Role of Autologous Lipoaspirate Therapy in Wound Healing
Normal wound healing is a complex process which involves combination of diverse immunological and biological process. Lipoaspirate is a remarkable source of stem cells. Adult stem cells are easily isolated from a section of whole fat or lipoaspirate for application to burn wound to improve healing. In this study we used autologous lipoaspirate in a paediatric patient with burn wounds to face.
Introduction
Wound healing is a physiological response of a living being to physical, chemical, mechanical or thermal injury. The wound healing process consists of several phases: homeostasis, inflammation, proliferation/granulation, and remodeling/maturation. Still, when the healing course deviates from the normal path, the healing does not advance past the inflammatory phase. In case of burns, there will be deficiency in normal healing. In modern medicine, usage of scaffolds either natural or synthetic has become popular and been recognized.
Normal wound healing is a complex process which involves combination of diverse immunological and biological process.
It involves a cascade of carefully and precisely regulated steps and events that correlate with appearance of various cell types in wound bed at various stages of wound healing [1].
Wounds that failed to progress through the normal stages of healing frequently enter a state of pathologic inflammation that is a chronic wound state. Having mesenchymal stem cells (MSCs) immunomodulatory properties, they reduce inflammation by secreting cytokines that promote tissue repair in the lesion [2]. In this way, by reduce the inflammatory response, they can affect the wound’s ability to progress beyond the inflammatory phase and not to regress to a chronic wound state. Lipoaspirate is a remarkable source of stem cells. Adult stem cells are easily isolated from a section of whole fat or lipoaspirate, relatively less aggressive and painful method is needed to obtain the stem cells [3].
Materials and Methods
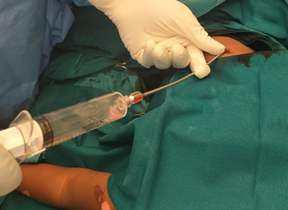
This study was conducted in Tertiary Care Centre in Department of Plastic Surgery after getting the department ethical committee approval. Informed consent was obtained. The subject was a 1yr - old female child who had accidental second degree scald burn injury which involves her left side of face, pinna and retro auricular region, left arm and forearm (Figure 1). She was taken to nearby hospital within 30min- inadequate initial resuscitation. Child developed blistering and swelling around left eye next day and presented to our center after a delay of 12hrs. She was admitted in tertiary burn care unit and initial resuscitation with intravenous fluids, analgesics and prophylactic antibiotics started. After tangential excision on post burn day 5, lipoaspirate therapy was done (Figure 2) .We used the technique described by Rigotti G, et al. [4] for the preparation of Autologous lipo- aspirate.
- Informed written consent is taken.
- The site for fat harvesting (lower abdomen) was cleaned and draped.
- Infiltrated the site with tumescent technique (100 ml of saline with 75 mg levobupivacaine, 40 mg mepivacaine and 0.5 ml of 1 in 1000 adrenaline).
- Connected a blunt 2-3 mun cannula to a syringe.
- small incision over the donor site was made.
- Inserted the cannula into subcutaneous tissue and gave negative pressure by pulling the plunger of the syringe. Fat is harvested using Coleman microcannula technique.
- Obtained approximately 10 ml of adipose tissue sample.
- Transferred the lipo-aspirate into the centrifugation tubes. Centrifuged at 3000 rpm for 3 minutes.
- After centrifugation 3 layers were formed.
- Top layer composed of oil from ruptured parcels of fat. Middle layer of compact adipose adipose tissue and cells. Bottom layer of blood and substances used for infiltration.
- Discard the top and bottom layer. The middle layer is used for lipoaspirate therapy.
- The harvested lipoaspirate was smeared over the wound and injected subcutaneously into the wound edges. (Figure 3).
- Wound inspection done on postoperative day 7 (Figure 4).



Results
Intraoperative and post-operative periods were uneventful for the patient. On post-operative day 7, dressing was opened and it showed significant areas of re-epithelialization and healing. All second degree superficial burn wound healed completely and islands of re- epithelization appeared in deep second degree burns areas. No complications and side effects were noted during entire procedure.
Discussion
The normal pace of wound healing and epithelialization is at the rate of 1mm/day. Optimum recovery requires the wound bed and the patient to be fit. To assist with implementing the concept of wound bed preparation, the TIME acronym was developed in 2002 by a group of wound care experts, as a practical guide for use when managing patients with wounds [5]. The TIME table summarizes the four main components of wound bed preparation:
- Tissue management
- Control infection and inflammation
- Moisture imbalance
- Advancement of epithelial edge of the wound The advanced wound healing therapies aim to hasten the process of wound healing by expediting the advancement of epithelial edge of the wound. Many growth factors have been used to advance the epithelialization. But the paradigm of wound healing is changing from repair of the tissue towards the regeneration of the tissue. The pre requisite for regeneration of tissue is the presence of stem cells in the wound environment.
Stem cell therapy is clinically applied as a safe and effective method for repair of several types of tissue damage [6, 7, 8]. Adult stem cells (ASC) are classified into hematopoietic stem cells (HSC) and mesenchymal stem cells (MSC) [9].” MSCs were first characterized in bone marrow, but many studies have reported the existence of MSCs in the connective tissue of several organs [10]. The most abundant and accessible source of adult stem cells is adipose tissue and MSCs have been obtained by lipo-suction of human adipose tissue [11]. The yield of MSCs from adipose tissue is approximately 40-fold greater than that from bone marrow [12]. Adipose Derived Stem Cells (ADSC) and their secretory factors have been investigated as a substitute for Bone Marrow Derived Stem Cells (BDSC), which offers a potential solution to skin repair and regeneration [13, 14]. ADSCs may exert their beneficial effects via complex paracrine mechanisms in addition to a building building function.
The wound-healing effect of ADSCs is mediated by secretory factors and the function is enhanced by hypoxia. Given their convenient isolation compared with BMSCs and extensive proliferative capacities ex vivo, ADSCs hold great promise for use in wound repair and regeneration [15].
Recently, evidence has accumulated that demonstrates the wound-healing effects of ADSCs [16]. ADSCs are physiologically located beneath dermal fibroblasts, and they may interact with them. However, ADSCs and their secretory factors may reach the epidermis in the case of skin damage. Hypoxia amplifies the paracrine effects of MSCs by enhancing the secretion of certain growth factors [17].
In our study we used lipoaspirate, harvested as per the technique described by Rigotti G, et al. [4]. In patients who are not fit for surgery/unwilling for surgery, we used ALA therapy as an adjunct to regular management of the wound. In this group of patients, ALA therapy accelerated wound healing and wound bed preparation for cover by SSG/flap. Due to small sample size statistical analysis could not be done. A randomized control study with adequate sample size with wounds of different etiology is desirable to substantiate the results.
Conclusion
The application of lipoaspirate which is a rich source of stem cells, in the treatment of second degree scald burns has been proven effective in this study. It hastens the overall healing time of second degree superficial and deep wound to within a week. Thus minimizing the total hospital stay and infection rates.
References
-
Broughton G, Janis JE, Attinger CE (2006) Wound healing: an overview. Plast Reconstr Surg 117(7): 1-32.
-
Ceresa C, Borrone A, Fracchia L, Rinaldi M, Marchetti A, et al. (2022) Lipoaspirate Shows In Vitro Potential for Wound Healing. Pharmaceutics 14(2): 447.
-
Strioga M, Viswanathan S, Darinskas A, Slaby O, Michalek J, et al. (2021) Same or not the same? Comparison of adipose tissue-derived versus bone marrow derived mesenchymal stem and stromal cells. Stem Cells Dev 21(14): 2724-2752.
-
Rigotti G, Marchi A, Galiè M, Baroni G, Benati D, et al. (2007) Clinical treatment of radiotherapy tissue damage by lipoaspirate transplant: a healing process mediated by adipose-derived adult stem cells. Plast Reconstr Surg 119(5): 1409-1422.
-
Schultz GS, Sibbald RG, Falanga V, Ayello EA, Dowsett C, et al. (2003) Wound bed preparation: a systematic approach to wound management. Wound Regen 11: 1-28.
-
Park BS, Jang KA, Sung JH, Park JS, Kwon YH, et al. (2008) Adipose-derived stem cells and their secretory factors as a promising therapy for aging. DermatolSurg 34(10): 1323-1326.
-
Schächinger V, Erbs S, Elsässer A, Haberbosch W, Hambrecht R, et al. (2006) Intracoronary bone marrow- derived progenitor cells in acute myocardial infarction. N Engl J Med 355(12): 1210-1221.
-
Schachinger V, Erbs S, Elsässer A, Haberbosch W, Hambrecht R, et al. (2006) Improved clinical outcome after intracoronary administration of bone-marrow- derived progenitor cells in acute myocardial infarction: final 1-year results of the REPAIR-AMI trial. European Heart Journal 27(23): 2775-2783.
-
Gregory CA, Prockop DJ, Spees JL (2005) Non- hematopoietic bone marrow stem cells: molecular control of expansion and differentiation. Exp Cell Res 306(2): 330-335.
-
Izadpanah R, Trygg C, Patel B, Kriedt C, Dufour J, et al. (2006) Biologic properties of mesenchymal stem cells derived from bone marrow and adipose tissue. J Cell Biochem 99(5): 1285-1297.
-
Kim WS, Park BS, Kim HK, Park JS, Kim KJ, et al. (2008) Evidence supporting antioxidant action of adipose- derived stem cells: protection of human dermal fibroblasts from oxidative stress. DermatolSci 49(2): 133-142.
-
Kern S, Eichler H, Stoeve J, Klüter H, Bieback K, et al. (2006) Comparative analysis of mesenchymal stem cells from bone marrow, umbilical cord blood, or adipose tissue. Stem Cells 24(5): 1294-1301.
-
Kim WS, Park BS, Sung JH, Yang JM, Park SB, et al. (2007) Wound healing effect of adipose-derived stem cells; a critical role of secretory factors on human dermal fibroblasts. J DermatolSci 48(1): 15-24.
-
Altman AM, Yan Y, Matthias N, Bai X, Rios C, et al. (2008) IFATS Series: Human adipose-derived stem cells seeded on a silk fibroin-chitosan scaffold enhance wound repair in a murine soft tissue injury model. Stem Cells 27(1): 250-258.
-
Liu TM, Martina M, Hutmacher DW, Hui JH, Lee EH, et al. (2007) Identification of common pathways mediating differentiation of bone marrow- and adipose tissue- derived human mesenchymal stem cells into three mesenchymal lineages. Stem Cells 25(3): 750-760.
-
Nambu M, Kishimoto S, Nakamura S, Mizuno H, Yanagibayashi S, et al. (2009) Accelerated wound healing in healing-impaired db/db mice by autologous adipose tissue-derived stromal cells combined with atelocollagen matrix. Ann Plast Surg 62(3): 317-321.
-
Park CH, Lee MJ, Kim JP, Yoo ID, Chung JH, et al. (2006) Prevention of UV radiation-induced premature skin aging in hairless mice by the novel compound Melanocin A. Photochem Photobiol 82(2): 574-578.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey