Case Report: Temporal Lobe Epilepsy Presenting as Psychiatric Illness
Psychiatric symptoms can masquerade temporal lobe epilepsy and can pose diagnostic dilemma. Chronic Lymphocytic Leukemia(CLL) as any other malignancy can cause radiologically evident or occult limbicparaneoplastic encephalitis leading to temporal seizures. Identifying known antibody in serum or CSF is not a requirement for diagnosis. Here we report a rare case of temporal lobe epilepsy from possible limbic paraneoplastic encephalitis in a patient with known CLL. A low index of suspicion and early aggressive treatment is key to improved out comes. Rarity of such cases makes impossible to conduct large scale studies.
Introduction
Limbic encephalitis is a rapidly developing neuropsychiatric illness characterized by irritability, depression, sleep disturbances, recurrent seizures, hallucinations, and/or memory loss. The clinical manifestations of limbic encephalitis are myriad and clinical picture is often confusing. Delay in diagnosisis common and could potentially be missed if the index of suspicion is not kept low. Here, we report an interesting and unusual case of chronic lymphocytic leukemia (B- CLL), presenting with mixture of unexplained rapid onset neurologic and neuropsychiatric symptoms concerning for seizures from possible limbic encephalitis.
Case
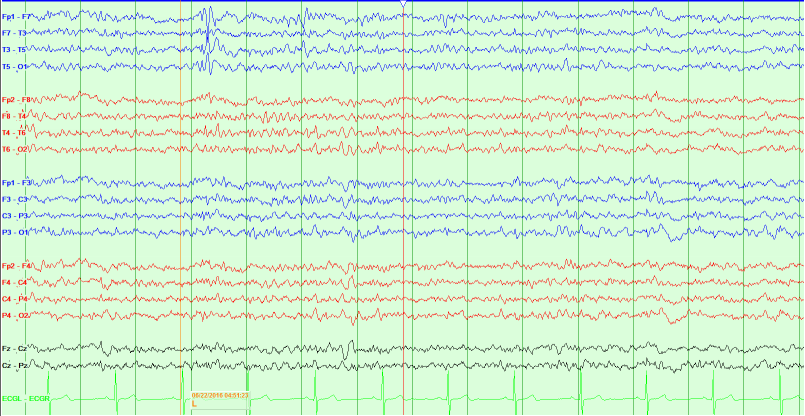
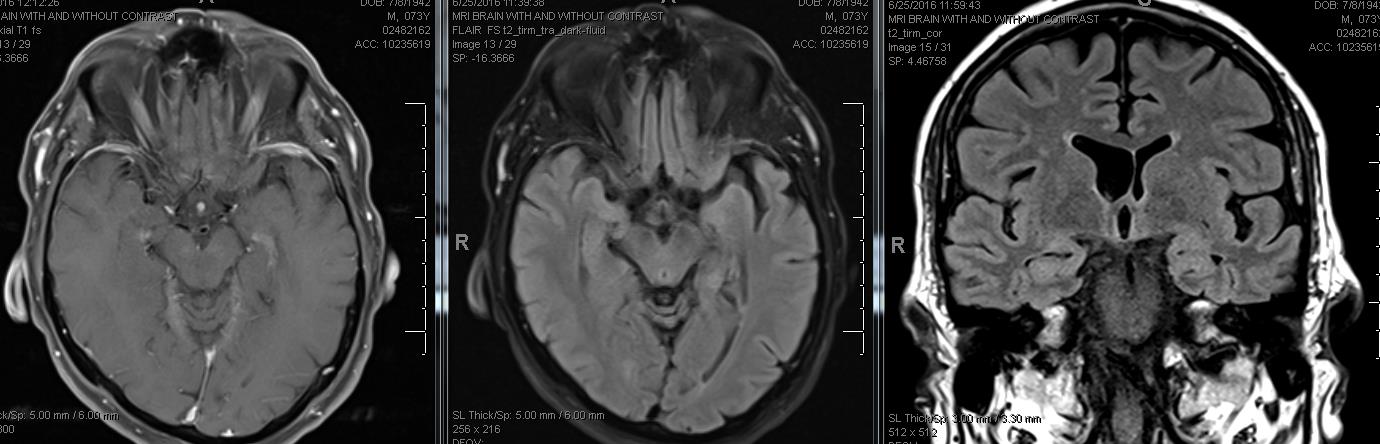
73-year-old left-handed Caucasian man with history significant for CLL in remission for 10 years, diabetes, hyperlipidemia, was visiting with his friends this area and presented with chief complaint of acute psychotic episode.He states that this all started about 2 months ago insidious in onset but progressively becoming frequent Deja vu like symptoms. He would describe his most intense episode at the airport during a layover. He saw a group of orthopedic surgeons and they were talking about the conference and patient felt that he saw them before discussing the same things in the past (experience of familiarity of personnel and situation).The sensation lasted for a few minutes and then it cleared up.Since then he has been having paranoid delusions as if everybody around him is making a conspiracy to execute him.At the local hospital, his preliminary blood work and urine studies were negative for any infection.He was given treatment for acute psychosis with Haloperidol and lorazepam and then transferred to our hospital. He had an MRI of the brain (without contrast) done at the outside hospital which showed a small left cerebellar old chronic lacunar infarct with encephalomalacia, but no acute lesions. At the time of admission to our hospital, his neurological exam was within normal limits. Further work up included Magnetic Resonance Imaging (MRI) brain with contrast which did not show any enhancing lesion, repeat blood work including toxicology screen, paraneoplastic and encephalitis panel (including ANNA -1, ANNA-2, ANNA-3, AGNA-1, PCA-1, PCA-2, PCA- Tr, Amphiphysin, CRMP-5- IgG) sent to Mayo clinic, came back within normal limits. During the hospitalization he had recurrence of paranoid delusional episodes requiring administration of typical antipsychotic medications and benzodiazepines with quick resolution of symptoms. Electroencephalogram (EEG) showed left temporal sharp waves indicative of a tendency to have seizures from that region. Lumbar puncture was performedwhich showed normal CSF analysis except for elevated protein to 92.Viral studies were all reported to be negative. He was empirically treated with Intravenous Immunoglobulin (IVIG) 2 gram/kilograms divided over three days for presumed autoimmune etiology. He was started on Lacosamide at 100 mg twice daily and repeat electroencephalogram in 48 hours showed resolution of left temporal lobe sharp waves. He improved significantly with no more déjà vu episodes with the initiation of anti- epileptic medication and after IVIG treatment. He was discharged to home in a stable medical and neurological condition.
Discussion
Epilepsy or seizures could be first manifestation of paraneoplastic process [1]. Antibodies responsible for autoimmune or paraneoplastic phenomenon can be against the surface antigens or ion channels and related complex proteins [1]. About 17 % cases of epilepsy are secondary to immune mediated phenomenon [1]. Limbic encephalitis is a well-known infective, autoimmune or paraneoplastic inflammatory disease of the central nervous system presenting with atypical neurologic symptoms including amnestic disturbances, hallucinations, and seizures as well as behavioral symptoms like depressed mood, paranoid thoughts, changes in personality and acute delirium [2]. Several paraneoplastic antibodies related to different malignancies have been described in the literature as possible pathogenesis of limbic encephalitis. It is often associated with small cell lung cancer, testicular cancer, breast cancer, or Hodgkin’s lymphoma [2]. In our case despite extensive diagnostic work up, no underlying etiology was identified. As its well understood that lack of antibody or primary malignancy detection does not rule out paraneoplastic etiology [1]. The only supportive evidence was lymphocytic pleocytosis on the CSF and the sharp wave discharges on the EEG from the left temporal lobe without any underlying structural pathology on imaging. He significantly improved with antiepileptic medication (Lacosamide) and IVIG treatment. Cerebral or meningeal involvement is a very rare event in CLL. Clinical presentations of acute delirium, meningitis, optic nerve and cerebellar involvement have been sporadically reported in the literature [2]. Neither of these was present in our patient. Progressive multifocal leukoencephalopathy has also been well described in hematological malignancies which potentially could present in a similar way but negative imaging and response to therapy makes it very unlikely in this scenario. The clinical manifestations of limbic encephalitis are myriad and clinical picture is often confusing. Delay in diagnosisis common and could potentially be missed if the index of suspicion is not kept low. It is a disorder that isusuallypresent in association with malignancies but in some cases it has been describedin cancer free patients. It has been associated with antibodies against intracellular neuronal antigens (e.g., Anti-Ma2 (Anti Ta), Anti-Hu, Anti- Yo, and CV2/CRMP5) or against cell membrane antigens (e.g., voltage-gated potassium channel, VGKC; N-methyl- Daspartate receptors, NMDAR) [1, 2]. Approximately 40% of cases are without known antibodies detected, hence their absence does not rule out the diagnosis [2]. Radiologically on MRI FLAIR or T2 unilateral or bilateral temporal lobe hyper intensity is present in acute and active disease with hippocampal and temporal lobe atrophy in longstanding cases. It is not uncommon to have patients with a syndrome typical of limbic encephalitis have normal MRI studies. Similarly in our case, MRI showed no specific signs of limbic encephalitis. Our patient improved markedly after the initiation of treatment with IVIG and anti-epileptic medications. In the light of the severe, rapidly progressive deterioration of the patient’s neuro-psychiatric condition until initiation of immune-modulation, we strongly suspect a therapeutic effect of IVIG rather than spontaneous improvement. The mechanism of action remains unknown. Although we cannot completely exclude with certainty for any unidentified viral infection presenting in our patient but the rapid improvement in the clinical course with near resolution with immunotherapy without administration of any anti-viral medications is highly suggestive of inflammatory/paraneoplastic process in the setting of chronic lymphocytic leukemia in remission. Our patient would follow with his home town oncologist regarding any need for further investigation such as bone marrow biopsy to investigate any recurrence in his primary malignancy. With our case we propose that CLL should be included in the list of malignancies possibly related to paraneoplastic limbic encephalitis. We also suggest low index of suspicion is necessary as the symptoms could be easily mistaken for pure psychiatric illness. A number of cases with limbic encephalitis get first admitted to a psych facility before getting diagnosed and treated for primary condition [3] (Figures 1 & 2).
References
-
Serafini A, Lukas RV, VanHaerents S, Warnke P, Tao JX, et al. (2016) Paraneoplastic epilepsy. Epilepsy Behav 61: 51-58.
-
Nogai H, Israel-Willner H, Zschenderlein R, Pezzutto A (2013) Improvement of paraneoplastic limbic encephalitis after systemic treatment with rituximab in a patient with B-cell chronic lymphocytic leukemia. Case Rep Hematol 2013: 958704.
-
Bost C, Pascual O, Honnorat J (2016) Autoimmune encephalitis in psychiatric institutions: current perspectives. Neuropsychiatr Dis Treat 12: 2775- 2787.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury