Usage of COX-1 and COX-2 Nanomedicines in Nanotechnology
Nanomedicine is the branch of medical applications in nanotechnology. Nanomedicine ranges from medical applications of nanomaterials, biological devices to nanoelectronic biosensors, molecular nanotechnology such as biological machines. It utilizes knowledge and tools of nanotechnology to prevention and treatment of disease. Nanomedicine involves use of nanoscale materials such as biocompatible nanoparticles for delivery, sensing or actuation in a living organism. COX inhibitors are a class of pharmaceutical compounds that selectively target and inhibit the activity of the enzymes cyclooxygenase-1 (COX-1) and cyclooxygenase-2 (COX-2). These enzymes are key players in the synthesis of prostaglandins, which are important mediators of inflammation, pain, and fever in the body. By modulating prostaglandin production, COX inhibitors have significant therapeutic implications in the management of various inflammatory conditions, pain relief, and fever reduction. COX-1 is constitutively expressed in many tissues and is involved in maintaining normal physiological functions, including the protection of the stomach lining and platelet aggregation. In contrast, COX-2 is induced at sites of inflammation and is primarily responsible for producing prostaglandins involved in the inflammatory response. The selective inhibition of COX-2 allows for targeted suppression of inflammation while preserving the beneficial functions of COX-1. Moreover, recent research has shed light on the complex interplay between COX-1 and COX-2 in health and disease. Emerging evidence suggests that the balance between COX-1 and COX-2 inhibition may have implications beyond pain and inflammation. Investigating the diverse roles of these enzymes in different tissues and pathologies may open up new avenues for drug development and personalized medicine. COX inhibitors represent an important therapeutic class with a profound impact on managing pain, inflammation, and related disorders. Understanding the differential regulation and functions of COX-1 and COX-2 is crucial for optimizing the clinical use of COX inhibitors and developing novel strategies for targeted and safer anti-inflammatory therapies.
Introduction to Nanomedicines
Application of nanotechnology for medical function has been characterized and is defined as the use of nanomaterials for monitoring, diagnosis, control, monitoring, prevention and treatment of diseases. Structures with one or more external measurements below 1 nm for instance fullerenes, graphene flakes and single wall carbon nanotubes are normally considered as nanomaterials [1].
COX Inhibitors
COX inhibitors are a class of drugs that target the enzymes cyclooxygenase (COX), which play a crucial role in the synthesis of prostaglandins. Prostaglandins are lipid molecules involved in various physiological processes, including inflammation, pain, and fever. By inhibiting the activity of COX enzymes, COX inhibitors reduce the production of prostaglandins, leading to anti-inflammatory, analgesic (pain-relieving), and antipyretic (fever-reducing) effects.
COX enzymes exist in two main isoforms: cyclooxygenase-(COX-1) and cyclooxygenase-2 (COX-2). COX-1 is constitutively expressed in many tissues and is involved in maintaining normal physiological functions, such as protecting the stomach lining and regulating platelet aggregation, which is essential for blood clotting. On the other hand, COX-2 is an inducible enzyme that is primarily activated at sites of inflammation and tissue injury. It is responsible for producing prostaglandins that promote inflammation and pain.
COX-1 is widely distributed in tissues throughout the body and is involved in the production of prostaglandins that support normal cellular functions. For example, in the stomach, COX-1-derived prostaglandins help maintain the integrity of the stomach lining, protect against acid damage, and regulate mucus production. In platelets, COX- 1 is critical for producing thromboxane A2, a prostaglandin that promotes platelet aggregation, leading to blood clot formation.
COX-2, on the other hand, is typically not expressed at significant levels in most tissues under normal conditions. However, in response to inflammation, tissue injury, or other stimuli, COX-2 expression is rapidly induced. The upregulation of COX-2 leads to the production of prostaglandins that contribute to the inflammatory response, causing pain, swelling, and redness at the site of injury or infection.
COX Inhibitors and Therapeutic Applications
Non-Selective COX Inhibitors: Traditional COX inhibitors, such as aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen and naproxen, are non-selective and inhibit both COX-1 and COX-While they effectively reduce inflammation and pain, they can also cause unwanted side effects, particularly in the gastrointestinal tract. Inhibition of COX-1-derived prostaglandins may lead to irritation of the stomach lining, increasing the risk of gastric ulcers and bleeding.
COX-2 Selective Inhibitors: In an effort to develop drugs with reduced gastrointestinal side effects, COX-2 selective inhibitors were introduced. These drugs specifically target COX-2 while sparing COX-1. COX-2 selective inhibitors, such as celecoxib, provide effective relief from pain and inflammation while minimizing the risk of gastrointestinal complications.
Clinical Applications: COX inhibitors are widely used in the treatment of various conditions, including: Inflammatory Disorders: COX inhibitors are prescribed for inflammatory conditions such as arthritis, where they help alleviate pain, reduce joint swelling, and improve mobility. Analgesia: They are commonly used for pain relief following surgeries, injuries, and dental procedures. Antipyretics: COX inhibitors help lower fever by reducing prostaglandin production in the hypothalamus, the region of the brain that regulates body temperature.
Limitations and Safety Concerns
While COX inhibitors are valuable therapeutic agents, they are not without risks. Non-selective COX inhibitors can cause gastrointestinal side effects, such as stomach irritation and ulcers. COX-2 selective inhibitors have been associated with an increased risk of cardiovascular events in some patients. As a result, careful consideration of individual patient profiles and potential risks is essential when prescribing COX inhibitors.
![Figure 1: Figure illustrates various methods of representation of nanomedicine [2].](/fulltextimages/10703/fig_1.png)
In conclusion, COX inhibitors play a pivotal role in managing inflammation, pain, and fever by targeting the COX
enzymes involved in prostaglandin synthesis. Their ability to selectively inhibit COX-1 or COX-2 provides the foundation for developing safer and more effective treatments for a wide range of medical conditions. However, their usage should be carefully assessed, and patients should be monitored for potential side effects to ensure optimal therapeutic outcomes.
In the above illustrations – lines, sticks, spheres, mesh, dots ribbon and cartoon are used to represent nanomedicine and surface is formed once molecules combine with the existing molecules in the living organism.
Drug Design-I
A nano material Drug simulation was performed to get the design for various drugs [2].
COX inhibitors which are also known as cyclooxygenase inhibitors, are a class of pharmaceutical agents commonly used to reduce pain, inflammation, and fever. They work by inhibiting the activity of the cyclooxygenase enzymes, namely COX-1 and COX-2, which play a crucial role in the production of prostaglandins. Prostaglandins are chemical messengers in the body that contribute to pain, inflammation, and fever.
In the context of nanomedicines, COX inhibitors can be incorporated into nanoparticles or other nanoscale drug delivery systems to improve their therapeutic efficacy and target specific sites of inflammation or pain. By utilizing nanotechnology, these medicines can enhance drug delivery, increase drug stability, and minimize side effects by focusing on specific tissues or cells.
Nanomedicines containing COX inhibitors have the potential to provide more targeted and controlled drug delivery, allowing for reduced dosages and minimizing systemic side effects. They offer promising opportunities for personalized medicine and improving patient outcomes in the treatment of various inflammatory conditions, including arthritis, inflammatory disorders, and pain management.
However, it’s essential to continue research and development to ensure the safety and effectiveness of COX inhibitor-based nanomedicines before widespread clinical use.
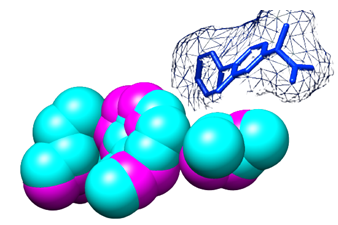
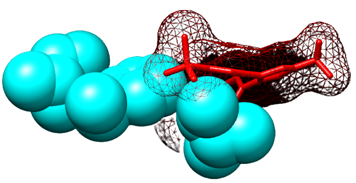
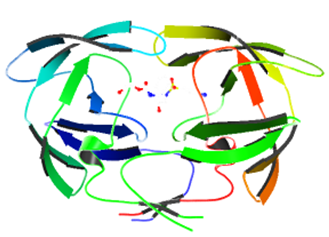
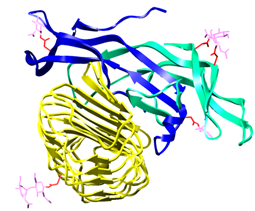
Figure 3: Figure illustrates flurbiprofen bound to COX-1 and COX-2 selective inhibitor SC-558 is bound to COX-2 Flurbiprofen is a nonsteroidal anti-inflammatory drug (NSAID) that belongs to the class of COX inhibitors. COX inhibitors work by inhibiting the activity of cyclooxygenase enzymes, which are involved in the production of inflammatory molecules called prostaglandins. By blocking these enzymes, COX inhibitors help reduce inflammation, pain, and fever.
In the context of COX-1 and COX-2 selective inhibition, certain NSAIDs like flurbiprofen are designed to preferentially target one of the two cyclooxygenase isoforms. COX-1 is constitutively expressed and is involved in maintaining normal physiological functions, including the protection of the stomach lining and platelet aggregation. COX-2, on the other hand, is induced during inflammation and plays a key role in generating prostaglandins that contribute to pain and inflammation.
When flurbiprofen binds to COX-1, it inhibits the enzyme’s activity, leading to the suppression of prostaglandin production. However, flurbiprofen’s selectivity towards COX- 1 is relatively moderate, and it can also inhibit COX-2 to some extent.
In contrast, SC-558 is a selective COX-2 inhibitor. It is designed to specifically target and bind to the COX-2 isoform, blocking its activity and reducing the production of prostaglandins that cause inflammation and pain. Selective COX-2 inhibitors like SC-558 were developed to minimize the gastrointestinal side effects associated with non-selective COX inhibitors, as COX-1 inhibition can lead to disruptions in the stomach lining.
By combining flurbiprofen and COX-2 selective inhibitor SC-558, researchers and pharmaceutical companies can study and compare their effects on different isoforms of cyclooxygenase. Understanding the selectivity and binding characteristics of these drugs to COX-1 and COX-2 is crucial for developing more targeted and effective treatments for inflammatory conditions while minimizing unwanted side effects.
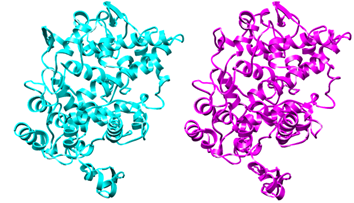
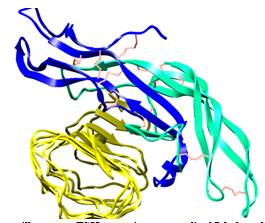
Superimposing COX-1 and COX-2 refers to the process of overlaying or comparing the three-dimensional structures of the two cyclooxygenase enzymes, COX-1 and COX-2. This superimposition is often done in the field of structural biology and drug design to understand the similarities and differences between these two enzymes at a molecular level.
COX-1 and COX-2 are isoforms of the cyclooxygenase enzyme, which play a crucial role in the production of prostaglandins, important signaling molecules involved in inflammation, pain, and other physiological processes. However, COX-1 and COX-2 have distinct functions in the body. COX-1 is constitutively expressed and is involved in maintaining normal physiological functions, such as protecting the stomach lining and promoting blood clotting. In contrast, COX-2 is induced during inflammation and is responsible for generating prostaglandins that contribute to pain and inflammation.
By superimposing the structures of COX-1 and COX-2, researchers can compare the active sites, binding pockets, and other critical regions of these enzymes. This comparison helps to identify the structural differences that contribute to their functional distinctions and selectivity for various drugs.
Understanding the structural differences between COX- 1 and COX-2 is essential for designing specific inhibitors that can selectively target one isoform over the other. This selectivity is crucial in drug development because it allows for the design of medications that can effectively treat specific conditions while minimizing potential side effects associated with non-selective inhibition of both COX isoforms. For example, COX-2 selective inhibitors were developed to target inflammation while sparing COX-1, which helps preserve the protective functions of COX-1 in the stomach lining and platelet aggregation.
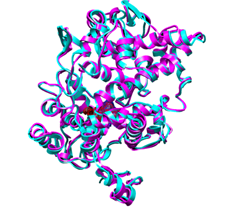
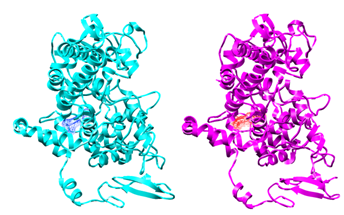
In the context of the cyclooxygenase enzymes (COX-1 and COX-2), the statement “Middle of residue is the same type in the two isoforms, the residues on either side are larger in COX-1 than in COX-2. One of these residues pushed the middle residue toward the active site” refers to a specific structural difference between the two isoforms.
Proteins, including enzymes like COX-1 and COX-2, are composed of chains of amino acids. Residues are individual amino acids within the protein sequence. The structure of a protein is crucial for its function, as it determines how the protein interacts with other molecules and carries out its biological role.
In the mentioned statement, the “middle residue” refers to a specific amino acid in the protein sequence of both COX- 1 and COX-2. This middle residue is of the same type (e.g., the same amino acid) in both isoforms.
However, the residues on either side of this middle residue are larger in COX-1 compared to COX-2. In other words, the neighboring amino acids in the COX-1 sequence are bulkier or more substantial than the corresponding neighboring amino acids in the COX-2 sequence.
As a result of this structural difference, one of the larger residues in COX-1 can exert a pushing force on the middle residue, moving it toward the active site of the enzyme. The active site is the region of the enzyme where catalytic reactions occur, and it is crucial for the enzyme’s function.
This structural variation between COX-1 and COX-2 can influence their selectivity for different ligands or substrates and may also impact their interactions with inhibitors or other molecules. Understanding these structural differences is essential for designing selective drugs that target either COX-1 or COX-2, depending on the desired therapeutic effects and potential side effects.
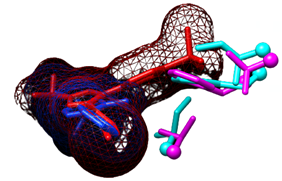
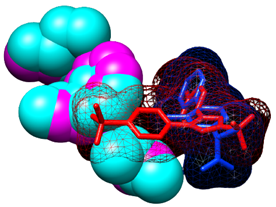
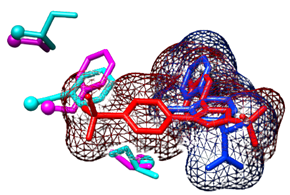
The statement “Inhibitor SC_558 is COX-2 selective because it can fit in the COX-2 site” refers to the selectivity of the inhibitor SC_558 for the COX-2 isoform of the cyclooxygenase enzyme.
Inhibitor SC_558 is a specific drug or molecule designed to target and inhibit the activity of COX-2, one of the two isoforms of the cyclooxygenase enzyme. As mentioned earlier, COX-2 is induced during inflammation and plays a significant role in generating prostaglandins that contribute to pain and inflammation.
The selectivity of SC_558 for COX-2 means that this inhibitor has a particular affinity and ability to bind to the active site or binding site of the COX-2 enzyme. The active site is a region within an enzyme where catalytic reactions take place. In the case of COX-2, it is the site responsible for the production of prostaglandins.
The structural features of SC_558 enable it to specifically fit into the active site of COX-2, blocking the enzyme’s activity and preventing the generation of prostaglandins associated with inflammation and pain.
In contrast, SC_558 has a weaker or limited binding affinity for COX-1, the other isoform of cyclooxygenase. COX- 1 is constitutively expressed and involved in maintaining normal physiological functions, including protecting the stomach lining and promoting blood clotting. The selectivity of SC_558 for COX-2 helps avoid interference with COX- 1’s essential functions, reducing the risk of unwanted side effects associated with non-selective COX inhibition.
The ability of SC_558 to selectively fit and interact with the COX-2 site makes it a promising candidate for targeted therapy in conditions where COX-2 activity contributes to inflammation and pain, while preserving COX-1’s physiological functions.
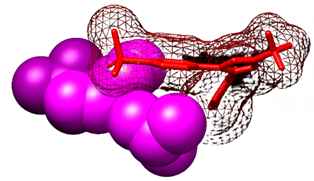
The statement “COX inhibitors are crowded out of the COX-1 site” refers to a phenomenon where certain COX
inhibitors, or drugs that target the cyclooxygenase enzymes, have difficulty binding to and inhibiting the COX-1 isoform of the enzyme.
COX inhibitors work by binding to the active site of cyclooxygenase enzymes (COX-1 and COX-2), which is the region responsible for the enzymatic activity of these proteins. By binding to the active site, COX inhibitors prevent the production of prostaglandins, which are inflammatory molecules.
However, the active site of COX-1 may be more tightly packed or “crowded” compared to the active site of COX- 2. This crowded nature of the COX-1 site can make it more challenging for certain COX inhibitors to access and bind to the site effectively. As a result, these inhibitors may have a weaker binding affinity for COX-1, making them less effective in inhibiting COX-1’s activity.
On the other hand, COX-2 inhibitors, which are designed to selectively target the COX-2 isoform, may have a better fit and binding affinity for the COX-2 site. This selectivity allows COX-2 inhibitors to effectively block COX-2 activity without interfering with COX-1 functions, thus reducing the risk of certain side effects associated with non-selective COX inhibition.
The crowded nature of the COX-1 site may influence the design and development of COX inhibitors to achieve selectivity and improve the therapeutic efficacy of these drugs. It highlights the importance of understanding the structural differences between COX-1 and COX-2 to develop drugs that can selectively target the desired isoform while minimizing unwanted effects on the other isoform.
The statement “Inhibitor flurbiprofen is nonselective because it fits well in the sites of the isoforms” refers to the property of the drug flurbiprofen as a nonselective COX inhibitor, meaning it can effectively bind to and inhibit both COX-1 and COX-2 isoforms of the cyclooxygenase enzyme.
Flurbiprofen is a nonsteroidal anti-inflammatory drug (NSAID) that belongs to the class of COX inhibitors. These drugs work by blocking the activity of the cyclooxygenase enzymes, which are involved in the production of prostaglandins, signaling molecules that contribute to pain, inflammation, and fever.
Unlike COX-2 selective inhibitors, which are designed to specifically target COX-2 while sparing COX-1, flurbiprofen can interact well with both COX-1 and COX-2 sites. It can bind effectively to the active sites of both isoforms, inhibiting their enzymatic activity and reducing the production of prostaglandins.
While nonselective COX inhibitors like flurbiprofen can provide broad anti-inflammatory and analgesic effects, they may also be associated with a higher risk of certain side effects. This is because COX-1 plays essential roles in maintaining normal physiological functions, such as protecting the stomach lining and promoting blood clotting. Inhibition of COX-1 can lead to gastrointestinal issues and disturbances in platelet aggregation.
The selectivity of COX inhibitors for different isoforms is an essential consideration in drug development, as it allows for the design of medications that can target specific conditions while minimizing potential side effects. COX- 2 selective inhibitors were developed to provide anti- inflammatory benefits without the gastrointestinal side effects associated with nonselective COX inhibition.
Drug Design-II
A second nano material Drug simulation was performed to get the design for various drugs (Hormone-Receptor Complex).
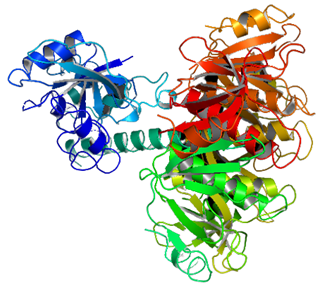
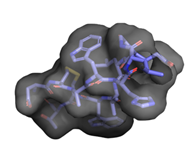
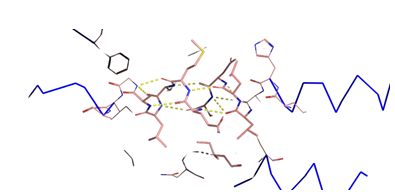
Figure17: Figure illustrates Ray Tracing.
Drug Design-III
A third nano material Drug simulation was performed to get the design for various drugs [3].
The rest of the receptor, including seven trans- membranes helices (not shown). The rest of the receptor would continue onward from the position shown as a ball.
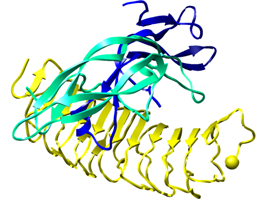
The structure mentioned includes two components: human Follicle-Stimulating Hormone (FSH) and the hormone-binding domain of the human Follicle-Stimulating Hormone Receptor (FSHR).
Human FSH: FSH is a hormone produced by the pituitary gland in the brain. It plays a crucial role in regulating reproductive functions in both males and females. FSH is composed of two subunits: an alpha chain and a beta chain. The alpha chain is common to other hormones like luteinizing hormone (LH), thyroid-stimulating hormone (TSH), and human chorionic gonadotropin (hCG). The beta chain is unique to FSH and is responsible for its specific actions.
Hormone-Binding Domain of the Human FSH Receptor (FSHR): The FSHR is a membrane-bound receptor present on the surface of target cells in the ovaries (in females) and testes (in males). The hormone-binding domain is the region of the receptor that interacts with FSH, leading to the activation of intracellular signaling pathways. The hormone- binding domain is the part of the receptor that specifically recognizes and binds FSH.
In the described structure, the FSH molecule (made up of the alpha and beta chains) is shown bound to the hormone- binding domain of the FSH receptor. This binding is essential for FSH to transmit its signals into the target cells and initiate the physiological responses necessary for reproductive functions. The “rest of the receptor” mentioned in the description refers to the remaining portion of the FSHR, which includes seven transmembrane helices. These helices are embedded in the cell membrane and play a crucial role in transmitting the signal from the hormone-binding domain to the inside of the cell. They are essential for the activation of intracellular signaling pathways that mediate the effects of FSH.
The depiction of the FSH-FSHR complex in this structure provides valuable insights into the molecular interactions that govern the function of FSH and its receptor. It helps researchers understand the mechanism by which FSH initiates its biological effects and offers opportunities for the development of novel therapies targeting reproductive disorders and fertility issues.
The “Hormone-Receptor Complex” refers to the molecular interaction between a hormone and its specific receptor on the surface of target cells. When a hormone binds to its receptor, it initiates a signaling cascade inside the cell, leading to various physiological responses.
In this context, the “hormone-binding domain” of the receptor is the specific region of the receptor that directly interacts with the hormone molecule. It is the part of the receptor that recognizes the hormone and allows it to bind with high affinity. The hormone-binding domain is crucial for the selectivity and specificity of the receptor’s response to its corresponding hormone.
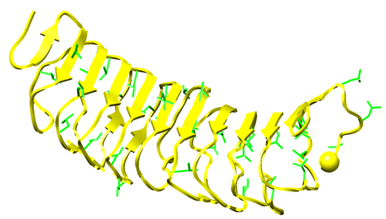
The term “leucine-rich repeats” (LRRs) refers to a structural motif found in the hormone-binding domain of certain receptors, including some hormone receptors. LRRs are short repetitive sequences of amino acids that contain leucine residues. They form a characteristic horseshoe- like structure, and their repeated arrangement creates a concave surface capable of binding to the hormone with high specificity.
The presence of leucine-rich repeats in the hormone- binding domain enhances the receptor’s ability to recognize and bind the hormone effectively. The unique shape and arrangement of LRRs create a specific binding pocket that complements the shape and properties of the hormone, allowing for a strong and specific interaction.
Overall, the presence of leucine-rich repeats in the hormone-binding domain plays a critical role in the formation of the hormone-receptor complex and ensures the receptor’s selectivity for its specific hormone. This complex interaction is fundamental for the initiation of cellular responses and the regulation of various physiological processes throughout the body. Understanding the structure and function of hormone- receptor complexes, including the role of leucine-rich repeats, is essential for unraveling the molecular basis of hormone signaling and its implications for health and disease.
Follicle-Stimulating Hormone (FSH) is a glycoprotein hormone, meaning it is a protein that contains carbohydrate (sugar) groups attached to its structure. These carbohydrate groups are covalently linked to specific amino acid residues in the FSH molecule.
In the case of FSH, the carbohydrate groups are attached to asparagine (Asn) residues. Asparagine is one of the twenty standard amino acids found in proteins. During the synthesis of FSH in the cells that produce it (e.g., pituitary gland), the protein undergoes a process called glycosylation.
Glycosylation involves the addition of carbohydrate chains to specific sites on the protein, typically at certain asparagine residues. This post-translational modification plays an important role in the structure, stability, and function of glycoproteins like FSH.
Notably, the FSH receptor, which is a protein located on the surface of target cells in the ovaries (in females) and testes (in males), also contains carbohydrate groups attached to asparagine residues. The glycosylation of the FSH receptor is important for its proper folding, trafficking to the cell surface, and interaction with FSH.
The presence of carbohydrate groups in FSH and its receptor contributes to their three-dimensional structure and enhances their stability. Additionally, glycosylation can also modulate the binding affinity between FSH and its receptor, affecting the strength and duration of the hormone- receptor interaction.
Overall, the glycoprotein nature of FSH, with carbohydrate groups attached to specific asparagine residues, is critical for its biological activity and signaling function. It allows FSH to effectively bind to its receptor, initiate intracellular signaling, and regulate various reproductive processes essential for fertility and reproduction in both males and females.
Follicle-Stimulating Hormone (FSH) is a protein hormone that plays a crucial role in regulating reproductive functions in both males and females. One of the essential features of FSH’s molecular structure is the presence of multiple disulfide bonds.
Disulfide bonds are strong covalent bonds formed between two cysteine amino acid residues in the protein chain. These bonds result from the oxidation of thiol groups (-SH) present in the cysteine side chains. The formation of disulfide bonds creates a stable linkage between two cysteine residues, contributing to the protein’s three-dimensional structure and stability.
In the case of FSH, the presence of numerous disulfide bonds helps hold the protein’s complex and folded structure together. The specific arrangement of these disulfide bonds determines the shape and conformation of FSH, which is essential for its biological activity and receptor binding.
The disulfide bonds play a critical role in maintaining the integrity of the FSH molecule during synthesis and secretion in the cells that produce it (e.g., pituitary gland). They prevent the protein from unfolding or denaturing under various physiological conditions, ensuring that FSH retains its functional structure.
The stability provided by disulfide bonds is particularly important for the proper functioning of FSH as a hormone. It enables FSH to survive the harsh conditions of the bloodstream and reach its target cells intact. Once at the target cells, FSH can interact with its specific receptor, initiating intracellular signaling pathways and regulating various processes related to reproduction, such as the maturation of follicles in the ovaries and sperm production in the testes.
In summary, the presence of multiple disulfide bonds in FSH is vital for maintaining its structural integrity and functionality as a hormone. These bonds contribute to the stability and overall shape of the protein, allowing FSH to perform its crucial role in the reproductive system.
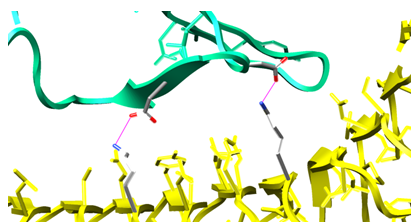
Hydrogen bonds between oppositely charged amino acid residues are commonly referred to as “salt bridges.” In the context of Follicle-Stimulating Hormone (FSH) and its receptor, specific salt bridges play a critical role in the interaction between the hormone and its receptor.
Within the FSH beta chain, two aspartic acid (Asp) residues are conserved. In the FSH receptor, two lysine (Lys) residues are also conserved. These conserved residues are found in corresponding positions across different species, indicating their importance in the function of FSH and its receptor.
The side chains of the aspartic acid residues in FSH and the lysine residues in the receptor interact through hydrogen bonding. Aspartic acid has a negatively charged side chain with a carboxyl group (COO-), and lysine has a positively charged side chain with an amino group (NH3+). The interaction between the negatively charged oxygen atom of the aspartic acid and the positively charged nitrogen atom of the lysine forms a salt bridge.
The salt bridges between the conserved aspartic acid and lysine residues in FSH and its receptor contribute to the stability of the hormone-receptor complex. They help hold the two molecules together and facilitate the specific binding of FSH to its receptor. This binding is essential for the activation of intracellular signaling pathways and the initiation of various physiological responses related to reproduction.
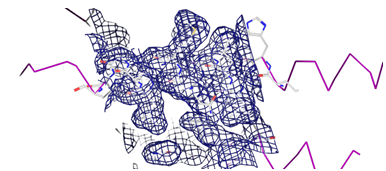
In structural representations of the FSH-FSH receptor complex, the side chains of these four conserved residues are often color-coded by element, with carbon in grey, oxygen in red, and nitrogen in blue. This color-coding allows researchers to visualize and study the molecular interactions and bond formations between these important residues.
Overall, the presence of salt bridges between conserved aspartic acid and lysine residues in FSH and its receptor is a key feature in the specific recognition and binding of FSH to its receptor, enabling the hormone to transmit its signals and regulate reproductive functions in the body.
Nanomedicine Data
| Cell label | Area | Mean fluorescence | Mean fluorescence/area | Channel |
|---|---|---|---|---|
| rs e7 cox2 317cn9 roi1.tif:0002-0031-0583:c:1/5 - rs e7 cox2 317cn9 roi1.nd2 (series 1) | 112.98 | 790.065 | 6.993272848 | dapi |
| rs e7 cox2 317cn9 roi1.tif:0002-0031-0583:c:2/5 - rs e7 cox2 317cn9 roi1.nd2 (series 1) | 112.98 | 343.745 | 3.042664306 | cd68 |
| rs e7 cox2 317cn9 roi1.tif:0002-0031-0583:c:3/5 - rs e7 cox2 317cn9 roi1.nd2 (series 1) | 112.98 | 671.599 | 5.944669175 | cox2 |
| rs e7 cox2 317cn9 roi1.tif:0002-0031-0583:c:4/5 - rs e7 cox2 317cn9 roi1.nd2 (series 1) | 112.98 | 1535.877 | 13.59483957 | nano |
| rs e7 cox2 317cn9 roi1.tif:0002-0068-0297:c:1/5 - rs e7 cox2 317cn9 roi1.nd2 (series 1) | 89.512 | 807.829 | 9.024812316 | dapi |
| rs e7 cox2 317cn9 roi1.tif:0002-0068-0297:c:2/5 - rs e7 cox2 317cn9 roi1.nd2 (series 1) | 89.512 | 277.08 | 3.095450889 | cd68 |
| rs e7 cox2 317cn9 roi1.tif:0002-0068-0297:c:3/5 - rs e7 cox2 317cn9 roi1.nd2 (series 1) | 89.512 | 532.128 | 5.944767182 | cox2 |
| rs e7 cox2 317cn9 roi1.tif:0002-0068-0297:c:4/5 - rs e7 cox2 317cn9 roi1.nd2 (series 1) | 89.512 | 1460.459 | 16.31579006 | nano |
| rs e7 cox2 317cn9 roi1.tif:0002-0069-0347:c:1/5 - rs e7 cox2 317cn9 roi1.nd2 (series 1) | 78.511 | 774.301 | 9.862325025 | dapi |
| rs e7 cox2 317cn9 roi1.tif:0002-0069-0347:c:2/5 - rs e7 cox2 317cn9 roi1.nd2 (series 1) | 78.511 | 441.828 | 5.627593586 | cd68 |
Table 1: illustrates for e7 cn rs [4].
| Cell label | Area | Mean fluoresence | Mean fluorescence/area | Channel |
|---|---|---|---|---|
| rs e7 cox2 317cd10 roi1.nd2:0002-0016-0897:c:1/5 - rs e7 cox2 317cd10 roi1.nd2 (series 1) | 40.44 | 771.276 | 19.07352177 | dapi |
| rs e7 cox2 317cd10 roi1.nd2:0002-0016-0897:c:2/5 - rs e7 cox2 317cd10 roi1.nd2 (series 1) | 40.44 | 2092.779 | 51.75406187 | cd68 |
| rs e7 cox2 317cd10 roi1.nd2:0002-0016-0897:c:3/5 - rs e7 cox2 317cd10 roi1.nd2 (series 1) | 40.44 | 538.1 | 13.30711972 | cox2 |
| rs e7 cox2 317cd10 roi1.nd2:0002-0016-0897:c:4/5 - rs e7 cox2 317cd10 roi1.nd2 (series 1) | 40.44 | 1196.506 | 29.58938596 | nano |
| rs e7 cox2 317cd10 roi1.nd2:0002-0027-0833:c:1/5 - rs e7 cox2 317cd10 roi1.nd2 (series 1) | 63.77 | 735.527 | 11.53387904 | dapi |
| rs e7 cox2 317cd10 roi1.nd2:0002-0027-0833:c:2/5 - rs e7 cox2 317cd10 roi1.nd2 (series 1) | 63.77 | 3621.257 | 56.78532562 | cd68 |
| rs e7 cox2 317cd10 roi1.nd2:0002-0027-0833:c:3/5 - rs e7 cox2 317cd10 roi1.nd2 (series 1) | 63.77 | 2593.552 | 40.66977153 | cox2 |
| rs e7 cox2 317cd10 roi1.nd2:0002-0027-0833:c:4/5 - rs e7 cox2 317cd10 roi1.nd2 (series 1) | 63.77 | 3673.642 | 57.60678051 | nano |
| rs e7 cox2 317cd10 roi1.nd2:0002-0037-0073:c:1/5 - rs e7 cox2 317cd10 roi1.nd2 (series 1) | 111.1 | 1227.357 | 11.04890893 | dapi |
| rs e7 cox2 317cd10 roi1.nd2:0002-0037-0073:c:2/5 - rs e7 cox2 317cd10 roi1.nd2 (series 1) | 111.1 | 1258.973 | 11.33352238 | cd68 |
| Cell label | Area | Mean fluoresence | Mean fluorescence/ area | Channel |
| rs ea cox2 415cn16 roi1.nd2:0002-0256-0551:c:1/4 - rs ea cox2 415cn16 roi1.nd2 (series 1) | 195.05 | 176.131 | 0.903004358 | dapi |
| rs ea cox2 415cn16 roi1.nd2:0002-0256-0551:c:2/4 - rs ea cox2 415cn16 roi1.nd2 (series 1) | 195.05 | 303.343 | 1.555206357 | cd68 |
| rs ea cox2 415cn16 roi1.nd2:0002-0256-0551:c:3/4 - rs ea cox2 415cn16 roi1.nd2 (series 1) | 195.05 | 197.244 | 1.011248398 | cox2 |
| rs ea cox2 415cn16 roi1.nd2:0002-0256-0551:c:4/4 - rs ea cox2 415cn16 roi1.nd2 (series 1) | 195.05 | 217.02 | 1.112637785 | nano |
| rs ea cox2 415cn16 roi1.nd2:0002-0265-0632:c:1/4 - rs ea cox2 415cn16 roi1.nd2 (series 1) | 133.64 | 140.737 | 1.053121118 | dapi |
| rs ea cox2 415cn16 roi1.nd2:0002-0265-0632:c:2/4 - rs ea cox2 415cn16 roi1.nd2 (series 1) | 133.64 | 230.046 | 1.721411575 | cd68 |
| rs ea cox2 415cn16 roi1.nd2:0002-0265-0632:c:3/4 - rs ea cox2 415cn16 roi1.nd2 (series 1) | 133.64 | 167.338 | 1.252173783 | cox2 |
| rs ea cox2 415cn16 roi1.nd2:0002-0265-0632:c:4/4 - rs ea cox2 415cn16 roi1.nd2 (series 1) | 133.64 | 207.962 | 1.556159176 | nano |
| rs ea cox2 415cn16 roi1.nd2:0002-0288-0551:c:1/4 - rs ea cox2 415cn16 roi1.nd2 (series 1) | 110.85 | 200.073 | 1.804898512 | dapi |
| rs ea cox2 415cn16 roi1.nd2:0002-0288-0551:c:2/4 - rs ea cox2 415cn16 roi1.nd2 (series 1) | 110.85 | 448.746 | 4.048227334 | cd68 |
Table 2: illustrates for e7 cd rs.
Results
Below are few results:
- Various COX Inhibitors are illustrated in the figures
- Illustration of flurbiprofen bound to COX-1 and COX-2 selective inhibitor SC-558 is bound to COX-2
- Various cartoon representation of Volume Rendering, Roving Detail, Roving Density, Transparency of surface, Ray Tracing, Sculpting, Molscript R3D Input are depicted.
- Sample of data is collected for e7 cn rs, e7 cd rs, ea cn rs
Conclusion
COX inhibitors, which target the enzymes cyclooxygenase-1 (COX-1) and cyclooxygenase-2 (COX-2), have proven to be valuable therapeutic agents in managing various medical conditions. These drugs exert their effects by modulating the production of prostaglandins, which play pivotal roles in inflammation, pain, and fever. The development of COX inhibitors has provided effective relief for patients suffering from inflammatory disorders, pain, and fever, significantly improving their quality of life.
Non-selective COX inhibitors, while effective in reducing inflammation and pain, come with limitations due to their potential gastrointestinal side effects. The inhibition of COX-
1-derived prostaglandins can lead to stomach irritation and ulceration, making them less ideal for patients at risk of gastrointestinal complications. In contrast, COX- 2 selective inhibitors were designed to provide targeted anti-inflammatory benefits while preserving the protective functions of COX-1 in the gastrointestinal tract. These selective inhibitors have demonstrated a favorable safety profile in terms of gastrointestinal side effects.
However, it is crucial to consider the potential risks associated with COX-2 selective inhibitors, particularly their link to increased cardiovascular events in some patients. Therefore, careful patient assessment and risk evaluation are essential when prescribing these drugs.
Recent research has shed light on the complex interplay between COX-1 and COX-2 in health and disease. Understanding the distinct roles of these enzymes in different tissues and pathologies may open up new avenues for drug development and personalized medicine, allowing for more targeted and safer anti-inflammatory therapies.
Overall, COX inhibitors have significantly contributed to the management of inflammation, pain, and fever, providing relief to countless patients worldwide. Their continued study and refinement will pave the way for the development of novel therapies and the optimization of existing treatments, ultimately improving patient outcomes in various medical conditions. As research progresses, the hope is to strike a delicate balance between the desired therapeutic effects and potential side effects, creating a new generation of COX inhibitors that offer both efficacy and safety in a wide range of clinical applications.
References
-
Soares S, Sousa J, Pais A, Vitorino C (2018) Nanomedicine: Principles, properties, and regulatory issues. Frontiers in Chemistry 6.
-
Pymol (2021) PyMOL. PyMOL.
-
Pettersen EF, Goddard TD, Huang CC, Couch GS, Greenblatt DM, et al. (2004) UCSF Chimera--a visualization system for exploratory research and analysis.. J Comput Chem 25(13): 1605-1612.
-
Muzamil S (2019) COX-2 positive macrophages at the sciatic nerve. Figshare.
- Solution-Processed Chiral Perovskites for Biomedical Applications
- Nanotechnology in Health Chemistry and Medicine: Current Challenges and Future Directions
- Human Exposure to Micro- and Nanoplastics: Pathways, Toxicity, and Intervention Strategies
- Exosome Nanomedicine for Cancer Therapy
- Micro and Nanoplastics–Plastisphere, Biotoxicity, Impact on Human Health, and Mitigation Strategies
- Process Validation of Cefixime Powder for Suspension Dosage Form, 50 mL