametes. Inherited diseases range from mild disorders to serious consequences, including severe mental defects or even death. However, no human studies have shown these hereditary effects from routine doses of background ionizing radiations. Furthermore, some studies of atomic bomb survivors in offspring have not shown statistically significant increase in hereditary defects or cancers [18].
Safety and Protection from Radiation
Safety and protection from radiation is main concern for all patients exposed to radiation, physicians and staff of the departments, including radiology procedures, is responsible for the greatest dose of radiation for all staff. Radiation from diagnostic imaging procedure, such as computed tomography, mammography, and nuclear imaging, are minor contributors. However, exposure to any radiation procedure possesses potential risk to patients as well as healthcare workers alike [19].
Main objective from radiation protection is to reduce unnecessary exposure to radiation to minimize the harmful effects of ionizing radiation [20]. In the field of medicine, ionizing radiation has become an inevitable tool used for the diagnosis as well as for the treatment of a variety of diseases. In medical settings, most of the radiation exposure occurs during fluoroscopic imaging, in which x-rays are used to obtain dynamic as well as functional imaging. Radiation protection training can help to reduce radiation exposure to staff as well as patients [21]. Radiation safety guidelines enforcement can be useful in this regard. It has been observed that many interventionists do not receive proper training in their residency on reduction of exposure to radiation dose. In particular, clinicians or staffs who uses fluoroscopic imaging or interventional departments has low adherence to guidelines for radiation safety. Fluoroscopic imaging is used in many specialties, including gastroenterology, orthopedics, urology, interventional radiology, interventional cardiology and vascular surgery. A thorough understanding of risks to radiation exposure and techniques to reduce the dose of radiation is of utmost importance as radiation exposure has become more prevalent.
Three basic principles of protection from radiation include: justification, optimization, and dose limitation. Justification involves an appreciation for the benefits and risks of using radiation for diagnostic procedures or treatments. Medical Professionals and radiologists play important role in the education of patients on the potential side effects of exposure to radiation. The benefits of radiation exposure should be very well clear to the medical professionals. Procedures in which the patients are exposed to relatively higher dose of radiation and the benefits outweigh the risks e.g. interventional vascular procedures are medically necessary. The Principal, As Low as Reasonably Achievable (ALARA), which was defined by the code of federal regulations, was created to ensure that all measures to reduce radiation exposure have been taken while acknowledging that radiation is an integral part of diagnosing and treating patients. Exposure to Radiation can increase the risk of chances of developing malignancy. These effects occur as a linear model in which there is no exact threshold to predict whether malignancy will develop or not. That’s why, the radiologists teach protection practices under the ALARA principle.
No study was conducted among Radiology Residents of Government Tertiary care Hospitals of Peshawar to evaluate the knowledge, attitude and practice about hazards of X-Rays. Therefore, this study was undertaken with main objective to evaluate knowledge, attitude and practices of radiology residents of Tertiary care Government Hospitals of Peshawar regarding biological hazards caused by X rays.
Materials and Methods
It was a cross sectional study conducted from September 2021 to March 2022 at Radiology departments of three Tertiary Government Hospitals, of Peshawar including Hayatabad Medical Complex, Khyber Teaching Hospital and Lady Reading Hospital. Ethical Approval was obtained from research committee of the respective hospitals and CPSP. A total of 136 radiology residents participated through a convenience sampling technique. The purpose, procedure, risk and benefits of the study were explained, and confidentiality was ensured prior to taking the informed consent of Radiology residents. The study included those radiology residents who were inducted from Year 1-4 of FCPS training in respective hospitals and have been performing residence since last six months. Those residents were excluded who refused to participate. A questionnaire was designed comprising of 20 questions to evaluate the knowledge, attitude and practice regarding biological hazards of X-rays. The initial 5 questions were related to background data of participant i.e. ID code of participant, name of Hospital, Age, gender and year of residency.
The remaining 15 questions were divided into 5 each related to Knowledge, Attitude and Practice of radiology residents about biological hazards of X Rays. These 15 questions were close-ended (Yes/No). A pilot study was performed first on 10 participants before proper starting the study to assess any difficulties in understanding the questionnaire. The questionnaire was provided to the study participants and clear instructions were given and were taken back after 30 minutes. For each correct response a score of 01 was given and those achieving 70% or above score was considered as having adequate knowledge, attitude and safe practices. All participants were assured that every possible measure would be taken to preserve the confidentiality and misuse of the data.
Data was collected and analyzed statistically by SPSS version 23.0. Mean and standard deviation was computed for age and knowledge score. Frequency percentages was calculated for the categorical variables like gender, year of residency of the participants and knowledge, attitude and practice (Yes/No). Effect modifiers like age, gender and year of residency were stratified to see the effect of these on outcomes. Post stratification Chi-square test was applied and p value ≤0.05 was considered as significant.
Results
This study was carried out on 136 radiology residents at the Department of Diagnostic Radiology, in HMC, KTH and LRH Peshawar. The Mean and SDs for age was 29.79 + 2.143. Tables 1-3 describe the frequency of participants according to age, gender and Year of Residency respectively.
| Frequency | |
| < 30 Years | 91(66.9%) |
| > 30 Years | 45 (33.1%) |
Table 1: Age Wise Distribution (n=136).
| Frequency (%) | |
| Male | 89 (65.4%) |
| Female | 47 (34.6%) |
Table 2: Gender Wise Distribution (n=136).
| Year of Residency | Frequency (%) |
|---|---|
| 1st Year | 12 (8.8%) |
| 2nd Year | 59 (43.4%) |
| 3rd Year | 53 (39.0%) |
| 4th Year | 12 (08.8%) |
Table 3: Frequency of Year of Residency (n=136).
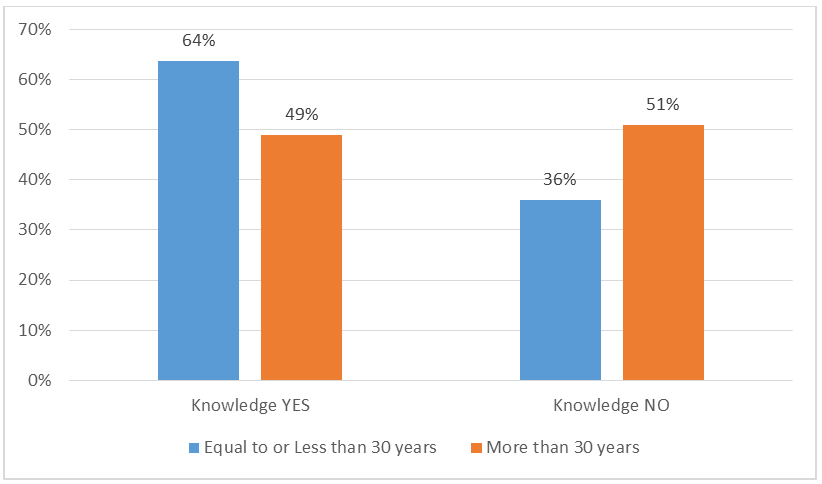
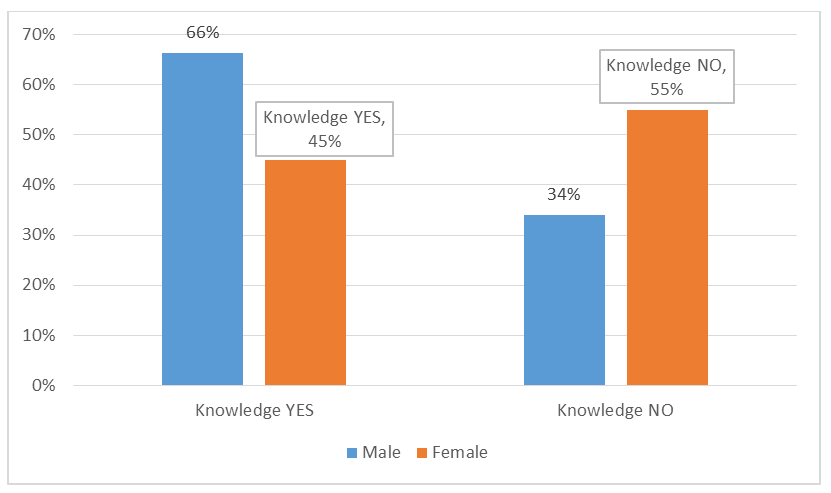
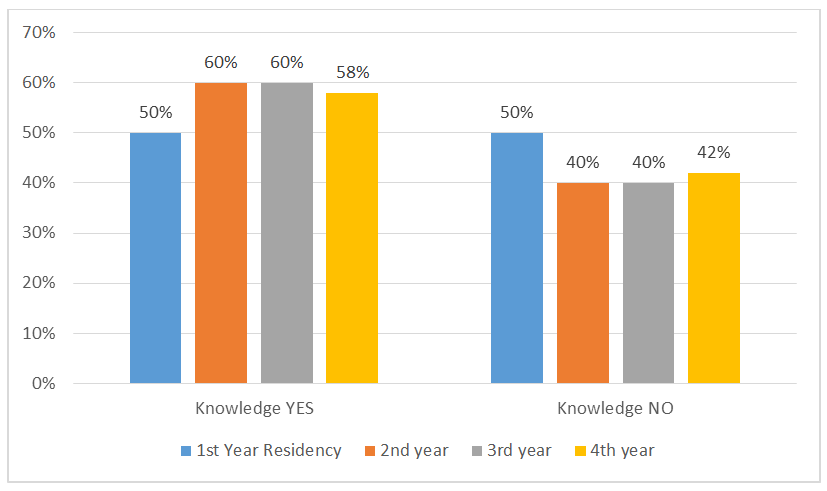
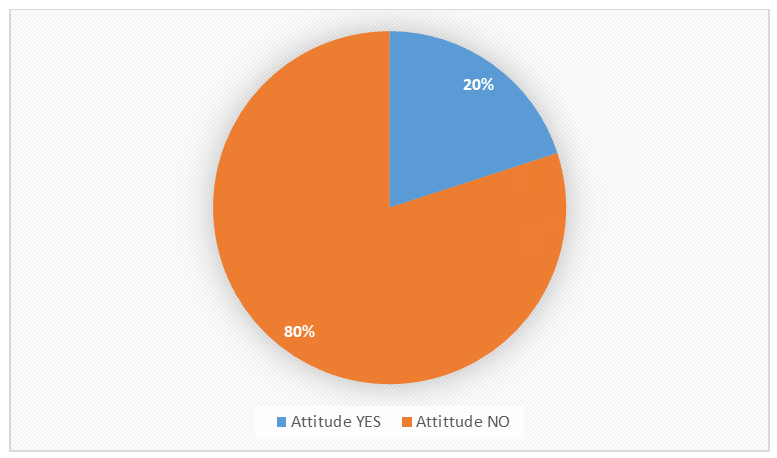
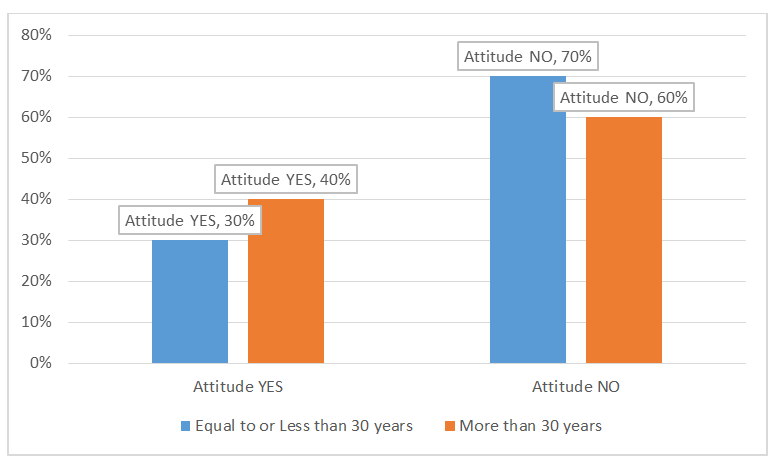
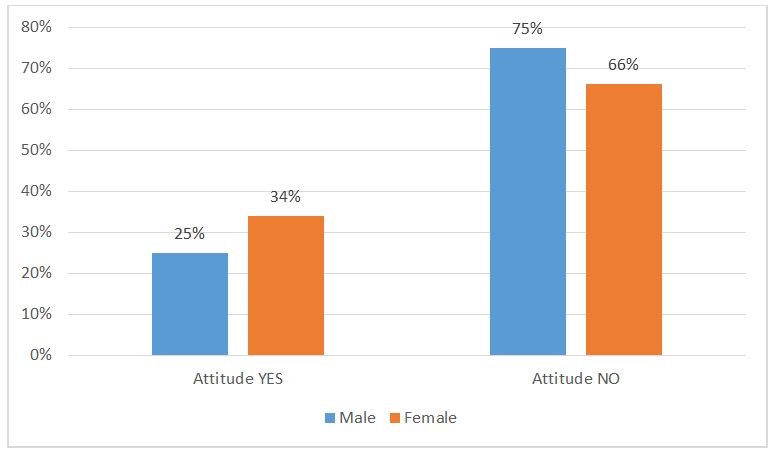
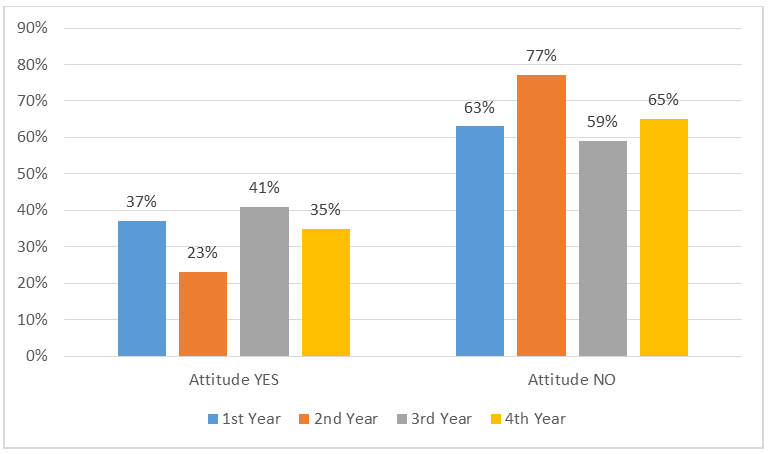
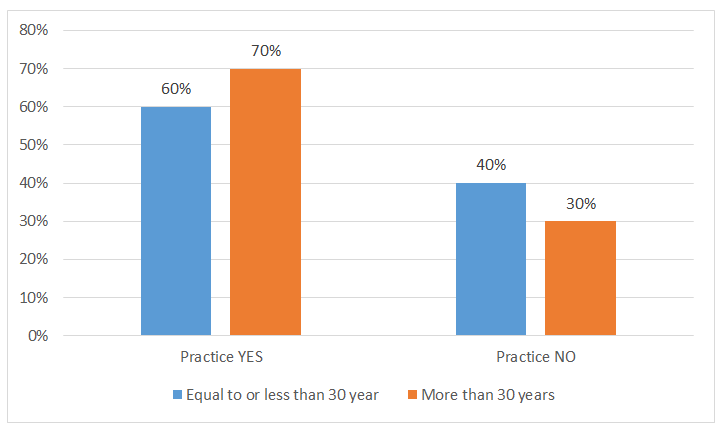
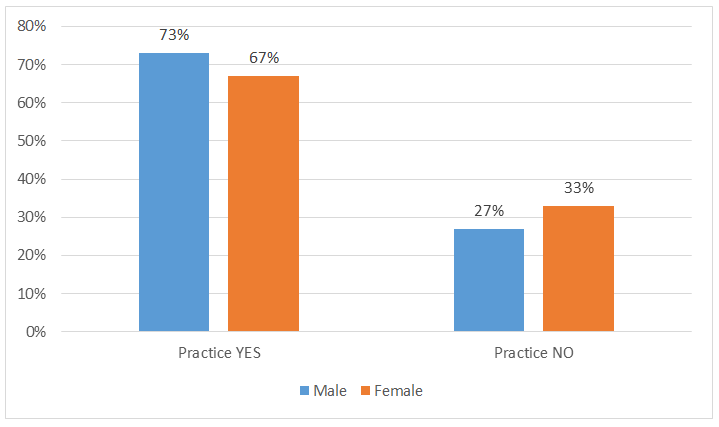
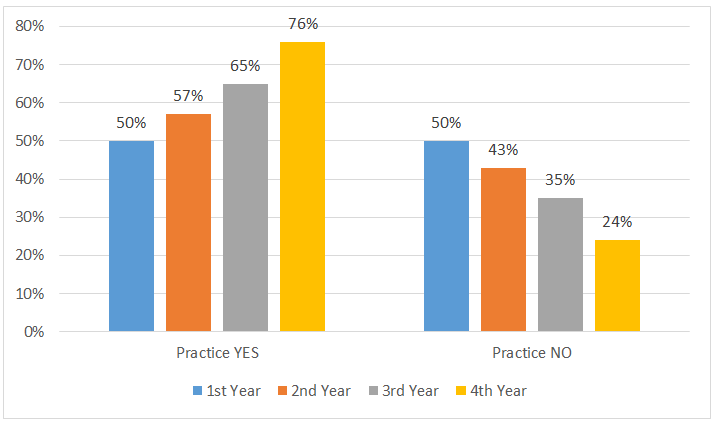
Figures 1 to 12 Depicts Frequencies of Knowledge, attitude and Practice (Yes or No) and stratification of Knowledge, Attitude and Practice versus age, gender and year of residency.
Discussion
This study highlighted the knowledge, attitude and practice of Radiology Residents regarding biological hazards of X Rays. Our study results show that although 58.8 % radiology residents were found to have knowledge of biological hazards, but the study population showed poor attitude (20 % positive) about these hazards. A total of 80% residents were having safe practice about protection from biological hazards of X rays. There are many studies held worldwide, that assessed that the knowledge, attitude, and practice (RP-KAP) of different health-care workers who work in a radiation environment and came up with different results [9, 10]. In one of these studies, maximum number of participants (72%) had appropriate knowledge, 70% had positive attitude but 65.5% had unsafe practice which is in agreement with the findings of our study [9].
In a local study it was concluded that 40% of the participants agreed that radiations are emitted from objects in the X-ray room after an X-ray procedure and about the same number agreed that protective measures should be taken while performing any procedure in the X-ray room and which was in agreement to the findings of our study. (58.8%) residents were having adequate knowledge about biological hazards of X ray radiations.
In a study carried out by Jha RK, et al. [21] it was concluded that there was average knowledge, poor perception and satisfactory practices of radiation risk among technical and non-technical staff of department of radiology [21]. In this study, the mean radiation awareness was 68.57% which was adequate. The level of knowledge regarding radiation protection among diploma graduates was 55.42 % which was in consistent with our study results. This implied that level of knowledge was higher in residents. Regular training courses should be arranged at regular intervals in institutions and also at national level [22].
In a study carried out in Gaza in Government Hospitals showed that knowledge, attitude, and practice of radiologists and radiographers was low/fair as compared to other countries like USA 82.5%, Pakistan 72% and 75%, Taiwan 65.8% and 61.8% among Iranian. These findings are in consistent with our study attitude and practice wise. These findings can be related to the lack of facilities and tools, the lack of standard protocols and regulations, and inadequate monitoring by the supervising authorities [23].
It has been observed that there is substantial need to improve awareness regarding protection from radiations for radiographers. In-service training for health care workers should be provided along with fresh documents with adequate radiation protection training protocols and guidelines. Further research work is required to justify the dose limits and the implementation of national protection legislation focusing on patient’s safety, linked with radiography practice. Our study may not be the first study regarding awareness of protection from radiations in Pakistan but we presume that our study will play a crucial role to improve the knowledge about it. We suggest that for proper awareness and understanding, it should be included in the curriculum at different training level of various diplomas and residency of technical staff.
Limitation of our study was that it does not represent whole population as it was conducted in only three tertiary care hospitals of Peshawar and small sample size (n=136). The results can be increased by performing studies in other teaching institutes of the province where these radiological facilities are available by including teaching and technical staff working in radiology department.
Conclusion
Our findings demonstrated that residents had adequate knowledge about biological hazards caused by X-rays, however, further improvement is warranted as most of the radiation-related hazards can be easily prevented by having proper KAP and continuous training at the institute level.
References
-
Doi K (2006) Diagnostic imaging over the last 50 years: research and development in medical imaging science and technology. Phys Med Biol 51(13): R5-27.
-
Verma M, Sonam AS (2016) Biological effects of X-rays on X-ray technicians. Int J Innov Res Sci Eng Technol 5(10): 18512-18516.
-
Bouzarjomehri FA (2004) Patient dose in routine X-ray examinations in Yazd state. Int J Radiat Res 1(4): 199- 204.
-
Gradl R, Dierolf M, Günther B, Hehn L, Möller W, et al. (2018) In vivo Dynamic Phase-Contrast X-ray Imaging using a Compact Light Source. Sci Rep 8(1): 6788.
-
Luntsi G, Daniel VS, Paul BT, Nwobi IC, Abdullahi AM, et al. (2018) Evaluation of low dose diagnostic X-rays induced effect on the white blood cells count in Guinea pigs. Int J Radiat Res 16(1): 129-132.
-
Eskandar O, Eckford S, Watkinson T (2010) Safety of diagnostic imaging in pregnancy. Part 1: X‐ray, nuclear medicine investigations, computed tomography and contrast media. Obstet Gynaecol 12(2): 71-78.
-
Choudhary S (2018) Deterministic and stochastic effects of radiation. Cancer Ther Oncol Int J 12(2): 555834.
-
Bolch WE, Dietze G, Henss NP, Zankl M (2015) Dosimetric models of the eye and lens of the eye and their use in assessing dose coefficients for ocular exposures. Ann ICRP 44(1 Suppl): 91-111.
-
Zafar M, Farhan A, Shaikh T, Rafiq R, Usman S, et al. (2016) Knowledge, attitude, and practices regarding radiological modalities among health-care providers, Karachi, Pakistan. Int J Heal Syst Disaster Manag 4(4): 132-138.
-
Dellie ST, Admassie D, Ewnetu Y (2014) An assessment of final-year medical students and interns awareness of radiation exposure to common diagnostic imaging procedures. Adv Radiol 2014: 1-7.
-
Mubeen SM, Abbas Q, Nisar N (2008) Knowledge about ionising and non-ionising radiation among medical students. J Ayub Med Coll Abbottabad 20(1): 118-121.
-
Ravikanth R (2018) Awareness of ionizing radiation and its effects among clinicians. World J Nucl Med 17(1): 1-2.
-
Krishnan S, Moghekar A, Duggal A, Yella J, Narechania S, et al. (2018) Radiation Exposure in the Medical ICU: Predictors and Characteristics. Chest 153(5): 1160- 1168.
-
Zeegers D, Venkatesan S, Koh SW, Low GKM, Srivastava P, et al. (2017) Biomarkers of Ionizing Radiation Exposure: A Multiparametric Approach. Genome Integr 8: 6.
-
Council NR (1998) Health effects of exposure to low levels of ionizing radiations: time for reassessment?. National Academies Press, Washington DC, USA.
-
Lowe SA (2020) Ionizing radiation for maternal medical indications. Prenat Diagn 40(9): 1150-1155.
-
Izumi S, Koyama K, Soda M, Suyama A (2003) Cancer incidence in children and young adults did not increase relative to parental exposure to atomic bombs. Br J Cancer 89(9): 1709-1713.
-
Lin EC (2010) Radiation risk from medical imaging. Mayo Clin Proc 85(12): 1142-1146.
-
Hamada N, Fujimichi Y (2014) Classification of radiation effects for dose limitation purposes: history, current situation and future prospects. J Radiat Res 55(4): 629- 640.
-
López M, Martín M (2011) Medical management of the acute radiation syndrome. Reports Pract Oncol Radiother 16(4): 138-146.
-
Jha RK, Nayak R, Subramanian U (2016) Knowledge, Attitude and Practice of radiation risk among employees in selected hospitals of Nepal. Janaki Med Coll J Med Sci 4(2): 10-18.
-
Clement CH, Rehani MM, Bjelac OC, Vañó E, Miller DL, et al. (2010) Radiological protection in fluoroscopically guided procedures performed outside the imaging department. Ann ICRP 40(6): 1-102.
-
Abo El-Aish ZM (2020) Knowledge, Attitude and Practice Assessment of Pediatric Radiation Protection Guidelines amongst Radiographers and Radiologists at Governmental Hospitals in the Gaza Strip. AUS Respository.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey