Multiple Expansile Jaw Radiolucencies Case Report
Cherubism is a congenital childhood disease of autosomal dominant inheritance, characterized by painless bilateral enlargement of the jaws, in which bone is replaced with fibrous tissue, and is well-known to regress without treatment following puberty. Boys are more affected than girls at the proportion of 2:1
Introduction
Cherubism is a congenital childhood disease of autosomal dominant inheritance, characterized by painless bilateral enlargement of the jaws, in which bone is replaced with fibrous tissue, and is well-known to regress without treatment following puberty. Boys are more affected than girls at the proportion of 2:1 [1, 2]. Jones [3] in described Cherubism as a familial disease, multilocular cystic disease of the jaws. Typical age of onset is 2 to 5 years, with the jaw lesions progressing gradually until puberty when the swelling spontaneously stabilizes and then it regresses [3]. Cherubism lesions impact on the eruption and arrangement of the primary dentition [4] however the effect on the permanent dentition include absence of the molars , teeth with abnormal shape and root resorption [5]. This is a case report that highlights the initial bilateral presentation of Cherubism case and reviews the different aspect of clinical, radiographic and histopathological feature.
Case scenario
A child male patient who was 8 year old presented to the dental clinic with slowly growing painless, bilaterally symmetrical swelling of both jaws. Swelling started at the age of two, and gradually increased in size. It extended posterio-anteriolly from the angle to parasymphysis region of the mandible on both sides. The enlarged jaw was hard on palpation. Skin was freely movable and swellings were immobile. Several teeth were displaced and impacted resulting into malocclusion, there was an expansion of both the buccal and lingual cortical plates, and sub-mandibular lymph nodes were enlarged about 1.5 cm× 1.0 cm in size and tendered in palpation. Family history was not significant. Orthopantamogram (OPG) revealed bilateral multilocular radiolucent lesion, and displacement of un-erupted teeth in the mandible and the maxilla. Hematological investigations were within normal limits, Incision biopsy of the lesion confirmed the diagnosis of cherubism (Figures 1-6).

Figure1: Facial view shows bilateral swelling of the mandible.


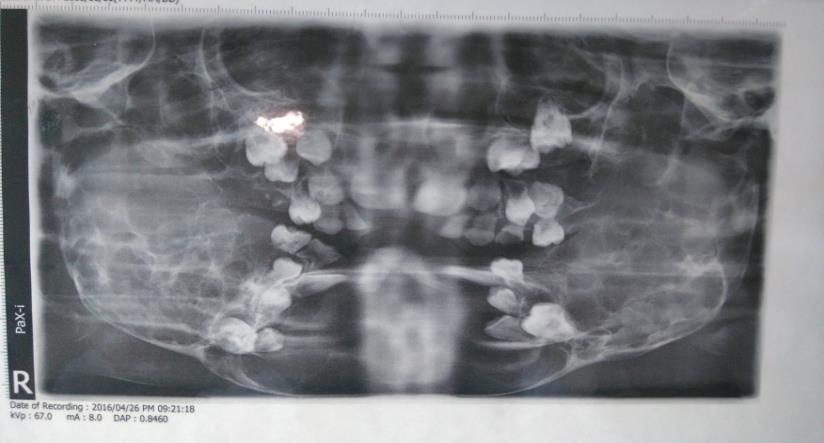
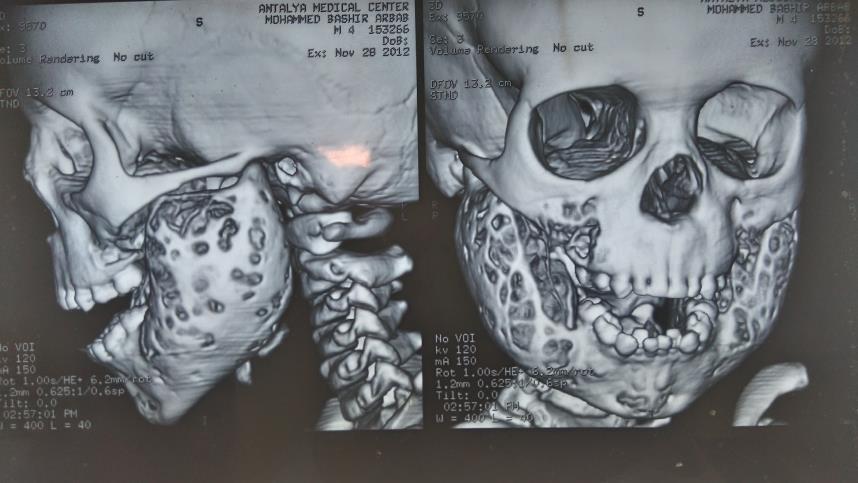
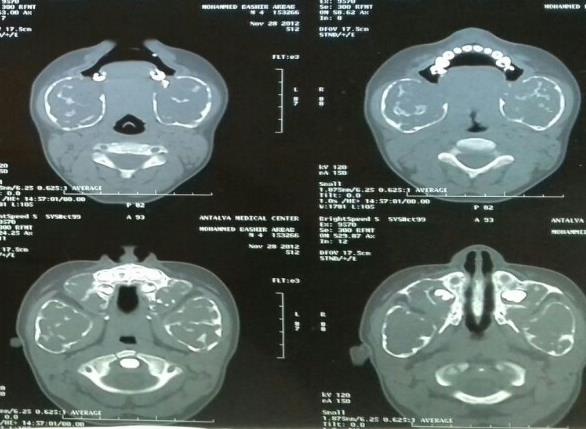
Figure 4&5: 3D and axial cuts of C.T scan shows bilateral large osteolytic mandibular lesions with condylar sparing & maxillary involvement.
Discussion
Cherubism is a rare hereditary childhood benign lesion, which appear as painless bilateral swelling that progress until puberty, WHO categorized it as non-neoplastic bone lesions that affect only the jaws [3, 6] Cherubism has been classified according to the severity grades with a supplement from the Seward & Hankey [7] system:
- Grade I: Involvement of bilateral mandibular molar region and ascending rami, mandible body or mentis.
- Grade II: Involvement of bilateral maxillary tuberosities as well as the lesion of grade I, diffused whole mandible.
- Grade III: Massive involvement of the entire maxilla and mandible except the condyles.
- Grade IV: Involvement of both jaws with condyles. Our patient considered as Grade II on this classification i.e. Involvement of bilateral maxillary tuberosities as well as the lesion of grade I, diffused whole mandible. Silva, et al. [2] reported an unusual extreme case of Cherubism, where it showed aberrant symmetrical orofacial swelling, eyes being pushed upward and appreciable weight loss in 9 months of observation. Perforation of the cortex noted in some cases. Syndromes that associated with Cherubism are; neurofibromatosis type-1, Noonan-like/multiple giant cell lesion syndrome, Ramon syndrome and Jaffe- Campanacci syndrome [8]. The disease clinical presentation in our patient was similar to other studies findings. Radiographically the lesions appeared as multilocular expansile cystic radiolucencies involving the jaws. Histological examination confirms the diagnosis, showing benign lesion composed of cellular fibrous connective tissue with scattered multinucleated giant cells. The management of this condition range from radical surgical reconstruction to an attitude of wait and observes which is being preferred today because it regresses spontaneously after puberty. Radical surgery is recommended when the disease occurs in all four quadrants in case of functional impairment. Poor results have been reported for curettage but only in early childhood due to its high growth potential and lack of complete removal of pathological tissue. A remodeling osteotomy can be done to the affected jaws. An attempt to control this disease with radiotherapy has been rejected because of the potential risk of developing osteoradionecrosis or malignant transformation. Medical treatment in the form of calcitonin is theoretically approved but lacking clinical evidence has unfavors its application though calcitonin has been shown to cause inhibition of bone resorption in cherubic tissue in vitro. However curettage in the beginning of resorption phase has been successful, the majority of the reported cases did not follow the patients to confirm the spontaneous regression. However In some cases, patient’s adult appearance has been found to be normal [3, 9].
Conclusion
The purpose of this is paper is to report a rare case of Cherubism showing the classical clinical features, sequence of progression and radiographic presentations which are the main characteristics of the disease.
References
-
Ozkan Y, Varol A, Turker N, N Aksakalli, S Basa (2003) Clinical and radiological evaluation of cherubism: a sporadic case report and review of the literature. Int J Pediatr Otorhinolaryngol 67(9):1005-1012.
-
Carvalho Silva E, Carvalho Silva GC, Vieira TC (2007) Cherubism: Clinicoradiographic Features, Treatment, and Long-Term Follow-Up of 8 Cases. J Oral Maxillofac Surg 65(3): 517-522.
-
Jones WA (1933) Familial multilocular cystic disease of the jaws. Am J Cancer17: 946-950.
-
Pontes FS, Armando CF, Alberto MK, Hélder ARP, Diele SA, et al. (2007) Aggressive case of cherubism: 17-year follow-up. Int J Pediatr Otorhinolaryngol 71 (5): 831- 835.
-
Kalantar Motamedi MH (1998) Treatment of cherubism with locally aggressive behavior presenting in adulthood: report of four cases and a proposed new grading system. J Oral Maxillofac Surg 56(11): 1336- 1342.
-
Pindborg JJ, Kramer IR (1971) WHO 1st Ed. Geneva: Histological typing of odontogenic tumours, jaw cysts, and allied lesions pp. 18-19.
-
Seward GR, Hankey GT (1957) Cherubism. Oral Surg Oral Med Oral Pathol 10(10): 952-974.
-
Atalar MH, Albayrak E, Erdlinc P, Bulut S (2008) Cherubism as a rare cause of bilateral expansion of the mandible : Radiological manifestations . Journal of Hong Kong College of Radiologists 11: 76-80.
-
Von Wowern N (2000) Cherubism-a 36 year long-term follow-up of two generations in different families and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 90(6): 765-772.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells