An Unwonted Cause of Acute Cerebellar Ataxia in a Young Lady: A Rare Path to Lupus
Neuropsychiatric manifestations are commonly observed in systemic lupus erythematosus (SLE) patients. In particular, neurological involvement is known to be more common in patients with positive anticardiolipin antibodies and lupus anticoagulants. Nevertheless, cerebellar ataxia has rarely been reported, especially as the first clinical manifestation of neuropsychiatric systemic lupus erythematosus (NPSLE). Cerebral vascular infarction or ischemia, vasogenic oedema and antibody-mediated cerebral vasculopathy or vasculitic process have been supposed as possible aetiologies of acute cerebellar ataxia related to SLE. We report the clinical and radiological features of a 38 years old diabetic lady who developed a rapidly progressive cerebellar syndrome as first sign of SLE; no other cause explaining her cerebellar ataxia was found. Imaging of brain in this patient revealed prominent cerebellar atrophy. She was treated with initial pulse intravenous methylprednisolone later oral prednisolone and oral mycophenolate mofetil. There was no further progression of her neurological signs after the initiation of therapy. The appearance of a cerebellar syndrome with unknown aetiology with associated features of possible systemic autoimmune dysfunction, should be taken into account in clinical practice for appropriate diagnostic workup in order to provide effective therapeutic options.
Introduction
Neuropsychiatric manifestations are present in 50- 70% of the patients with systemic lupus erythematosus (SLE) and include a wide variety of central and peripheral neurological manifestations [1]. Cerebellar ataxia is one of the less described neurological manifestations of systemic lupus erythematosus (SLE). Its prevalence in SLE has been estimated to occur in less than 2% of the cases, even more uncommon as the first clinical manifestation of such autoimmune systemic condition [2, 3, 4]. Several possible aetiologies of acute cerebellar syndrome related to SLE have been postulated, including cerebral infarction or ischemia, antibody-mediated dysfunctions and vasculopathy or vasculitis. Most of the patients present with acute to subacute onset cerebellar syndromes. Some of them were seen to have vasculitic infarcts in cerebellum on magnetic resonance imaging (MRI). However, the presence of cerebellar atrophy at the outset is even rarer [3]. Volume loss of cerebellum cannot be traced to the known pathogenic mechanisms of lupus. Although auto antibodies are present in such patients, there is no specific pattern attributing to the condition.
Anti‑Purkinje cell antibody [5] and anti‑neuronal cell antibody [6] have been described in the literature without large‑scale validation. We report the clinical and radiological features of a patient who showed signs of acute cerebellar syndrome associated to MRI evidence of the right cerebellar hemisphere atrophy. Other possible causes, including infective, metabolic or paraneoplastic causes, drugs, alcohol and demyelinating diseases, are excluded by medical history, physical examination and appropriate investigations. The cerebellar ataxia, which was the main clinical feature in our patient, improved following pulse intravenous steroid administration.
Case Report
38 years old diabetic, non-alcoholic pleasant Bangladeshi lady, not known to have any other co morbidities or not on any other medications admitted to our hospital with the complaints of 4 days history of vertigo, vomiting and unsteady gait. She had no visual symptoms, headache, convulsion, altered consciousness, loss of consciousness sphincteric disturbances, fever, weakness of any limbs, speech disturbances, hallucination, or other neurological symptoms. No family history of neurological disease was reported. She has been treated for diabetes in the previous 4 years with oral hypoglycemic drug and diabetes was well controlled. There was no history of any pedal swelling, nocturia, hematuria, oliguria, psychosis, menstrual irregularity, oral ulcer, hair loss, joint pain, photo sensitive rash, any abortion, chronic drug usage (including lithium and anti convulsants), exposure to any known toxin or addiction. On admission, the patient’s pulse was 80 beats/min, blood pressure 125/70 mmHg, respiratory rate 16/min and SpO2 95% while inhaling room air. Neurological examination showed marked limb and truncal ataxia. She presented kinetic tremor involving right arms and dysdiadikokinesia. Horizontal nystagmus was also present with fast phase towards right. She had an ataxic, wide-based gait with tendency to fall towards right and was unable to perform tandem walk. Deep tendon reflexes were normal and symmetrical. No muscle weakness or sensory disturbance was noted. Mental functions, speech, cranial nerve examination, including ocular movement and fundus examination were normal. Meningeal signs were absent. Examinations of other systems including cardiovascular, chest and abdominal were unremarkable.
Initial blood tests including complete blood count, kidney function test, liver function test, random blood sugar, HbA1c, hepatitis profile, TSH were unremarkable. Urinalysis was normal with no presence of protein, glucose, red blood cells, white cell count or cellular casts. Chest radiograph did not show any abnormalities. Cranial magnetic resonance imaging (MRI) with gadolinium ruled out acute ischemic infarct, parenchymal hemorrhage, mass lesion and demyelinating process. More specifically, the cranial MRI failed to reveal any lesion particularly in the posterior fossa that could support the findings of acute cerebellar ataxia. But right cerebellar hemisphere seemed atrophied (Figures 1 & 2). Ideally, a positron emission tomography or a functional MRI could be done to demonstrate areas of dysfunction.
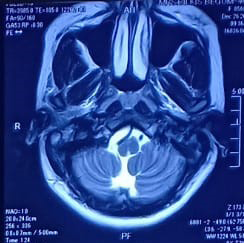
Figure 1 & 2: MER of brain revealed right sided cerebellar atrophy. There was no evidence of ischemic change.
She was started treatment symptomatically with intravenous prochlorperazine, oral flunarizine and betahistine but she failed to improve in next 2 days. There after CSF study was done which revealed normal opening pressure, cell counts, biochestry, gram stain, culture and ADA (adenosine deaminase). In the absence of an infectious or vascular cause, the work-up for an autoimmune disease was pursued. Anti-nuclear antibody by immunofluorescence in HEp-2 cells was strongly positive with fine speckled pattern. Anti-dsDNA antibody was also positive 124 U/ml(positive>75 u/ml). ENA profile, c-ANCA, p-ANCA, anti phospholipid antibody were negative. There was low C3 value of 65 mg/ dL and low C4 value of 6 mg/dL(normal C3 is 80–178 mg/ dl, for C4 is 12–42 mg/dl )The patient thus fulfilled four of the 11 Systemic Lupus International Collaborating Clinics Classification (SLICC) criteria.
A final diagnosis of lupus cerebellitis with right sided cerebellar atrophy was made. Treatment was initiated with injection methylprednisolone (MP) 1 g i.v. 5 days followed by oral prednisolone 1mg/kg body weight along with 2 gram daily of oral mycophenolate mofetil. The patient responded promptly with gradual amelioration of all cerebellar features within the ensuing 10 days. After 3 months of follow‑up, her neurological features improved. As a corollary, her cerebellar atrophy can be attributed to SLE.
Discussion
Acute cerebellitis is an inflammatory disorder most commonly seen in children. It is rare in adults. The pathophysiology is not completely understood. The etiology is typically unknown but may be secondary to medications, paraneoplastic or parainfectious causes, or a specific pathogen (e.g., EBV, HSV, or Mycoplasma pneumoniae). It is more frequently seen in females. The most common presenting symptoms are ataxia (94%), headache (88%), nausea and vomiting (88%), and fever (71%). Altered consciousness is seen in only 29% of patients. Treatment is based on the underlying cause and often consists of antimicrobial and antiviral therapies and steroids.
Acute cerebellar dysfunction in SLE can be due to SLE activity itself as a part of neuropsychiatric SLE (NPSLE), or can be due to acute disseminated encephalomyelitis, diffusely infiltrating glioma or lymphoma, drug-related inflammatory processes or vasculitis [7]. Clinical course and MRI picture of these cases are characteristic, and were absent in our present case. There were no clinical, imaging or CSF findings suggestive of vasculitis in our case.
The estimated prevalence of neuropsychiatric signs in SLE is between 12% and 95%. According to the 1999 American College of Rheumatology consensus statement for NPSLE, 19 neuropsychiatric syndromes have been defined [8]. Further classification included diffuse psychiatric or neuropsychological manifestations and focal neurological syndromes. Localized central nervous system (CNS) involvement is represented by focal NPSLE [9]. However, cerebellar symptoms or ataxia, such as those seen in our patient, has not been described previously as manifestations in the NPSLE spectrum.
The CNS is considered immunologically unique due to the presence of tightly regulated and highly restrictive blood–brain and blood–CSF barrier. Interestingly, the two brain regions preferentially targeted by autoimmunity are the limbic system and the cerebellum. Numerous immune- mediated diseases affect the cerebellum and the mechanisms for each differ. These may include paraneoplastic cerebellar degeneration, Miller Fisher syndrome, postinfectious cerebellitis and cerebellar ataxia associated with connective tissue diseases [9]. Interestingly, cerebellar involvement in SLE occurs only in less than 2% of reported cases [6, 10]. Possible causes of cerebellar ataxia related to SLE are cerebral ischaemia, vasogenic oedema and antibody- mediated dysfunction [10]. Because specific markers of cerebellar involvement in SLE have not been validated, a response to therapy can be accepted as a surrogate marker of immunopathogenesis. Ahmed, et al. [11] reviewed fifteen cases of patients with SLE presenting with cerebellar symptoms. They found that all but one case occurred in females with 80% of patients being between 15 and 34 years of age. Cerebellar involvement was present at the time of SLE diagnosis in five patients, and, with the exception of one patient who was diagnosed with SLE 12 years after cerebellar dysfunction was noted, onset was 1 month to 14 years after SLE diagnosis.
The investigation of choice for cerebellar ataxia is brain MRI [7]. Functional studies such as positron emission tomography (PET), functional MRI, or single photon emission computerized tomography (SPECT) can demonstrate patchy areas of dysfunction in brain areas unaffected on conventional MRI, which suggests an uncoupling of metabolic process independent of obstruction to blood flow. The mechanism of these metabolic derangements is unknown as yet. In our case, conventional MRI failed also to reveal any lesion that could explain the acute cerebellar ataxia. Due to severe financial constraints and logistical problems we could not perform functional brain imaging in our patient. Prompt treatment with i.v. methylprednisolone reverses the cerebellar dysfunction in most cases, as was evident in our case. Delay in initiation of therapy is associated with poorer prognosis [12].
Subcortical and periventricular white matter lesions indicative of small infarcts or edema are commonly observed in the MRI scans of adults with SLE [13]. Quantitative volumetric measures of cerebral and corpus callosum atrophy in adult patients progress over a relatively short period of time and correlate with disease duration, history of NPSLE, aPL positivity and cognitive impairment [14]. Cumulative corticosteroid dosing has been associated only with gray matter atrophy, in particular hippocampal and cerebral atrophy. In a recent study [14, 15, 16] of newly diagnosed adult patients with SLE, cerebral atrophy was found in 18% of patients, probably as a result of disease-associated axonal/ myelin loss, and was unrelated to higher corticosteroid dosing [17]. Although cerebellar changes are associated with neurocognitive deficits in other inflammatory and ischemic disorders, there are minimal data on cerebellar involvement in patients with SLE [2, 18]. In a very recent study of pediatric lupus patients, researchers have found cerebral and cerebellar volume losses in most of the brain MRI of pediatric patients with NPSLE manifestations within the first 4 years of disease presentation [18]. Cerebral and cerebellar volume loss and corpus callosal atrophy occurred in newly diagnosed patients with neurologic manifestations prior to steroid exposure [18]. This may reflect sequelae of active NPSLE and not just physiologic corticosteroid effects. Less prominent volume loss in patients with previous nephritis may be related to more aggressive control of systemic inflammation or vasculopathy by previous immunosuppressive agents [18].
To our knowledge, the evaluation of pooled information regarding patients with NPSLE presenting as cerebellar ataxia has not been done in the literature. However, multiple case reports on the subject have been cited since 1988. The patients described are female and between 14 and 41 years old [12]. These individuals were previously diagnosed with SLE, eventually developing cerebellar ataxia as a neuropsychiatric manifestation of the disease [6, 12, 19]. Majority had imaging evidence, revealing a cerebellar infarct, solitary lesions in the junction between the pons and the medulla, or cerebellar atrophy.
Most reports of cerebellar ataxia in SLE demonstrated response to immunosuppression with high-dose corticosteroid. Immunomodulators such as azathioprine, cyclophosphamide or hydroxychloroquine were also beneficial. Consequently, majority of patients had good outcomes with improvement of neurological symptoms after treatment [6, 12, 19].
The patient’s neurological signs suggested a disorder affecting right hemispheres of the cerebellum. The tempo of the disease progression could be explained by a demyelinating disorder, a neoplasm or a vasculitic syndrome. In this patient, the possibility of a first attack of demyelinating disorders like multiple sclerosis was considered, but there were no suggestive features on brain imaging. Final diagnosis of the patient as SLE was confirmed with the help of autoimmune markers. Reports of cerebellar ataxia in lupus demonstrated response to immunosuppression with high‑dose intravenous corticosteroid. In rare instances [20], a biopsy of cerebellum revealed dense microglial infiltration and perivascular neutrophilic invasion. As specific markers of cerebellar affection in SLE have not been validated, a response to therapy can be accepted as a surrogate marker of immunopathogenesis [21]. However, therapy with mycophenolate mofetil in such a situation has not been reported. So to conclude, we report an interesting case of cerebellar atrophy in SLE with clinical response to a combined regimen with mycophenolate mofetil and oral steroid.
Conclusion
Lupus cerebellitis is an exceedingly rare disorder that needs to be considered in any patient presenting with ataxia that persists despite treatment of other potential underlying causes. The appearance of an acute or subacute cerebellar syndrome with no obvious cause, especially together with emerging associated autoimmune systemic features during the clinical course, should suggest for possible SLE. Such diagnostic hypothesis, albeit not frequent, is crucial due to implications for clinical practice in order to provide a prompt therapy and to improve clinical outcome.
Conflict of Interest
None declared.
References
-
Hochberg MC (1997) Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 40(9): 1725.
-
Appenzeller S, Cendes F, Costallat LT (2008) Cerebellar ataxia in systemic lupus erythematosus. Lupus 17(12): 1122-1126.
-
Manto MU, Rondeaux P, Jacquy J, Hildebrand JG (1996) Subacute pancerebellar syndrome associated with systemic lupus erythematosus. Clin Neurol Neurosurg 98(2): 157-160.
-
Ghosh K, Chatterjee A, Ghosh S, Chakraborty S (2014) Cerebellar ataxia in a young patient: a rare path to lupus. Neurosci Rural Pract 5(S1): S75-S76.
-
Shimomura T, Kuno N, Takenaka T, Maeda M, Takahashi K (1993) Purkinje cell antibody in lupus ataxia. Lancet 342(8867): 375‑376.
-
Iwasaki Y, Okamoto A, Shoda H, Takahashi Y, Fujio K, et al. (2012) Subacute cerebellar ataxia and atrophy developed in a young woman with systemic lupus erythematosus whose cerebrospinal fluid was positive for antineuronal cell antibody. Lupus 21(3): 324‑328.
-
De Bruecker Y, Claus F, Demaerel P, Ballaux F, Sciot R, et al. (2004) MRI findings in acute cerebellitis. Eur Radiol 14(8): 1478-1483.
-
Schwartz N, Stock AD, Putterman C (2019) Neuropsychiatric lupus: new mechanistic insightsand future treatment directions. Nat Rev Rheumatol 15(3): 137-152.
-
McGlasson S, Wiseman S, Wardlaw J, Dhaun N, Hunt DPJ (2018) Neurological disease in lupus: Toward a personalized medicine approach. Front Immunol 9: 1146.
-
Baizabal-Carvallo JF, Bonnet C, Jankovic J (2013) Movement disorders in systemic lupus erythematosus and the antiphospholipid syndrome. J Neural Transm 120(11): 1579-1589.
-
Tomita M, Holman BJ, Williams LS, Pang KC, Santoro TJ (2001) Cerebellar dysfunction is associated with overexpression of proinflammatory cytokine genes in lupus. J Neurosci Res 64(1): 26-33.
-
Singh RR, Prasad K, Kumar A, Misra A, Padmakumar K, et al. (1988) Cerebellar ataxia in systemic lupus erythematosus: three case reports. Ann Rheum Dis 47(11): 954-956.
-
Brey RL (2007) Neuropsychiatric lupus: clinical and imaging aspects. Bull NYU Hosp Jt Dis 65(3): 194-199.
-
Appenzeller S, Rondina JM, Li LM, Costallat LT, Cendes F (2005) Cerebral and corpus callosum atrophy in systemic lupus erythematosus. Arthritis Rheum 52(9): 2783-2789.
-
Appenzeller S, Carnevalle AD, Li LM, Costallat LT, Cendes F (2006) Hippocampal atrophy in systemic lupus erythematosus. Ann Rheum Dis 65(12): 1585-1589.
-
Ainiala H, Dastidar P, Loukkola J, Lehtimäki T, Korpela M, et al. (2005) Cerebral MRI abnormalities and their association with neuropsychiatric manifestations in SLE: a population-based study. Scand J Rheumatol 34(5): 376-382.
-
Petri M, Naqibuddin M, Carson KA, Wallace DJ, Weisman MH, et al. (2008) Brain magnetic resonance imaging in newly diagnosed systemic lupus erythematosus. J Rheumatol 35(12): 2348-2354.
-
Muscal E, Traipe E, de Guzman MM, Myones BL, Brey RL, et al. (2010) Cerebral and cerebellar volume loss in children and adolescents with systemic lupus erythematosus: A review of clinically acquired brain magnetic resonance imaging. J Rheumatol 37(8): 1768- 1775.
-
Smith RW, Ellison DW, Jenkins EA, Gallagher PJ, Cawley MI (1994) Cerebellum and brainstem vasculopathy in systemic lupus erythematosus: two clinico-pathological cases. Ann Rheum Dis 53(5): 327-330.
-
Chattopadhyay P, Dhua D, Philips CA, Saha S (2011) Acute cerebellar ataxia in lupus. Lupus 20(12): 1312‑1315.
-
Kim YS, Park BS, Baek W, Kim SH (2012) Massive vasculitic cerebellar infarction in patient with systemic lupus erythematosus. Neurol India 60(1): 106‑108.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury