Clinical Profile and Outcomes of Respiratory Distress in Neonates A Cross Sectional Study
Background: Respiratory distress in neonates is a significant cause of morbidity and mortality worldwide. Understanding its prevalence and associated factors is crucial for effective management and preventive strategies. This cross-sectional study aimed to assess the prevalence and clinical profile and outcomes associated with respiratory distress in neonates admitted to the neonatal unit. Methods: Data were collected from neonates admitted to Miracle hospitals, medipally, Hyderabad, Paramitha hospitals, medipally, Hyderabad over period of 6 months. Clinical signs and symptoms of respiratory distress, demographic details, maternal history, and neonatal characteristics were recorded. Descriptive statistics were used to summarize the data, and multivariable logistic regression analysis was performed to identify independent predictors of respiratory distress. Results: 150 neonates included in the study those were diagnosed with respiratory distress. Preterm birth, low birth weight, maternal complications during pregnancy, and perinatal asphyxia were significantly associated with an increased risk of respiratory distress. Neonates born via cesarean section had a higher likelihood of respiratory distress compared to those born via vaginal delivery. Additionally, male gender and maternal smoking during pregnancy were identified as significant risk factors. The prevalence of Respiratory distress observed in males (60%) and in females (40%). Higher percentage of our study population belonged to the preterm babies (<38weeks). In the sample size of 150 patients, we observed 60 cases with TTNB, 40 Cases with HMD, 30 cases with MAS, 15 cases with congenital pneumonia & 5 cases with birth asphyxia. Conclusion: This study provides insights into the prevalence and associated factors of respiratory distress in neonates, highlighting the importance of early recognition and targeted interventions. Strategies targeting modifiable risk factors such as maternal smoking cessation and optimizing prenatal care may help reduce the burden of respiratory distress in neonates. Further research is warranted to explore additional factors and validate these findings in diverse settings.
Introduction
Background
Respiratory Distress Syndrome was the new naming for the illness in 1959 after Avery & Head 1 found that the pathophysiology of RDS included the impoverished generation of pulmonary surfactant (PS) in premature newborns known as “HMS”. Research on supplements to improve deficits in animal models of RDS has been carried out since the pathophysiology of the disease was described [1]. As the first artificial PS replacement therapy for neonatal RDS, Surfactant R was originally commercialized in Japan in 1986. Since then, numerous more comparable medicines have been created, marketed, imported, and utilized in Korea.
Respiratory Distress Syndrome (RDS)
RDS is a term used to describe a breathing disease that occurs in newborns, usually in preterm babies, and is caused by undeveloped lungs. The earlier a baby is born, the higher the chance that they may have RDS and require oxygen support to breathe. RDS is brought on by a baby’s lungs lacking enough surfactant [2]. It is characterized by tachypnoea (RR> 60cycles/min) where, the normal respiratory rate is 40-60 cycles / min in neonates. RD in neonates can because by TTNB then HMD, MAS, Congenital pneumonia & Birth asphyxia [3].
Classification: The classification of respiratory distress into 3 main categories: Mild, Moderate & Severe respiratory distress based on the Andersons Silverman score, APGAR & Down’s score by the following criteria:
| Category | Score |
|---|---|
| Mild Rd | 1-3 |
| Moderate Rd | 4-6 |
| Severe Rd | >6 |
Table 1: Respiratory Distress score.
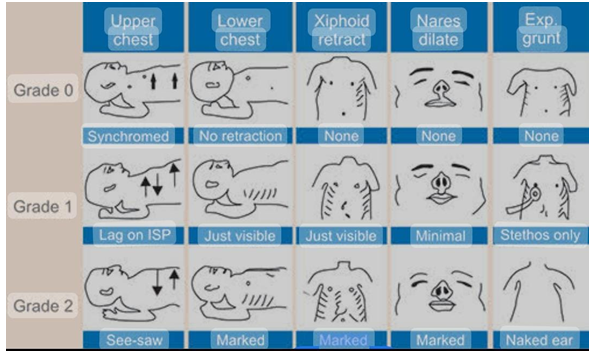
Andersons Silver Man Syndrome: Silverman Andersen respiratory severity score, which is assessed by physical exam, within 1 h of birth is associated with elevated carbon dioxide level and/or the need for increased respiratory support [4].

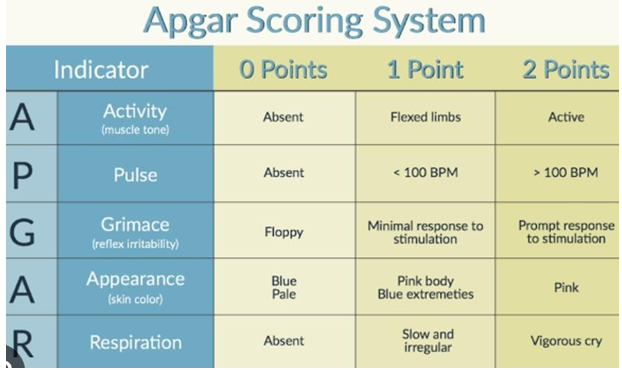
Apgar score: The Apgar score is a quick assessment tool used in pediatrics to evaluate the health and well-being of newborn babies immediately after birth. Developed by Dr. Virginia Apgar in 1952, the Apgar score helps healthcare professionals quickly determine if a newborn needs immediate medical attention or further observation [3]. Appearance (skin color): This criterion assesses the newborn’s skin color, with a score of 2 given for normal skin color, 1 for a body with normal color but blue extremities, and 0 for a completely blue or pale appearance. Pulse (heart rate): The pulse or heart rate of the newborn is evaluated, with a score of 2 for a heart rate over 100 beats per minute, 1 for a heart rate below 100 beats per minute, and 0 for no heartbeat [5]. Grimace (reflex irritability): This criterion evaluates the newborn’s reflexes or response to stimulation, such as a gentle pinch. A score of 2 is given if the newborn cries vigorously in response, 1 if there is only a grimace or weak cry, and 0 if there is no response at all. Activity (muscle tone): The muscle tone or activity level of the newborn is assessed, with a score of 2 given for active movement and flexion of limbs, 1 for some flexion or movement with resistance, and 0 for no movement or muscle tone [6]. Respiration (breathing rate and effort): This criterion evaluates the newborn’s breathing rate and effort. A score of 2 is given if the newborn is breathing well and crying loudly, 1 if there are slow or irregular breaths, and 0 if there is no breathing.
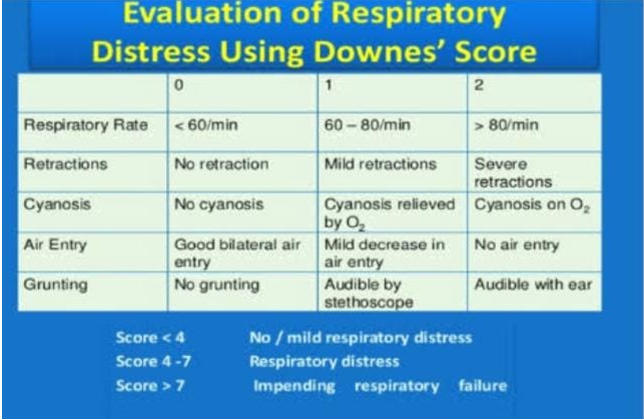
Downe’s Score: Downe’s score for assessing hyperoxaemia in neonates with respiratory distress. As per the study shown by USAID Indonesia that the downs score of <4 is shown no respiratory distress, the score of 4-7 are moderate risk of the respiratory distress and the score of >7 shown High rate of respiratory distress [7].
- Tachypnea (respiratory rate >60/min)
- Increased work of breathing
- Retractions (SCR, ICR & Xiphoid)
- Cyanosis (central & peripheral)
- Pallor / Poor perfusion (CRT >3 sec)
- Grunt
- Lethargy
- Poor oral feeding
- Apnea
- Tachycardia
Risk Factors
- Gestational age (Prematurity)
- Maternal history (LSCS, Consanguineous marriage & multiple births)
- Male gender
- Caucasian race
- Perinatal asphyxia
- Antenatal risk factors (maternal diabetes, asthma, hypertension, hypothyroidism & eclampsia)
- Cold stress or hypothermia
- Genetic disorder [8]
Causes of RD in Neonates
Transient Tachyapnea of the New Born:
- Most newborns experience transient tachypnoea, a condition that develops soon after birth and is caused by fatal lung fluid delaying after birth as a result of delayed or absent crying. This results in inefficient gas exchanges, respiratory distress, and tachypnoea.
- TTN usually appears 2–6 hours after birth, lasting 12– 24 hours in the majority of infants and 72 hours in a small percentage. It is particularly common in low birth weight babies (LSCS) because the fluid in the lungs fails to evacuate during vaginal birth.
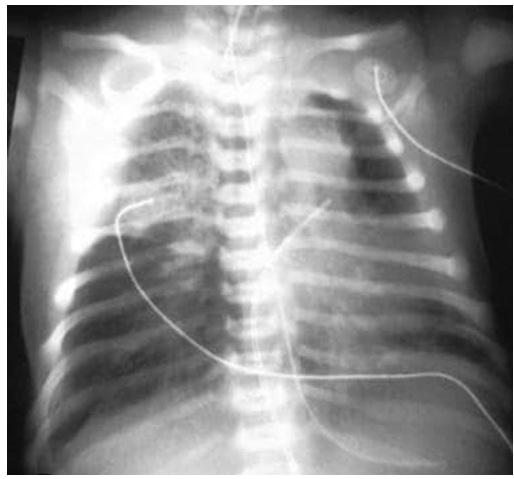
- Chest x-ray in the TTNB looks like retained lung fluid, streaky, interstitial opacities with hyperinflation and pleural effusions. It can be treated with the help of respiratory support depending upon the condition [9].
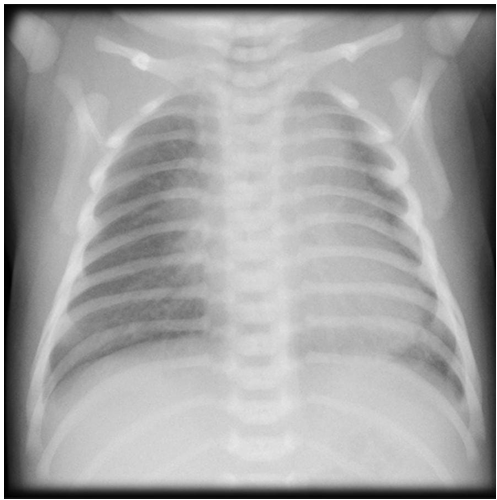
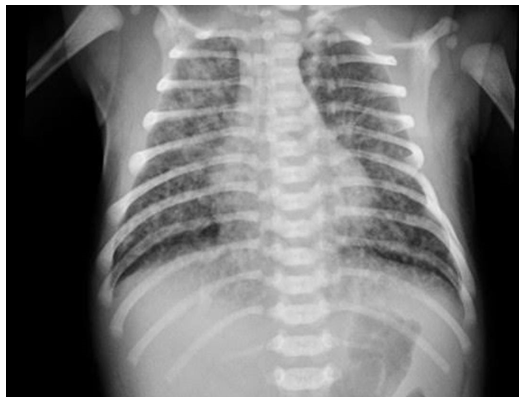
Hyaline Membrane Disease: HMD is also called as respiratory distress syndrome (RDS), a breathing disorder caused in new born whose lungs are not fully matured with surfactant deficiency which is most common in preterm babies. Chest X ray shows hypo aeration with bilateral fine granular opacities in the parenchyma & peripherally extending air bronchogram. It can be treated by the primarily as a prevention antenatal steroid, then respiratory support & exogenous surfactant [10].
Meconium Aspiration Syndrome: Neonatal respiratory distress occurs when a baby breaths in an assortment of amniotic fluid-the fluid surrounding the fetus and meconium, which is the newborn’s first stool. The chest x-ray displays patchy opacities, flattening of the diaphragm, and hyperinflation with atelectasis. It can be managed conservatively and with respiratory assistance [11].

Congenital Pneumonia/ Sepsis: All it is a pregnancy- related infection of the mother brought on by a set of beta hemolytic streptococcal infections; the agents are klebsiella, staphylococcus, enterobacter, and pseudomonas. Bilateral consolidation with decreased lung capacity and CRP < 6 mg/ dl are seen on the chest x-ray. There will be a substantial risk of death. It can be managed conservatively, with O2 support and antibiotic medication [11].
Birth Asphyxia: In this condition baby’s brain and other organs don’t get enough oxygen, blood and nutrients supply before, during and after birth. ABG shows the evidences of respiratory, metabolic or lactic acidosis. It can be treated by respiratory support and nebulisation steroid therapy.
Diagnostic Criteria: The diagnosis can be done based on clinical examination of signs and symptoms like increased work of breathing, tachypnoea, grunting, nasal flaring, retractions, cyanosis & poor perfusion. Chest X-Ray: Chest x ray findings in neonatal RD shows hypo aeration, atelectasis, which appears as a ground glass reticule granular with air bronchogram, bilateral infiltrates and patchy consolidation with low lung volume [12]. Arterial Blood Gases: ABG reveals hypoxemia, which implies need for the advancement of oxygen or respiratory support, some repeat ABG studies suggestive evidence of respiratory, metabolic & lactic acid acidosis. Other Investigations: Other investigations such as CBC shows anaemia, leucocytosis, abnormal blood cell count, CRP indicates sepsis or infection if >6mg/din case of any other susceptive infections CSF analysis, blood and urine culture will be performed. Shake Test: It can be performed on the gastric aspirate do determine the lung maturity, mix 0.5ml of gastric aspirate with 0.5ml of absolute alcohol in a test tube and shake well for 15 sec, formation of bubbles indicates adequate surfactant and less chance of RDS [13].
Treatment: The goals of effective neonatal respiratory distress syndrome management include reducing incidence and severity using antenatal corticosteroids, followed by optimal management with respiratory support, surfactant therapy, and conservative management.
- Antenatal corticosteroids.
- Respiratory support.
- Exogenous surfactant.
- Supportive care, including thermoregulation, nutritional support, fluid and electrolyte management, antibiotic therapy etc [14].
Antenatal Corticosteroids: Antenatal corticosteroid administration to pregnant women at risk of preterm delivery is a cornerstone in the management of NRDS. When provided, these steroids hasten the maturity of the fetus’ lungs, lowering the risk of infant respiratory distress syndrome and infant death. Corticosteroids such as betamethasone or dexamethasone promote lung maturity in the fetus, enhancing surfactant production and reducing the risk and severity of NRDS in preterm infants. Administration protocols typically involve a single or repeated dose regimen given to pregnant women at risk of preterm delivery within a specific gestational age window. Betnosol 6mg is given for 2 doses in 24hours or Dexamethasone 4 mg is given for 4 doses in 24 hours [11].
Respiratory Support: Nasal prongs oxygen: This is the initial oxygen support given through nasal mask here the oxygen flow rate will be 2l/min- 6l/min it can manage flow rate FiO2 from 24% to 44%.

- Optimal respiratory support is crucial in managing neonates with NRDS to ensure adequate oxygenation and ventilation.
- Non-invasive ventilation strategies such as nasal continuous positive airway pressure (CPAP) and nasal intermittent positive pressure ventilation (NIPPV) are preferred initial modalities to support respiratory function and prevent the need for invasive mechanical ventilation [15].
- Invasive mechanical ventilation may be required in severe cases or if non-invasive methods fail to provide adequate respiratory support.
High Flow Nasal Canula: Some facilities additionally utilize heated humidified high-flow nasal cannulas (HFNC) as an alternative to CPAP to give newborns with RDS positive displacing pressure ventilation. According to a clinical trial, HFNC is proven to be less effective than CPAP [16].

Continuous Positive Airway Pressure (CPAP): An initial strategy for preterm newborns with RDS or at risk for RDS without respiratory failure is nasal CPAP. There are numerous ways to provide CPAP, including ventilator- derived CPAP and a less expensive bubble CPAP device [17]. In the SUPPORT trial (Surfactant Positive Airway Pressure and Pulse Oximetry Randomized Trial), infants who received CPAP fared as well as infants who received prophylactic surfactant therapy along with mechanical ventilation. Infants who received CPAP earlier also required less surfactant therapy. Additionally, CPAP use reduced the incidence of BPD. The treatment aims to maintain SpO2 between 90 - 95% and PaCO2 between 45 - 65mmHg [18].
Non-invasive Respiratory Support: Although it is equally safe and expensive, nasal intermittent positive pressure ventilation (NIPPV) seems to be better than CPAP alone in lowering extubation failure, or the requirement for intubation in premature babies. The main difference between NIPPV and CPAP is that the former may provide the required pressures using a less expensive device, like a bubble CPAP, while the later needs a ventilator [19].
Mechanical Ventilation (MV): Endotracheal intubation and mechanical ventilation are used to treat patients who do not react to CPAP, experience respiratory acidosis (PH 7.2 and PaCO2 > 60-65 mm of Hg), hypoxia (PaO2 50mm of Hg or FiO2 > 0.40 on CPAP), or have severe apnea. In order to balance the dangers of barotrauma, polytrauma, and oxygen toxicity, mechanical ventilation aims to provide adequate respiratory support. Time-cycled pressure-restricted ventilation is the first-choice method of ventilation for preterm neonates with RDS. When pulmonary air leakage is a concern or a patient requires a lot of assistance from a conventional ventilator, high-frequency oscillatory ventilation (HFOV) and high-frequency jet ventilation (HFJV) are commonly used as emergency therapies. Additional strategies include the empirical application of high-frequency breathing to mitigate lung damage in extremely preterm babies [20].

Exogenous Surfactant Therapy: Using an endotracheal tube, intra-tracheal surfactant replacement therapy is the intended treatment for surfactant deficiency. When a premature newborn is given a surfactant within 30 to 60 minutes of birth, it has been shown to be advantageous. The use of surfactant speeds up healing and lowers the incidence of BPD, intraventricular hemorrhage (IVH), interstitial emphysema, pneumothorax, and infant mortality both in the hospital and after a year [21]. Nonetheless, there is a higher chance of preterm apnea in newborns treated with surfactant for existing RDS. As to the rules set forth by the European Census, newborns that are immature (FiO2 > 0.3) or mature (FiO2 > 0.4) are given the surfactant [20]. At similar dosages, there are currently no clinically meaningful benefits to using one kind over another. Beractant: This is a modified natural surfactant prepared from minced bovine lungs with the additives Poractant alfa: This is a modified natural surfactant derived from minced porcine lung extract Calfactant: This is a natural surfactant obtained from ravaging calf lung alveoli and contains 80% phosphatidylcholine with only 1% protein Synthetic surfactant: Clinical trials are ongoing [17, 18].
Surfactant is administered either by standard endotracheal intubation, which needs experienced practitioner or through less invasive surfactant administration (LISA) technique like aerosolized nebulized surfactant preparations, laryngeal mask, pharyngeal instillation, and thin intratracheal catheters [22]. The standard technique of surfactant administration by endotracheal intubation and mechanical ventilation may result in transient airway obstruction, pulmonary injury, pulmonary air leak, and airway injury. Emerging evidence shows that the LISA technique is associated with a lower rate of BPD, death, and need for mechanical ventilation compared to surfactant administration through endotracheal intubation. Still, further investigations are required to prefer the LISA technique as the standard technique of surfactant administration in place of endotracheal intubation. If the neonates maintain adequate respiratory drive with FiO2 <0.3, it should be planned to stop surfactant and switch to CPAP. Oxygen saturation (>90%), thermoregulation (36.5 to 37.5°C), and fluid and nutrition status should be monitored [23].
Supportive Care: Preterm infants with apnea of prematurity may require caffeine therapy. Caffeine can also be administered to preterm infants < 28 weeks with extremely low birth weight (BW <1000g) to increase respiratory drive and enhance the use of CPAP. There was a low incidence of BPD and earlier extubation in preterm infants who received caffeine compared to placebo.
During RDS’s early stages, proper fluid and electrolyte control is essential. Certain neonates might need to have their volume restored with the help of crystalloids and vasopressors to treat hypotension. Optimizing thermoregulation, nutritional assistance, blood transfusions for anemia, treatment for hemodynamically severe PDA, and antibiotic medication when needed are all included in the overall care of a premature newborn. I/V/O: Infection; IV The primary antibiotics used in antibiotic therapy include inj.taxim, inj.pipzo, inj.gentamycin, inj.monocef, inj.amikacin, and others, depending on the weight and condition of the infant [24].
Need of Study
Prevalence and Impact: a. RDS is one of the leading causes of respiratory distress in premature infants, particularly those born before 34 weeks of gestation.
b. Its prevalence is substantial, with a higher incidence among infants born at earlier gestational ages, contributing significantly to neonatal morbidity and mortality rates worldwide. c. Studying RDS helps in understanding its epidemiology, risk factors, and impact on neonatal health outcomes, facilitating targeted interventions and healthcare policies [25].
Pathophysiology and Mechanisms: a. RDS arises due to surfactant deficiency in the immature lungs of preterm infants, leading to alveolar collapse, atelectasis, and impaired gas exchange. b. Investigating the underlying pathophysiological mechanisms of RDS elucidates the complex interplay of factors involved, including lung development, surfactant production, and pulmonary vascular function. c. Understanding these mechanisms is crucial for developing effective preventive strategies, diagnostic tools, and therapeutic interventions for RDS [26].
Early Identification and Diagnosis: a. Timely recognition and diagnosis of RDS are vital for initiating prompt management and improving neonatal outcomes. b. Research focusing on identifying biomarkers, imaging techniques, and clinical indicators for early detection of RDS enhances diagnostic accuracy and facilitates timely intervention, reducing the risk of complications and long-term sequelae [27].
Treatment and Management Strategies: a. Effective management of RDS requires a multidisciplinary approach encompassing pharmacological, respiratory and supportive interventions. b. Research endeavors aim to optimize existing treatment modalities such as antenatal corticosteroids, surfactant replacement therapy, and respiratory support strategies, as well as explore novel therapeutic approaches. c. Studying the efficacy, safety, and long-term outcomes of different treatment strategies informs evidence-based clinical practices and improves the quality of care for infants with RDS [28].
Prevention and Risk Reduction: a. Despite advances in neonatal medicine, preventing preterm birth remains a challenge. Therefore, strategies to reduce the incidence and severity of RDS are of paramount importance. b. Investigating modifiable risk factors, maternal interventions, and antenatal care practices can help mitigate the risk of preterm birth and subsequent RDS development. c. Research focusing on prenatal screening, prenatal counseling, and interventions to promote fetal lung maturity contributes to preventive efforts and enhances neonatal health outcomes [21].
Quality Improvement and Healthcare Delivery: a. Continuous quality improvement initiatives in neonatal care necessitate ongoing research and evaluation of RDS management protocols and healthcare delivery practices. b. Studying the implementation of evidence-based guidelines, standardized protocols, and quality improvement strategies enhances healthcare delivery efficiency, reduces variability in clinical practice, and ensures optimal outcomes for infants with RDS [29].
Aims and Objectives
- To evaluate which gender & gestational age was more in number born with RD in neonates.
- To evaluate the efficacy of supportive care for RD in neonates.
- To study the major cause of RD.
- Based on the parameters (RR, HR, and SPO2 & CYANOSIS) & investigations (CXR & ABG).
- To determine the prevalence and severity of respiratory distress in neonates
- To identify the risk factors associated with respiratory distress in neonates
- To evaluate the management approaches and their effectiveness in treating respiratory distress in neonates
- To analyze the short-term and long-term outcomes of neonates with respiratory distress
Materials and Methods
Study Procedure
- Subjects with RD are selected based on inclusion and exclusion criteria.
- Demographic data was collected from patient’s records.
- Based on age diabetes mellitus patients were divided into 2 groups.
- Group- 1 (Preterm babies) - <38 weeks.
- Group- 2 (Term babies) - >38 weeks
- RD in many cases chest X ray findings correlated with the clinical Picture. Chest X ray in RD shows complete white lungs (hypo aeration), bilateral fine granular opacities in the pulmonary parenchyma extending air bronchograms, ABG – hypoxemia (Respiratory acidosis), Cyanosis, tachypnoea, retractions & grunt.
- The data collected throughout 6 months from 150 patients were analysed.
- The summarized data was entered in Microsoft excel.
- Statistical calculations were done by using chi-square test and ANOVA.
- Patients were separated based on gestational age, causes of RD & gender.
Statistical Analysis: One Way and Two Way anova
Assessment of Respiratory Distress: Respiratory distress was diagnosed based on clinical signs and symptoms observed by attending healthcare providers and documented in the medical records. Severity of respiratory distress was categorized based on validated scoring systems such as the Silverman-Anderson respiratory severity score or Downe score. Statistical Analysis: Data were analyzed using appropriate statistical software (e.g., SPSS, R). Descriptive statistics were used to summarize demographic and clinical characteristics. Prevalence of respiratory distress and associated factors were calculated with appropriate measures of association (odds ratios, relative risks, etc.). Multivariable logistic regression analysis was performed to identify independent predictors of respiratory distress, adjusting for potential confounders.
Study Conducted: St Theresa Hospital, Sanathnagar, Hyderabad. Miracle Hospitals, Medipally, Hyderabad. Paramitha Hospitals, Medipally, Hyderabad. Study Type: Cross Sectional Study Study Period: 6 Months Inclusion Criteria: Respiratory Distress Babies. Neonates (Late Preterm / Term) Inborn & Out Born Babies Admitted In Nicu. Exclusion Criteria: Infants >1month. Comorbid Babies Source of Data: Patient data records:
- Patient demographic details
- Antenatal risk factors
- Maternal history
- Presenting complaints
- Gestational age Data Collection: Data collection form including patient’s demographic details, antenatal risk factors, maternal history, presenting complaints & Gestational age. Vital Examination: To estimate the prevalence of respiratory distress, include lists from general practitioners. Sample Size: 150 Patients.
Results and Discussion
According to our study, the prevalence of Respiratory distress observed in males (60%) and in females (40%). Higher percentage of our study population belonged to the preterm babies (<38weeks). In the sample size of 150
patients, we observed 60 cases with TTNB, 40 Cases with HMD, 30 cases with MAS, 15 cases with congenital pneumonia & 5 cases with birth asphyxia. We observed that the majority of parameter levels were managed by the antenatal steroid, respiratory support, exogenous surfactant & conservative management. Mostly, it will be managed by the respiratory support [30, 31, 32].
| Cause of Rd | No. of Male Patients | No. of Female Patients |
|---|---|---|
| TNTB | 35 | 25 |
| HMD | 24 | 16 |
| MAS | 20 | 10 |
| Congenital Pneumonia | 8 | 7 |
| Birth Asphyxia | 3 | 2 |
Table 2: No. of male and females affected by RD.
The following bar graph shows the causes of RD in Neonates.
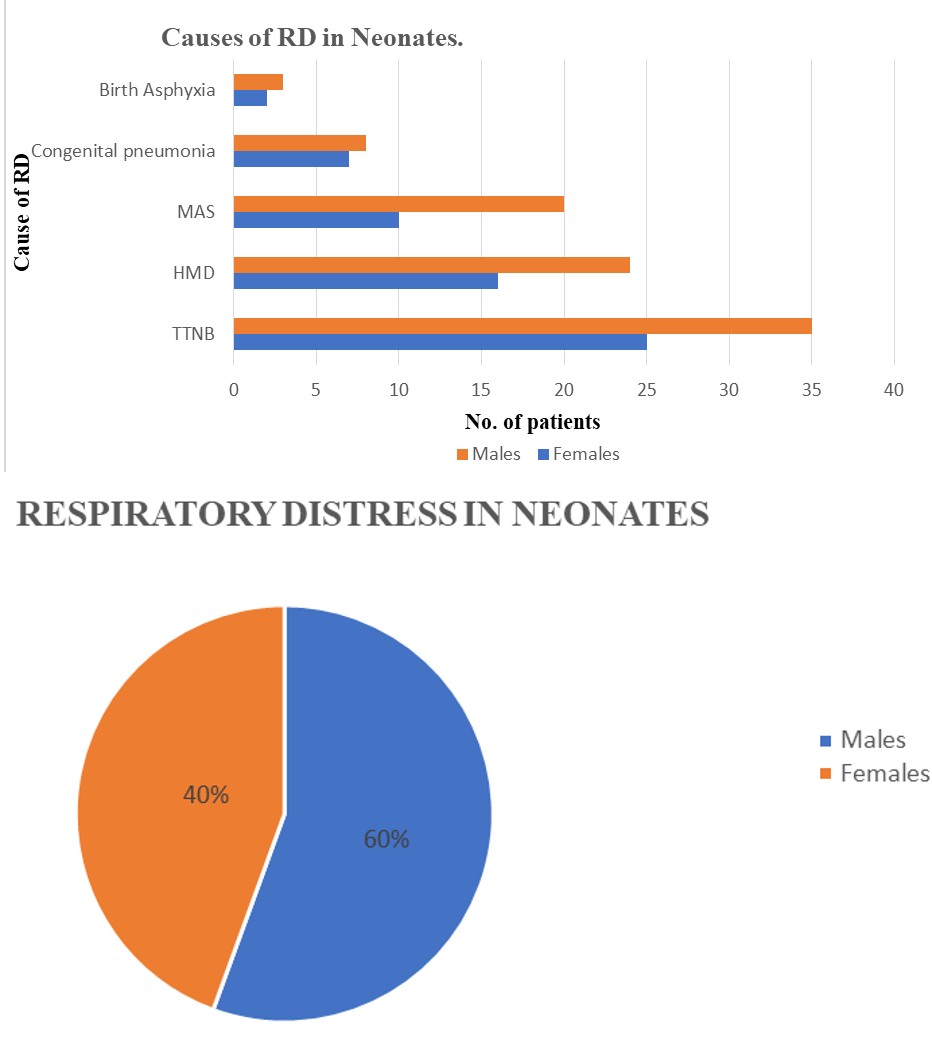
Figure 13A: Causes of RD in Neonates.
The following pie chart shows the prevalence of Respiratory distress observed in patients based on gender.
Figure 13B: RD in Neonates.
Conclusion
- Most of RD cases were seen in premature male babies with TTNB then HMD, MAS, Congenital pneumonia & Birth Asphyxia.
- Most of the preterm babies are born with RD because they are less for gestational age, low birth weight & immature organs (lungs).
- The supports used to treat RD are Antenatal steroids, Respiratory support & exogenous surfactant with these IV fluids, IV Antibiotics, IV Antiemetics, Proton pump inhibitors were included in the treatment.
- Early identification and proper management is important to secure better outcomes in neonates with RD.
The outcomes of neonatal RD were identified as a survival rate >95% and mortality rate <10%.
References
-
Meena LK (2021) Clinical Profile of Neonates with Respiratory Distress. International Journal of Medical and Biomedical Studies 5(1).
-
Naoom MB, Abdul ZAA, Alsaadi YA (2012) Respiratory Distress in Full Term Outborn Neonates: A Hospital Based Study. Journal of the Faculty of Medicine Baghdad 54(4).
-
Ma X, Xu X, Chen C, Yan C, Liu Y, et al. (2010) Epidemiology of Respiratory Distress and the Illness Severity in Late Preterm or Term Infants: A Prospective Multi-Center Study. Chinese Medical Journal 123(20): 2776-80.
-
Rao GC, Rao MSP (2017) Etiological Profile of Respiratory Distress in First Day of Life of a Newborn Baby. International Journal of Contemporary Pediatrics 4(1).
-
Ali ML, Jabbar N, Hannan A, Azher (2019) Etiology and Frequency of Respiratory Distress in Neonates: A Cross Sectional Study Conducted in Tertiary Care Hospital, Lahore. The Professional Medical Journal 26(11).
-
Nema A, Mittal SK (2019) Clinical Profile of Neonates with Respiratory Distress. International Journal of Medical and Biomedical Studies 3(7).
-
Fedakar A, Aydogdu C (2011) Clinical Features of Neonates Treated in the Intensive Care Unit for Respiratory Distress. The Turkish Journal of Pediatrics 53(2): 173-179.
-
Palod PH, Lawate BB, Sonar MN, Bajaj SP (2017) A Study of Clinical Profile of Neonates with Respiratory Distress and Predictors of their Survival Admitted in Neonatal Intensive Care Unit of Tertiary Care Hospital. International Journal of Contemporary Pediatrics 4(6).
-
Lamichhane A, Panthee K, Gurung S (2019) Clinical Profile of Neonates with Respiratory Distress in a Tertiary Care Hospital. JNMA: Journal of the Nepal Medical Association 57(220): 412-415.
-
Wapner RJ (2013) Antenatal Corticosteroids for Periviable Birth. Seminars in perinatology 37(6): 410- 413.
-
Bae CW, Kim CY, Chung SH, Choi YS (2019) History of Pulmonary Surfactant Replacement Therapy for Neonatal Respiratory Distress Syndrome in Korea. Journal of Korean medical science 34(25): e175.
-
Olicker AL, Raffay TM, Ryan R (2021) Neonatal Respiratory Distress Secondary to Meconium Aspiration Syndrome. Children (Basel) 8(3): 246.
-
Kommawar A, Borkar R, Vagha J, Lakhkar B, Meshram R, et al. (2017) Study of Respiratory Distress in Newborn. International Journal of Contemporary Pediatrics 4(2): 490-494.
-
Hailman M, Merritt TA, Schneider H, Epstein BL, Mannino F, et al. (1983). Isolation of Human Surfactant from Amniotic Fluid and a Pilot Study of its Efficacy in Respiratory Distress Syndrome. Pediatrics 71(4): 473- 482.
-
Poerio A, Galletti S, Baldazzi M, Martini S, Rollo A, et al. (2021) Lung ultrasound features predict admission to the neonatal intensive care unit in infants with transient neonatal tachypnoea or respiratory distress syndrome born by caesarean section. Eur J Pediatr 180(3): 869- 876.
-
Barsotti M, Chundu V, Silvka S, Sephus J, Hallman M (1996) Hemodynamics of respiratory failure in rabbit model effect of surfactant supplementation. Lung 174(4): 255-268.
-
Rachuri H, Oleti TP, Murki S, Subramanian S, Nethagani J (2017) Diagnostic performance of point of care ultrasonography in identifying the etiology of respiratory distress in neonates. Indian J Pediatr 84(4): 267-270.
-
Bacha, Lensa T, Tesfaye GE (2022) Clinical outcome and associated factors of respiratory distress syndrome among preterm neonates admitted to the neonatal intensive care unit of Adama Hospital and Medical College. SAGE open medicine 10.
-
Carlo WA, McDonald SA, Fanaroff AA, Vohr BR, Stoll BJ, et al. (2011) Association of antenatal corticosteroids with mortality and neurodevelopmental outcomes among infants born at 22 to 25 weeks’ gestation. Jama 306(21): 2348-2358.
-
Haneda K, Hessel II EA, Thomas R, Huntsman LL (1986) Cardiovascular Response to Rapid Infusion of Lactated Ringer’s. Tohoku J Exp Med 149(4): 397-406.
-
Arun KP, Nandeesh R, Thomas G (2015) Neonatal respiratory distress a practical approach to its diagnosis and management. Pediatr Clin North Am 62(2): 453-469.
-
Reuter S, Moser C, Baack M (2014) Respiratory distress in the newborn. Pediatr Rev 35(10): 417-429.
-
Soltero RG, Hansbrough JF (1999) The effects of diaspirin cross-linked hemoglobin on hemodynamics, metabolic acidosis and survival in burned rats. J Trauma 46(2): 286-291.
-
Kumar A, Bhatnagar V (2005) Respiratory distress in neonates. Indian J Pediatr 72(5): 425-428.
-
Liszewski MC, Stanescu AL, Phillips GS, Lee EY (2017) Respiratory Distress in Neonates Underlying Causes and Current Imaging Assessment. Radiologic Clinics 55(4): 629-644.
-
Avery ME, Gatewood OB, Brumley G (1966) Transient tachypnea of newborn possible delayed resorption of fluid at birth. Am J Dis Child 111(4): 380-385.
-
Edwards MO, Sarah JK, Sailesh K (2013) Respiratory distress of the term newborn infant. Paediatr Respir Rev 14(1): 29-36.
-
Corsini I, Parri N, Gozzini E, Coviello C, Leonardi et al. (2019) Lung ultrasound for the differential diagnosis of respiratory distress in neonates. Neonatology 115(1): 77-84.
-
Saboute M, Kashaki M, Bordbar A, Khalessi N, Farahani Z (2015) The incidence of respiratory distress syndrome among preterm infants admitted to neonatal intensive care unit a retrospective study. Open Journal of Pediatrics 5(4): 285-289.
-
El-Gendy N, Kaviratna A, Berkland C, Dhar P (2013) Delivery and performance of surfactant replacement therapies to treat pulmonary disorders. Ther Deliv 4(8): 951-980.
-
Ersch J, Roth KM, Baeckert P, Bucher HU (2007) Increasing incidence of respiratory distress in neonates. Acta Paediatr 96(11): 1577-1581.
-
Yee W, Amin H, Wood S (2008) Elective cesarean delivery neonatal intensive care unit admission and neonatal respiratory distress. Obstet Gynecol 111(4): 823-828.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey