Indirect Bonding in Lingual Orthodontics
Indirect bonding of lingual brackets is crucial to the success of lingual orthodontic treatment. Transferring brackets to the pre determined position in a precise manner to patients’ mouth is of paramount importance. This article briefly discusses various in-house lingual bracket-transfer methods that can carry out this task with precision and reliability
Introduction
Currently there are several techniques for positioning and transferring lingual brackets from set-up models to patients’ teeth. Both CAD-CAM technology and manual methods may be used to accomplish this task. While use of CAD-CAM enhances feasibility, reliability and precision, it requires the use of commercial laboratory services, which in turn may increase costs and turnaround times [1, 2, 3]. On the contrary, manual methods of transferring lingual brackets have the advantage of carrying out this procedure in-house in an economical manner. It is imperative that these transfer systems are precise, feasible and if possible, reusable. Assuming that lingual brackets have been already been positioned and their bases have been customized on the malocclusion or set–up models, following is a brief description of in-house lingual bracket-transfer systems:
The Convertible Resin Core system [4]
In this technique individual transfer trays are fabricated using hard resin and elastomeric ligatures. Individual transfer caps are formed on set-up model with help of Duralay resin (Reliance Dental Manufacturing Company, USA). Elastomeric ligature holds the bracket and the transfer tray together and helps to disconnect the transfer tray from the bracket upon completion of indirect bonding. The same transfer tray may be reused in case of bond failure.
KommonBase [5]
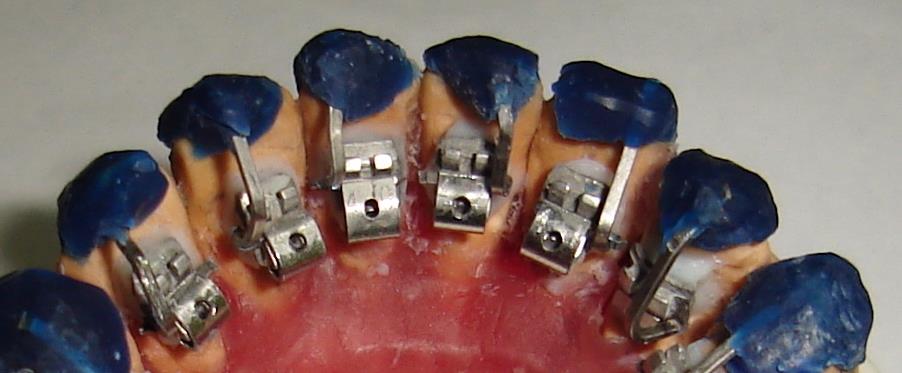
Even though no transfer cap is needed in this technique, the extension of customized bracket pad in itself serves as customized transfer tray (Figure 1). After the bracket bases are customized with KommonBase Resin HV(high viscosity), these bases are extended on the tooth on the set up model with KommonBase Resin LV(low viscosity) in occlusal, mesial and distal direction and then polymerized with a light cure. The use of low viscosity resin during the extension phase imparts flexibility to the material and therefore minimizes fracture of the material.
![Figure 1: GC Kommonbase customized bracket bases with resin extensions. Teeth are etched, rinsed and dried and clinical bonding is accomplished with light curable resin-modified glass ionomer cement. The advantage of using RGIC is that the bond strength of an RGIC is not affected in moist condition in situations where brackets are bonded in close proximity to gingival tissue [4-6].](/fulltextimages/1214/fig_1.jpeg)
Figure 1: GC Kommonbase customized bracket bases with resin extensions. Teeth are etched, rinsed and dried and clinical bonding is accomplished with light curable resin-modified glass ionomer cement. The advantage of using RGIC is that the bond strength of an RGIC is not affected in moist condition in situations where brackets are bonded in close proximity to gingival tissue [4, 5, 6].
The Hybrid Core System [7]
In this system, a combination of silicone and composite resin is used to fabricate an indirect bonding tray. First a layer of silicone is applied to cover the bracket then a layer of composite resin follows this step. Silicone helps in easy tray removal while resin layer provides rigidity and stability to the tray [7].
Single or Dual Tray Method
Transfer trays may be fabricated with conventional single or dual trays methods using polyvinylsiloxane (PVS), PVS putty, PVS vacuum-form materials as in labial orthodontics [8, 9, 10, 11, 12]. Single trays made out of PVS putty, Vacuum form, or even hot glue gun may be used for indirect bonding but for the sake of better control, dual tray methods are preferred [12]. Furthermore, it has been shown that silicone based transfer-tray methods for transferring brackets have higher accuracy than methods that utilize exclusively vacuum-formed trays [12].
Dual trays may be fabricated using the following methods
Double PVS Tray Method [8]: Dispense a small amount of transparent silicone like Emiluna (Opal Orthodontics, Ultradent) from the cartridge onto each bracket, making sure that brackets are fully covered with Emiluna Figure 2. This will act as an inner soft layer. Before this inner layer sets up, quickly apply a second layer of thick, firm clear silicone like Lumaloc (Opal Orthodontics, Ultradent). The purpose of the outer layer is to impart rigidity to the tray.

Double vacuum form tray method: Same technique may be done with help of a vacuum form/suck down method [9] using Biostar (Scheu Dental, Germany). First a1- 1.5mm Bioplast (Scheu Dental, Germany) material is sucked down on the model to form the inner layer, then a silicone spray separator is applied to the top of this inner layer. After this, a 1mm Biocryl (Scheu Dental, Germany) splint type material is sucked down over the inner layer to form a hard outer tray. Rest of the indirect bonding can be accomplished as usual. Other Methods: There are other dual tray methods like one described by Dr. Pablo Echarri [13] in which first individual tooth transfer trays are fabricated based on CRC ready-made core system [4]and then these individual trays are connected to one another by an overlay single silicone tray [13]. Dual/single tray transfer systems have an advantage that all teeth in the arch can be bonded simultaneously with precision or these trays may be sectioned into quadrants depending on operator’s preference.
Jig/Wire Supported Transfer Tray Method
A few orthodontic manufacturers have created unique accessories with their bracket system such as, smart jig in Evolution bracket (AdentaGmgH, Gilching, Germany) and set-up wire in 3D torque lingual bracket (Forestadent) to simplify the bracket-transfer methods. As such accessories are not available with every bracket system on the market, few clinicians have overcome these hurdles and have innovated their own accessories, which can work with most of the available bracket systems [14, 15, 16].
Weldable Wire Connector [14]
This technique uses a combination of beta-titanium wires (0.018” x 0.025” and 0.017”x0.025”) in constructing the Weldable Wire Connector (WWC). These wires are welded together in a way that 0.018” x 0.025” part goes into the bracket slot and 0.017”x0.025” part is used to fabricate the resin cap (Figure 3). The former part of the WWC allows for the use of a full-size rectangular wire in the bracket slot, rendering 3 dimensional control, whereas the latter section of the WWC imparts sufficient flexibility to the transfer tray so that it can be quickly disconnected from the bonded bracket with ease. The technique is unique that the same WWC may be reused for re bonding in case of bond failure, saving chair time.
Conclusion
The use of in-office laboratory procedures not only keeps the provider in full control of the lingual case set-up but also helps minimize the laboratory costs associated with it. As discussed above, there are several in-office laboratory options to transfer brackets from the indirect bonding models to patients’ teeth. Depending upon the clinician’s preference,any of these methods can accomplish this task with precision and reliability. For example, if the operator prefers to bond individual brackets then methods like“The convertible resin core system”, “Weldable wire connector” or “Kommon base“techniques may be used, and if the clinician opts for a single step indirect bonding procedure, full arch PVS or vacuum formed trays may be used.For better control, full arch double PVS or Vacuum formed trays are preferred over full arch single trays.
References
-
Fillion D (2011) Lingual straight wire treatment with the Orapix system. J Clin Orthod 45(9): 488-497.
-
Gimenez CM (2011) Digital technologies and CAD/CAM systems applied to lingual orthodontics: The future is already a reality. Dental Press J Orthod 6(2): 22-27.
-
Goraya KS (2017) Customization in lingual orthodontics. Research & Reviews: Journal of Dental Sciences 5(2): 8-12.
-
Kim T, Bae G, Cho J (2008) New indirect bonding method in lingual orthodontics: convertible resin core system. J Clin Orthod 34: 348-350.
-
Komori A, Fujisawa M, Iguchi S (2010) KommonBase for precise direct bonding of lingual orthodontic brackets. Int Orthod 8(1): 14-27.
-
Cacciafesta V, Jost-Brinkmann PG, Sussenberger U, Miethke RR (1998) Effects of saliva and water contamination on the enamel shear bond strength of a light-cured glass ionomer cement. Am J Orthod Dentofacial Orthop 113(4): 402-427.
-
Matsuno I, Okuda S, Nodera Y (2003) The hybrid core system for indirect bonding. J Clin Orthod 37(3): 160- 161.
-
Koga M, Watanabe K, Koga T (2007) Quick indirect bonding system (Quick IDBS): An indirect bonding technique using a double-silicone bracket transfer tray. Semin Orthod 13(1): 11-18.
-
Sondhi A (2007) Effective and efficient indirect bonding: The Sondhi method. Semin Orthod 13(1): 43-57.
-
Moskowitz EM (2007) Indirect bonding with a thermal cured composite. Semin Orthod 13(1): 69-74.
-
Kalange JT (2007) Prescription-based precision full arch indirect bonding. Semin Orthod 13(1): 19-42.
-
Castilla AE, Crowe JJ, Moses JR, Wang M, Ferracane JL, et al. (2014) Measurement and comparison of bracket transfer accuracy of five indirect bonding techniques. Angle Orthod 84(4): 607-614.
-
Lobiondo PE (2006) Lingual technique direct bonding: Double transfer tray technique. World journal of orthodontics 7(2): 154-158.
-
Goraya KS, Boparai BK (2009) Weldable Wire Connector: A New Bracket-Transfer System In Lingual Orthodontics. Virtual Journal of Orthodontics 8 (3): 1-4.
-
Arima VO, Arima NE, Eto LF (2008) Lingual technique- Arima’s transferring master mold. Lingual News-serial online 6(1).
-
Hong RK, Soh BC (1996) Customized indirect bonding method for lingual orthodontics. J Clin Orthod 30: 650-652.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells