Comparative Safety Profile of Single Versus Combination Antipsychotic Therapy by Using Glassgow Antipsychotic Side Effect Scale (Gass)
Background: The considerable controversies exist regarding the clinical safety of first and second-generation antipsychotics and their different combinations frequently prescribed for schizophrenia and bi-polar disorders. Objective: The prime intent of the study was to compare the side effect profiles of first and second-generation antipsychotic drugs, either single or combination, in patients with schizophrenia and bipolar disorder. Methods: In this cross-sectional observational study, Glassgow Antipsychotic Side effect Scale (GASS), a validated self-assessment and self-rating scale for determining side effects of antipsychotics, was used for grading purpose. The study was conducted by enrolling a total of 252 patients. Results: Out of 252 patients, 21.83% were using first generation antipsychotics (FGAs), 44.04% were using second generation antipsychotics (SGAs) and 34.13% were using combination of the first and second generation antipsychotics. A total of 57.9% of patients suffered from mild and 42.06% patients experienced moderate side effects after using different antipsychotics. The findings indicated greater risk of side effects of antipsychotics in female gender based on GASS score (Male;18.82, Female; 22.00, p=0.014). On the other hand, demographic factors like age (p=0.185), marital status (p=0.655), education (p=0.128), family history of psychosis (p=0.496) and history of substance (p=0.736) were not significantly associated with overall side effects. However, patients doing exercise experienced fewer side effects as compared to those patients who were having sedentary life style (17.42 vs 20.51,. p=0.006). Mean GASS score was least in case of combination therapy of FGAs and SGAs which showing that antipsychotic drugs were better tolerance when used in combination (FGAs: 20.51, SGAs: 20.05, Combination: 18.12).Conclusion: This study manifested that the differences between antipsychotics were subtle, but precise and distinguishable. These findings depicted the general notion that risk of side effects significantly increased in patients on mono-therapy as compared to those who were using combination of FGA and SGA.
Introduction
Schizophreniais a cluster of different psychological disorder notable by disruptive thoughts and behaviours and characterized by hallucinations, delusions, aggression, hyperactivity and insomnia [1, 2]. Bipolar disorder is generally characterized by mood variations with frequent episodes of depression, mania and mixed state [3]. Antipsychotic drugs act either by blocking dopaminergic or serotonin receptors and are used to treat symptoms of schizophrenia and bipolar disorder [4]. Most of the newer antipsychotic agents inhibit serotonin receptor [5]. Previously disease was treated with first generation antipsychotics (FGAs) but due to potential toxicity and side effects, lately, newer class of second generation antipsychotics (SGAs) were developed with lesser side effects [6]. FGAs effect basal ganglia and cortical areas of brain whereas second generation cause enlargement of thalami [7]. Extra pyramidal side effects (EPS) include dystonia, akathisia, tardive dyskinesia and parkinson like symptoms which may lead to therapy related problems resulting in noncompliance among patients [8, 9]. Antipsychotics-induced weight gain, endocrine imbalance and hyperlipidemia which may lead to diabetes mellitus, hyperprolactinemia, hypertension, orthostatic hypotension, coronary artery disease, seizures and stroke [10, 11]. Newer SGAs have better control over negative symptoms [12] and extra pyramidal side effects along with more efficacious response to the delusions and hallucinations in those patients who don’t reciprocate to other antipsychotics [13]. Nonetheless, the newer second generations are more likely to cause metabolic side effects [14]. Older conventional FGA which bind very tightly to dopaminergic receptors have more pronounced side effects linking with movement disorder, like haloperidol, as compared to those drugs that form weak bonds with dopaminergic receptors like Chlorpromazine [15]. Some of SGA have added side effects when compared with the rest of the class, therefore, in selecting the drug, physician should keep in mind treatment related disease symptoms together with efficacy [16]. Among these, olanzapineis most notorious because of its side effects, such as weight gain and increment of blood glucose levels [17]. Polypharmacy of antipsychotic drugs in schizophrenia and bipolar disorder is being most commonly practiced from past many years [18]. Combination of first and second generation antipsychotics is comparatively condescending upon monotherapy in critically ill patients, however significant evidence regarding effectiveness of combination therapy is not present in literature and further clinical trials are needed in this respect [18, 19]. The basic proposed working hypothesis of this study was to prove that monotherapy has rather more severe adverse effects as compared to combination of first and second generation antipsychotics. Therefore, we had done this observational study to compare the side effect profile of mono versus combination antipsychotic therapy among schizophrenic and bipolar disorder patients in Punjab Institute of Mental Health (PIMH) and Fountain House Lahore, Pakistan.
Methodology
A cross sectional observational study was designed to assess the side effects of antipsychotics in schizophrenia and bipolar patients presenting to two major hospitals of Lahore including Punjab Institute of Mental health and Fountain House. Ethical approval for the study was obtained from Ethical committee on human research, University of the Punjab and medical directors of both the hospitals. Selection criteria were majorly inclusive and were least exclusive. A total of 252 patients, willing to give their information and stable on medication for the last one year irrespective of age, gender, education and ethnic background, were enrolled in the study. Diagnosis of patients was being done by qualified physicians of both hospitals based on DSM-IV-TR (Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition Text Revision).Manual describes the diagnostic criteria for this disease which states that ailment is present if pertinacious dysfunction persist longer than 6 months and more than two symptoms like delusions, hallucination and negative symptoms exists for at least the month [20]. Patients with epilepsy and concomitant disease of other organs were excluded from the study. A group of six final professional Pharm.D graduates collected the data, having thorough knowledge of the disease. Informed consent was obtained from all the enrolees as per hospital policy. In this study Glassgow Antipsychotic Side effect Scale (GASS), a validated self-assessment and self-rating scale for determining side effects of antipsychotics, was used for grading purpose. Total GASS scoring from 0-21 indicates mild side effects, 22-42 indicates moderate side effects and 43 or more than this indicates severe side effects. There are several antipsychotic side effect rating scales that were used previously, majority of them are extensive, time taking and focussing on merely akathisia or extra pyramidal side effects [21]. It is relatively new, convenient, handy, time saving and patient friendly scale that is covering all aspects. A comprehensive questionnaire along with the 22 items GASS, fulfilling the project needs and objectives was prepared.
Data and Statistical Analysis
The data was analysed using the SPSS software (IBM, version 22) to estimate the side effects of first generation, second generation and their combination. Descriptive statistics was performed using SPSS. Chi square test was applied for nominal data, kruskal-wallis for ordinal data and independent sample t-test and analysis of variance (ANOVA) for continuous data. A p-value less than 0.05 was considered significant.
Results
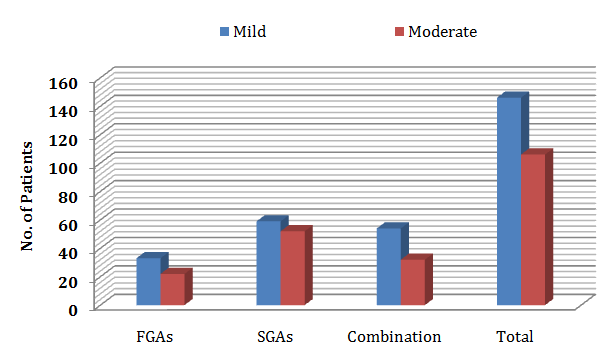
As per the data, out of 252 patients, 21.83% were using FGA, 44.04% were using SGA and 34.13% were using combination, both first and second-generation.
Patient Demographics and Clinical Characteristics
Patient demographics and clinical characteristics are summarized in (Table 1). The occurrence of schizophrenia was more frequent in males as per antipsychotic usage (FGAs; 76.4%, SGAs; 82.9%, Combination; 75.5%) compared to females, and more likely to affect unmarried (FGAs; 63.6%, SGAs; 63.1%, Combination; 52.3%). Out of total 252 patients, 70.9%educated people were on different types of antipsychotics (p=0.604). Overall 45.3% patients were unemployed taking combination treatments (p=0.496). Moreover, 67.4% patients that were on combination drugs didn’t have any of the psychiatric diseases in their families including blood relations i.e. in their parents, grandparents and siblings. This study also revealed that 58.2% patients taking first generation antipsychotics were not addicts, while 76.6% people taking combination of neuroleptics were normotensive before starting antipsychotics. A total of 56 patients out of 252 patients were diagnosed with bipolar disorder and among them 20.9% were on combination of Antipsychotics along with other medications.
| Parameters | FGAs | SGAs | Combination | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| (n=55) | (n=111) | (n=86) | |||||||||
| Gender __no. (%) Male Female | 42 (76.4%) 13 (23.6%) | 92 (82.9%) 19 (17.1%) | 65 (75.5%) 21 (24.4%) | ||||||||
| Marital Status__no. (%) | 20(36.4%) 35(63.6%) | 41(36.9%) 70(63.1% ) | 41(47.7%) 45(52.3%) | ||||||||
| Married | |||||||||||
| Single | |||||||||||
| Education__no. (%) Educated Uneducated | 36(65.5%) 19(34.5%) | 81(73%) 30(27%) | 61(70.9%) 25(29.1%) | ||||||||
| Occupation__no. (%) | 2(3.6%) 8(14.5%) 19(34.5%) 26(47.3%) | 2(1.8%) 23(20.7%) 44(39.6%) 42(37.8%) | 0 (0%) 13(15.1%) 34(39.5%) 39(45.3%) | ||||||||
| Govt.job | |||||||||||
| Private | |||||||||||
| Self | |||||||||||
| Unemployed | |||||||||||
| Family history_no. (%) No Yes | 31(56%) 24(43.6%) | 70(63.1%) 41(36.9%) | 58(67.4%) 28(32.6%) | ||||||||
| Drugabuse_no. (%) | 32(58.2%) | 53(47.7%) | 42(48.8%) | ||||||||
| Non Abusers |
Table 1: Patient Demographics, Personal Information and Clinical Presentation.
| Abusers | 23(41.8%) | 58(52.3%) | 44(51.2%) | ||
|---|---|---|---|---|---|
| Exercise_no. (%) Yes No | 15(27.3%) 40(72.7%) | 41(36.9%) 70(63.1%) | 27(31.4%) 59(68.6%) | ||
| Blood Pressure_no. (%) | 47(85.5%) 8(14.5%) | 94(84.7%) 17(15.3%) | 66(76.7%) 20(23.3%) | ||
| Normotensive | |||||
| Hypertensive | |||||
| Diagnose no. (%) Schizophrenia Bipolar Disorder | 48(87.27%) 7(12.72%) | 80(72.07%) 31(20.12%) | 68(79.07%) 18(20.9%) |
Table 2: Patient Demographics, Personal Information and Clinical Presentation.
Grading of Side Effects of Antipsychotic Drugs Based on GASS
The frequencies of side effects in all three arms, FGAs, SGAs and combinations, are summarized in (Table 2 & Figure 1). When data was segregated based on mild and moderate side effects as per GASS criteria, in FGAs group, fluphenazine exhibited higher frequencies of side effects, mild (42.4%) and moderate (36.4%), followed by flupentixol (mild; 24.3%, moderate; 31.8%) and haloperidol (mild; 18.2%, moderate; 27.3%) (Table 2). When SGAs group was examined for side effects,
| Drugs | Mild Side Effec | t | Moderate Side Effects | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| FGAs | |||||||||||
| Haloperidol_no. (%) | 6/33(18.2%) | 6/22(27.3%) | 12/55(21.8%) | ||||||||
| Fluphenazine_no. (%) | 14/33(42.4%) | 8/22(36.4%) | 22/55(40%) | ||||||||
| Flupentixol_no. (%) | 8/33(24.3%) | 7/22(31.8%) | 15/55(27.3%) | ||||||||
| Trifluroperazine_no. (%) | 3/33(9.1%) | 1/22(4.5%) | 4/55(7.3%) | ||||||||
| Zuclopenthixoldihydrochloride_no. (%) | 2/33 (6.1%) | 0 | 2/55(3.6%) | ||||||||
| SGAs | |||||||||||
| Risperidone_no. (%) | 40/59(67.8%) | 39/52(75%) | 7 | 9/111(71.2% | ) | ||||||
| Olanzapine_no. (%) | 10/59(20.4%) | 7/52(13.4%) | 1 | 7/111(15.3% | ) | ||||||
| Quetiapine_no. (%) | 4/59(6.8%) | 5/52(9.6%) | 9/111(8.1%) | ||||||||
| Clozapine_no. (%) | 2/59(3.4%) | 1/52(1.9%) | 3/111(2.7%) | ||||||||
| Aripiprazole_no. (%) | 3/59(1.7%) | 0 | 3/111(2.7%) | ||||||||
| Combination of FGAs & SGAs | |||||||||||
| Risperidone+ Fluphenazine_no. (%) | 36/54(66.7%) | 16/32(50%) | 52/86(60.5%) | ||||||||
| Fluphenazine+ Olanzapine_no. (%) | 1/54(1.9%) | 3/32(9.4%) | 4/86(4.7%) | ||||||||
| Risperidone +quetiapine+ Flupentixol_no. (%) | 1/54(1.9%) | 2/32(6.3%) | 3/86(3.5%) | ||||||||
| Olanzapine+ Risperidone+ Fluphenazine_no. (%) | 2/54(3.7%) | 0 | 2/86(2.3%) | ||||||||
| Risperidone+ quetiapine+ Fluphenazine_no. (%) | 1/54(1.9%) | 0 | 1/86(1.2%) | ||||||||
| Risperidone+ Zuclopenthixol_no. (%) | 1/54(1.9%) | 1/32(3.1%) | 2/86(2.3%) | ||||||||
| Risperidone + Flupentixol_no. (%) | 2/54(3.7%) | 2/32(6.3%) | 4/86(4.7%) | ||||||||
| Haloperidol+ quetiapine_no. (%) | 1/54(1.9%) | 0 | 1/86(1.2%) | ||||||||
| Fluphenazine+ haloperidol+ Olanzapine_no. (%) | 1/54(1.9%) | 3/32(9.4%) | 4/86(4.7%) | ||||||||
| Fluphenazine+ Risperidone +zuclopenthixol_no. (%) | 1/54(1.9%) | 1/32(3.1%) | 2/86(2.3%) | ||||||||
| Risperidone + haloperidol_no. (%) | 7/54(13%) | 4/32(12.5%) | 11/86(12.8%) |
Table 3: Side Effects of Fgas, Sgas and Combinations Based on Gass.
- Parameters
- No. (%)
- Mean±S.D p-value
- Gender
- 199 (78.9%)
- 18.82±8.19
- 22.00±8.61
- Male
- Female
- 0.014*
- 53 (21%)
- Age
- <30
- >30
- 116(46.03%)
- 136(53.97%)
- 20.25±8.20
- 18.84±8.42
- 0.185
- Marital Status
- 102(40.5%)
- 150(59.5%)
- 19.21±8.28
- 19.69±8.44
- Discussion
- Married
- Unmarried
- 0.655
- Education
- 178(70.6%)
- 19.07±8.25
- 20.50±8.61
- Educated
- Uneducated
- 0.218
- 74(29.4%)
- Family history
- 159(63.1%)
- 19.77±8.71
- 19.02±7.77
- No
- Yes
- 0.496
- 93(36.9%)
- Substance abuse
- 127(50.4%)
- 125(49.6%)
- 19.31±8.74
- 19.67±7.80
- Non Abusers
- 0.736
- Abusers
- Exercise
- 83(32.9%)
- 169(67.1%)
- 17.42±8.97
- 20.51±7.88
- Yes
- 0.006*
- No
- Blood Pressure
- 207(82.1%)
- 19.25±8.21
- 20.62±9.08
- Normotensive
- 0.318
- Hypertensive
- 45(17.9%)
- Type of
- Antipsychotic Drug
- 55(21.8%)
- 111(44.1%)
- 20.51±9.34
- 20.05±7.93
- 17.45±7.28
- 0.036*
- FGA
- SGA
- Combination
- 86(34.1%)
Table 4: GASS score classified by demographic and clinical
GASS Score Classified by Demographic Characteristics
As shown in table 3, gender was found to be more significantly associated with GASS score. The finding indicated that females were having higher GASS score as compared to male patients which was indicating greater risk of side effects of antipsychotics in female gender. As shown in (Table 3), mean GASS score for male and female gender were 18.82 and 22.00 respectively (p=0.014). On the other hand, demographic factors like age (p=0.185), marital status (p=0.655), education (p=0.128), family history of mental illnesses (p=0494) and history of drug substance abuse (p=0.736) were not significantly associated with overall GASS score. However, patients doing exercise experienced fewer side effects as compared to those patients who were having sedentary life style (17.42 vs 20.51p<0.05 i.e. p=0.006). On the whole, there was non-significant association among the type of antipsychotic drugs and GASS. However, mean GASS score was least in case of combination therapy of FGAs and SGAs which showing that antipsychotic drugs were better tolerance when used in combination (FGAs: 20.51, SGAs: 20.05, Combination: 17.45).
There are numerous antipsychotic side effect rating scales that were used previously like Simpson-Angus Scale (SAS), Barnes Akathisia Scale, Abnormal Involuntary Movement Scale (AIMS), Extrapyramidal Side Effect Rating Scale (ESRS), Antipsychotic Non-Neurological Side- effect Rating Scale (ANNSERS), Liverpool University Neuroleptic Side-Effect Rating Scale (LUNSERS) and many others [22]. In this study, a new self-assessment Glassgow Antipsychotic Side Effect Scale (GASS) was used which was relatively easy, time saving, patient friendly and covers all side effects including metabolic along with extra pyramidal side effects. Several assessment scales have certain advantages and disadvantages like Simpson Angus Scale and Extra pyramidal Side Effect Rating Scale were rather easy to conduct but solely used for determination of extra pyramidal side effects. Barnes Akathisia Rating Scale and Hillside Akathisia Scale only concentrate on Akathisia. Liverpool University Neuroleptic Side Effect Rating Scale covers many areas of side effects but it is slightly lengthy and symptoms can only to be described in single word that is quite arduous for patients suffering from mental illness. Another Abnormal Involuntary Movement Scale is used that is quick to perform but only considering on abnormal movements. Side Effects Rating
| [27]. Antipsychotics | -induced acute Extra Pyramidal side- | ||
|---|---|---|---|
| effects are more visible in patients having Bipolar | |||
| Disorder as compared to Schizophrenic patients when in | |||
| depressive state. Atypical antipsychotics are least | |||
| markedly to produce acute Extra Pyramidal side-effects in | |||
| Bipolar Disorder as compared to typical antipsychotics, | |||
| although every antipsychotic has a distinctive burden | |||
| [28] | . | This study showed that SGAs caused more weight |
sleep related breathing disorder and night eating syndrome was due to use of both FGAs and SGAs [35]. Studies also demonstrated that SGAs significantly increases stage 2 sleep and total sleep time, whereas FGAs significantly decreases the stage 2 sleep latency but enhances the sleep efficacy [36]. According to another data, second generation aripiprazole caused minimum side effects in comparison to first generation haloperidol [37]. There was no significance difference in the side effect profile of all first and second generation drugs in the response of remaining questions of GASS in this study. When the GASS score was classified by treatment arms, there was significant reduced risk of side effects in combination therapy as compared to monotherapies of FGAs and SGAs. Data obtained from this study suggested that there was prominent reduction in the frequency of mild and moderate adverse events when risperidone combined with fluphenazine. A meta-analysis of randomized controlled trails has suggested that co- treatment of different classes of antipsychotics are far better than the monotherapy [19]. However, likelihood of getting benefit out of this augmentation with co treatment is still controversial [38, 39, 40]. Patients clinical characteristics play a pivotal role in making decision to start with either monotherapy or co-treatment with FGA and SGA [41]. A paucity of data also highlighted that discontinuing one of two drugs from combination therapy was followed by more quickly and more often treatment discontinuation owing to non-adherence [42]. According to another meta-analysis, patients who have partially responded to clozapine get benefit after adding another antipsychotic [43].
Limitation of study
The only limitation observed during study was that few questions related to sex life were not replied by patients properly due to sociocultural perspectives of region. So most of the patients replied “Never” in few questions of questionnaire or didn’t respond entirely.
Conclusion
This study manifested that the differences between antipsychotics were subtle, but precise and distinguishable. According to the GASS scoring, risk of side effects significantly increased in patients on monotherapy as compared to those who were using combination of FGA and SGA. Funding: There is no funding source for this study.
Conflict of Interest: There is no conflict of interest among authors.
References
-
Frith CD (2015) The Cognitive Neuropsychology of Schizophrenia (Classic Edition). Psychology Press.
-
Tsuang MT, Faraone SV, Glatt SJ Schizophrenia (2011): Oxford University Press.
-
Sajatovic M (2005) Bipolar disorder: disease burden. Am J Manag Care 11(3): 80-84.
-
Geddes JR, Miklowitz DJ (2013) Treatment of bipolar disorder. The Lancet 381(9878): 1672-1682.
-
Spina E, de Leon J (2014) Clinically relevant interactions between newer antidepressants and second-generation antipsychotics. Expert Opin Drug Metab Toxicol 10(5): 721-746.
-
Dolder CR (2008) Side effects of antipsychotics. Clinical handbook of schizophrenia: 168.
-
Dazzan P, Morgan KD, Orr K, Hutchinson G, Chitnis X, et al. (2005) Different effects of typical and atypical antipsychotics on grey matter in first episode psychosis: the AESOP study. Neuropsychopharmacology 30(4): 765-774.
-
Rummel Kluge C, Komossa K, Schwarz S, Hunger H, Schmid F, et al. (2012) Second-generation antipsychotic drugs and extra pyramidal side effects: a systematic review and meta-analysis of head-to- head comparisons. Schizophr Bull 38(1): 167-177.
-
Peluso MJ, Lewis SW, Barnes TR, Jones PB (2012) Extra pyramidal motor side-effects of first-and second-generation antipsychotic drugs. The British Journal of Psychiatry 200(5): 387-392.
-
Choong E, Bondolfi G, Etter M, Jermann F, Aubry JM, et al. (2012) Psychotropic drug-induced weight gain and other metabolic complications in a Swiss psychiatric population. J psychiatr Res 46(4): 540-548.
-
De Hert M, Detraux J, van Winkel R, Yu W, Correll CU (2012) Metabolic and cardiovascular adverse effects associated with antipsychotic drugs. Nat Rev Endocrinol 8(2): 114-126.
-
Kane JM, Freeman HL (1994) Towards more effective antipsychotic treatment. Br J Psychiatr Suppl (25): 22-31.
-
Meltzer HY (2004) What’s atypical about atypical antipsychotic drugs? Curr Opin Pharmacol 4(1): 53- 57.
-
De Hert M, Dobbelaere M, Sheridan EM, Cohen D, Correll CU (2001) Metabolic and endocrine adverse effects of second-generation antipsychotics in children and adolescents: a systematic review of randomized, placebo controlled trials and guidelines for clinical practice. Eur Psychiatr 26(3): 144-158.
-
John Muench M (2010) Oregon Health & Science University, Portland, Oregon, Oregon State University College of Pharmacy, Corvallis, Oregon, Adverse Effects of Antipsychotic Medications.
-
Rummel Kluge C, Komossa K, Schwarzs, Hunger H, Schmid F, et al. (2010) Head-to-head comparisons of metabolic side effects of second generation antipsychotics in the treatment of schizophrenia: a systematic review and meta-analysis. Schizophr Res 123(2-3): 225-233.
-
Lieberman JA, Stroup TS, McEvoy JP, Swartz MS, Rosenheck RA, et al. (2005) Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 353(12): 1209-1223.
-
Gallego JA, Bonetti J, Zhang J, Kans MJ, Correll CU (2012) Prevalence and correlates of antipsychotic polypharmacy: a systematic review and meta- regression of global and regional trends from the 1970s to 2009. Schizophr Res 138(1): 18-28.
-
Correll CU, Rummel Kluqe C, Corves C, Kane JM, Leucht S, et al. (2009) Antipsychotic combinations vs monotherapy in schizophrenia: a meta-analysis of randomized controlled trials. Schizophr Bull 35(2): 443-457.
-
Edition F (1980) Diagnostic and statistical manual of mental disorders.
-
Waddell L, Taylor M (2008) A new self-rating scale for detecting atypical or second-generation antipsychotic side effects. J Psychopharmacol 22(3): 238-243.
-
van Strien AM, Keijsers CJ, Derijks HJ, van Marum RJ (2015) Rating scales to measure side effects of antipsychotic medication: A systematic review. J Psychopharmacol 29(8): 857-866.
-
Jeste DV, Rockwell E, Harris MJ, Lohr JB, Lacro J (1999) Conventional vs. newer antipsychotics in elderly patients. Am J Geriatr Psychiatr 7(1): 70-76.
-
Glazer W (1999) Extra pyramidal side effects, tardive dyskinesia, and the concept of atypicality. J Clin Psychiatr 61(3): 16-21.
-
Leucht S, Pitschel Walz G, Abraham D, Kissling W (1999) Efficacy and extrapyramidal side-effects of the new antipsychotics olanzapine, quetiapine, risperidone, and sertindole compared to conventional antipsychotics and placebo. A meta-analysis of randomized controlled trials. Schizophr Res 35(1): 51-68.
-
Simpson GM, Lindenmayer JP (1997) Extrapyramidal symptoms in patients treated with risperidone. J Clin Psychopharmacol 17(3): 194-201.
-
Miller DD, Caroff SN, Davis SM, Rosenheck RA, McEvoy JP, et al. (2008) Extrapyramidal side-effects of antipsychotics in a randomised trial. Br J Psychiatr 193(4): 279-288.
-
Gao K, Kemp DE, Ganocy SJ, GajwaniP, Xia G, et al. (2008) Antipsychotic-induced extrapyramidal side effects in bipolar disorder and schizophrenia: a systematic review. J Clin Psychopharmacol 28(2): 203-209.
-
Taylor D, McAskill R (2000) Atypical antipsychotics and weightgain-a systematic review. Acta Psychiatrica Scandinavica 101(6): 416-432.
-
Nasrallah H (2003) A review of the effect of atypical antipsychotics on weight. Psychoneuroendocrinology 28(1): 83-96.
-
Domecq JP, Prutsky G, Leppin A, Sonbol MB, Altayar O, et al. (2015) Clinical review: Drugs commonly associated with weight change: a systematic review and meta-analysis. J Clin Endocrinol Metab 100(2): 363-370.
-
Meyer JM, Koro CE (2004) The effects of antipsychotic therapy on serum lipids: a comprehensive review. Schizophr Res 70(1): 1-17.
-
Ray WA, Chung CP, Murray KT, Hall K, Stein CM (2009) Atypical Antipsychotic Drugs and the Risk of Sudden Cardiac Death. N Engl J Med 360(3): 225-235.
-
Hennekens CH, Hennekens AR, Hollar D, Casey DE (2005) Schizophrenia and increased risks of cardiovascular disease. Am Heart J 150(6): 1115- 1121.
-
Cohrs S (2008) Sleep disturbances in patients with schizophrenia. CNS drugs 22(11): 939-962.
-
Monti JM, Monti D (2004) Sleep in schizophrenia patients and the effects of antipsychotic drugs. Sleep medicine reviews 8(2): 133-148.
-
Kane JM, Carson WH, Saha AR, McQuade RD, Ingenito GG, et al. (2002) Efficacy and safety of aripiprazole and haloperidol versus placebo in patients with schizophrenia and schizoaffective disorder. J Clin Psychiatr 63(9): 763-771.
-
Freudenreich O, Goff DC (2002) Antipsychotic combination therapy in schizophrenia. A review of efficacy and risks of current combinations. Acta Psychiatr Scand 106(5): 323-330.
-
Miller AL, Craig CS (2002) Combination antipsychotics: Pros, cons and questions. Schizophr Bull 28(1): 105-109.
-
Fleischhacker WW, Uchida H (2014) Critical review of antipsychotic polypharmacy in the treatment of schizophrenia. Int J Neuropsychopharmacol 17(7): 1083-1093.
-
Grande I, Vieta E (2015) Pharmacotherapy of acute mania: monotherapy or combination therapy with mood stabilizers and antipsychotics? CNS drugs 29(3): 221-227.
-
Essock SM, Schooler NR, Stroup TS, McEvoy JP, Rojas I, et al. (2011) Effectiveness of switching from antipsychotic poly pharmacy to monotherapy. American Journal of Psychiatry 168(7): 702-708.
-
Paton C, Whittington C, Barnes TR (2007) Augmentation with a second antipsychotic in patients with schizophrenia who partially respond to clozapine: a meta-analysis. J Clin Psychopharmacol 27(2): 198-204.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury