Herpetiform Ulceration Involving Pharynx – Case Report
Oral ulceration is routinely encountered by dentists in their daily practice. Painful ulcers hamper dental treatment besides rendering patient incapacitating, in terms of dental procedures. Herpetiform ulcers occur mostly in female patients and rarely involve the posterior palate. A male patient reported with multiple oral ulceration some of them being painful at a particular area while some non painful. The ulcers were numerous and involved tongue while some of them involved the soft palate. A systematic clinical history and oral examination that included a detailed review of the general body systems to preclude any relation to a systemic inflammatory process was done. The patient’s history revealed an emotional stress and poor diet intake. The patient was prescribed multivitamin and was asked to consume vitamin rich diet
Introduction
Herpetiform ulcers are a form of aphthous ulcer which is derived from a Greek word “aphtha” meaning ulceration whereas herpetiform means having clusters of vesicles that resemble the skin lesions of herpes virus infections [1]. Also called canker sores, they are primarily painful ulcers that dentists encounters in their practice. They vary in size, location, number and extent, but usually occur as recurrent, multiple, small, round or ovoid ulcers with circumscribed margins having yellow or gray floors encircled by erythematous halos, and present first in childhood or adolescence [2, 3, 4, 5]. Herpetiform ulcers (recurrent aphthous ulcers RAU) affect about 20% of the world population [6] and has been described under three different clinical variants with different incidences. Minor RAU being most common variant constitutes 80%, while major RAU constitutes 10- 15% with the rest representing as herpetiform ulceration [1, 7] which predominantly occurs more in women and their site of occurrence is usually lips, tongue, cheeks, floor of mouth and gingiva [8]. This article presents a case of herpetiform ulceration of the oral cavity of an adult male patient and besides normal locations it also was present on the palatopharyngeal wall.
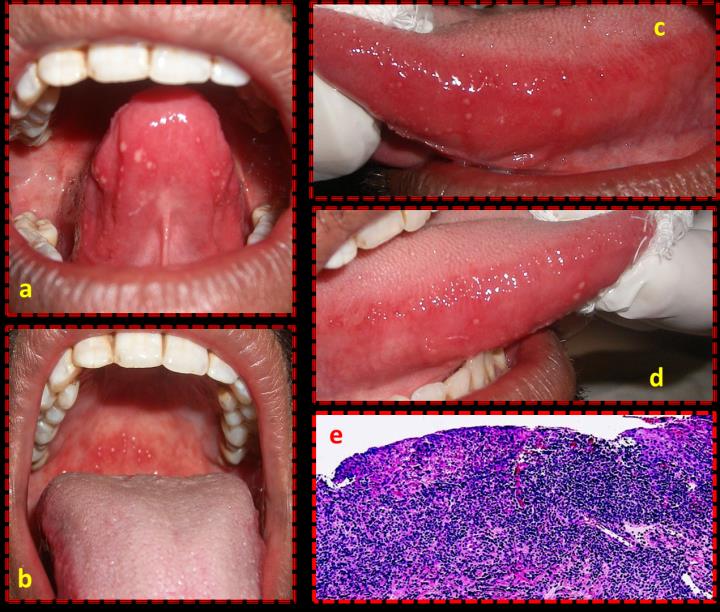
A male patient, aged 38 years, was referred to the department of Prosthodontics for a crown restoration after undergoing endodontic treatment in relation to mandibular left first molar. Medical, social, dietary, drug and dental history were non contributory. Extra oral examination disclosed normal features while intra orally the patient demonstrated multiple ulcerations on the underside of the tongue (Figure 1a), on the anterior part of the soft palate (Figure 1b) and on the lateral borders of the tongue (Figure 1c,d). Visible ulcers ranging from 2- 3 mm and up to 75 or more in number were present. Most of the ulcers were having a clinically visible differentiated border, while some of the ulcers had yellow floors with erythemateous halo. The patient reported that many of them were mildly painful and tender. Subsequent detailed history was taken to rule out ulceration due to systemic disturbance. Clinically relevant history disclosed a period of emotional stress since last few months with rare intake of vitamin containing foods. The patient reported fewer episodes of cheek biting during these months. There was no clinical evidence of scarring of any healed ulcers. Because of the discomfort and pain associated with the ulcers, the patient was referred to department of oral medicine and diagnosis where after undergoing histopathological investigation (Figure 1e), he was put on a multi vitamin regimen for two months and was given a dietary counselling. Fabrication of the crown was deferred for three weeks and the patient was instructed not to bite anything hard with the endodontically treated tooth.
Discussion
Recurrent aphthous stomatitis (RAS) has three variants namely Minor RAS, Major RAS and Herpetiform ulceration as described by Stanley in 1972.3 The lesion in this case are consistent with herpetiform type of ulceration which usually last for 10 to 14 days. Most of the findings of this case are in accordance with already established features of herpetiform ulceration. Although twice as common in women and occur on tongue, gingiva and lingual mucosa, we report a case of an adult male with a variation in location, which is the region of the palatopharyngeal wall in relation to the soft palate. The patient did not report any history of such problem in the family nor was there any history of recent trauma except cheek biting. The patient reported rare intake of fruits while he reported stress due to personal problems. Gallo [9] has proposed that trauma in the form of lip or cheek biting or parafunctional habits may act as a triggering or predisposing factor to ulceration. Diagnosis of Herpetiform ulceration is based on a clear, well defined history taking, clinical manifestations and histopathology. The most important aspect of diagnosis is to rule out other local and systemic causes of ulceration. Various criteria have been proposed for the diagnosis of idiopathic recurrent aphthous stomatitis [10].
Conclusion
Herpetiform ulceration although predominant in women can occur in men and the lesion may involve the soft palate also. Ulceration due to systemic causes must be ruled out before recommending any treatment. Dental procedures can be deferred in cases where pain and discomfort are associated.
Acknowledgements
The authors would like to acknowledge the prompt effort of the staff of oral medicine and diagnosis.
References
-
Preeti L, Magesh KT, Rajkumar K, Karthik R (2011) Recurrent aphthous stomatitis. J Oral Maxillofac Pathol 15(3): 252-256.
-
Jurge S, Kuffer R, Scully C, Porter SR (2006) Recurrent aphthous stomatitis. Oral Dis 12(1): 1-21.
-
Stanley HR (1972) Aphthous lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 30: 407-416.
-
Scully C, Porter S (1989) Recurrent aphthous stomatitis: Current concepts of etiology, pathogenesis and management. J Oral Pathol Med 18(1): 21-27.
-
Femanio F, Lanz A, Buonaiuto A, Gombos F, Nunziata M, et al. (2007) Guidelines for diagnosis and management of aphthous stomatitis. Pediatr Infect Dis J 26(8): 728-732.
-
Casiglia JM (2002) Recurrent aphthous stomatitis: etiology, diagnosis, and treatment. Gen Dent 50(2): 157-166.
-
Cawson RA, Odell EW (2008) Cawson's Essentials of Oral Pathology and Oral Medicine. (8th edn), Philadelphia: Elseivier.
-
Wallace A, Rogers HJ, Hughes SC, Hegarty AM, Zaitoun H, et al. (2015) Management of recurrent aphthous stomatitis in children. Oral Medicine. 42(6): 564-572.
-
Gallo Cde B, Mimura MA, Sugaya NN (2009) Psychological stress and recurrent aphthous stomatitis. Clinics (Sao Paulo) 64(7): 645-648.
-
Natah SS, Konttinen YT, Enattah NS, Ashammakhi N, Sharkey KA, et al. (2004) Recurrent aphthous ulcers today: A review of growing knowledge. Int J Oral Maxillofac Surg 33(3): 221-234.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells