One Stage Sinus Augmentation with Simultaneous Implant Placement- A Predictable Procedure in Implantology
Over the years implant placement has become a standard treatment procedure for replacement of missing teeth. The placement of dental implants in posterior maxilla at times presents a unique clinical rehabilitation challenge due to the presence of insufficient quantity & quality of bone. The goal of sinus floor augmentation is to lift the schneiderian membrane from the floor of the sinus to create a superiorly located sinus floor with a space between it and the deficient alveolar ridge. The present case report highlights the use of allografts for simultaneous dental implant placement during sinus augmentation in a case with posterior atrophic maxillary ridge height of less than 6 mm.
Introduction
The pneumatisation of the maxillary sinus coupled with alveolar bone resorption frequently leads to insufficient volume of bone in posterior maxilla. The placement of implants presents a challenge in such situations and during the last decade various surgical procedures for augmenting the maxillary sinus have evolved [1, 2, 3]. The goal of sinus floor augmentation is to lift the schneiderian membrane from the floor of the sinus to create a superiorly located sinus floor with a space between it and the deficient alveolar ridge. The simultaneous placement of dental implants during sinus augmentation was initially limited to cases wherein a minimum of 4 to 5 mm alveolar bone was present coronal to the sinus floor. This was chosen arbitrarily as the minimal amount of bone, most likely because of its ability to provide initial implant stability and accurate implant location, inclination and parallelism [4]. Currently, there is no consensus of specific bone height limit for a simultaneous procedure, as similar procedures with alveolar bone height of only 1 to 2 mm have been reported [5]. A crucial factor for osseointegration of dental implants in sinus lift procedures is the presence of primary implant stability post placement of an implant [6]. Simultaneous placement of dental implant during sinus augmentation is advantageous to the patient because of lesser number of surgical interventions as well as reduction in the required time for completing the implant-supported prosthesis [7]. The present case report highlights the use of allografts for simultaneous dental implant placement during sinus augmentation in a case with posterior atrophic maxillary ridge height of less than 6 mm.
A 41-year-old male patient reported to this clinic with chief complaint of missing upper posterior teeth. History
of present illness revealed loss of 16, 17 due to caries. The medical and family histories were non-contributory. Intra-oral examination revealed missing 16, 17 and an alveolar ridge width of about 6mm in that region. IOPA radiograph revealed insufficient vertical residual ridge height of about 4mm in the region of 16 (Figure 1).

Figure 1: Pre-operative Radiograph. Patient was systemically healthy, non-smoker, without any deleterious habits. There was no evidence of any abnormality with respect to the maxillary sinus. Treatment protocol arrived at was placement of two implants with the dimensions of 3.4mm diameter and 11mm length with simultaneous sinus augmentation with allografts (DemboneTM; Los Angeles, CA). All procedures were fully explained to the patient and an informed consent was obtained.
Sinus Floor Augmentation Technique
Local anaesthesia was achieved by posterior superior alveolar and greater palatine nerve block with 2% lignocaine and 1,80000 Adrenaline. The surgical procedures were performed under standard aseptic conditions. Initial horizontal sub crestal incision was placed palatally on the edentulous area extending as sulcular incision to adjacent tooth. Two vertical releasing incisions extending up to the mucogingival line were placed on the buccal side and a mucoperiosteal flap was raised with periosteal elevator to expose the antero- lateral wall of the antrum (Figures 2 & 3).

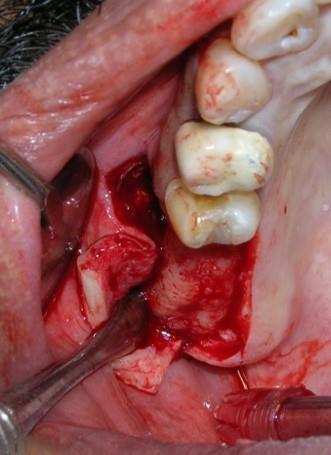
Figure 3: Exposure of Bony antral wall. A low speed high torque round bur with copious saline irrigation was used to outline a rectangular buccal window (Figure 4). The window was accordingly created and care was taken not to perforate the sinus membrane. Once the outline was completed, bone tap was used to separate the lateral sinus window wall. A delicate dissection, using blunt sinus elevators was performed to push the sinus membrane inwards and upwards. The membrane was released without any tension to provide an adequate compartment for placement of the implants with the allograft material (Figure 5). The cut window wall was pushed superiorly like a trap door so that the elevated sinus membrane rested on the bony wall. The distance between the alveolar crest and the inferior border of the window was measured to be 6 mm to facilitate simultaneous orientation of the implant.

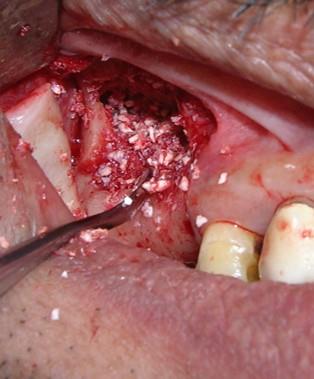
Figure 5: Placement of graft material. The implant site was marked using a surgical stent and the osteotomy was performed using sequential drills as recommended by the manufacturer. The implants were inserted and wrenched into the osteotomy site prepared on the alveolar crest by a hand-heldratchet. To achieve complete adaptation and stabilisation of the implant the created compartment was packed with allograft bone graft material (DemboneTM; Los Angeles, CA) and the created window covered by a bioabsorbable membrane (Periocol®-GTR, Eucare) (Figure 6). Primary closure of the mucoperiosteal flap was achieved using 3-0 silk sutures (Figure 7). Amoxicillin+Clavulanic acid 625 mg bid, Tinidazole 500 mg bid, Brufen+Paracetamoltid and 0.2% Chlorhexidine mouthwash were prescribed for 5 days during the postoperative period. Postoperative instructions were given. Sutures were removed on the 10th day, and the patient was scheduled for follow-up recall visits at 2 weeks and at 1, 2, 3 and 6 months. Healing was uneventful.
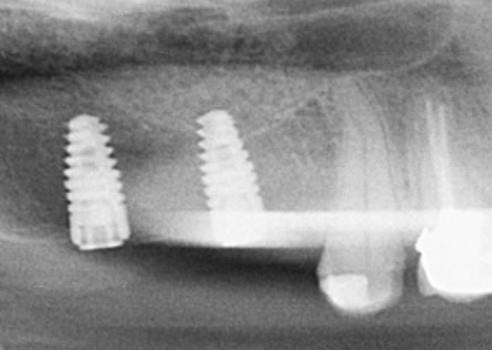
Figure 7: Primary approximation of mucoperiosteal flaps. Post-operative periapical radiographs were recorded at 6 months to assess the radiographic features of uptake of the graft, newly formed bone, and their close relationship to the implants (Figure 8). Clinical assessment at the time of recall visits included implant stability, crestal bone resorption and pain or discomfort. Prosthetic rehabilitation was carried out after six months with PFM crown. The clinical & radiographic assessment showed successful function and excellent peri-implant parameters with no pain or discomfort to the patient.
Discussion
The sinus augmentation procedure for posterior atrophic maxilla is becoming a well-established, predictable and accepted procedure. A variety of graft materials, ranging from autogenous (intraoral or extraoral) to various combinations of allografts, xenografts and alloplastic materials with predictable results have been reported [2, 3]. It has been shown that in an atrophic maxilla when sufficient crestal bone exists to stabilize the implant, sinus augmentation with simultaneous implant placement is a predictable procedure [8]. The survival rate varies depending on the graft material: autogenous 87.7%; combination of autogenous and bone substitutes 94.88%; and bone substitutes alone 95.98%. No difference in the survival rates between simultaneously placed implants with sinus lifts (92.17%) and delayed procedures (92.93%) were observed [2]. Sinus floor augmentation with simultaneous implant placement in severely atrophic maxilla may pose technical problems and complications such as; releasing of the mount from the implant (10.2%), which might cause the dislocation of the implant from its original implantation axis and the bone fractures between the sinus-augmentation window and the implant osteotomy site (3.4%) [9]. This case report not only highlights the merit of using sinus augmentation and simultaneous implant placement but also the reduced duration of treatment. Antibiotics and 0.2 % chlorhexidine mouthwash were prescribed to decrease the incidence of post-operative infection. Chlorhexidine being a broad-spectrum antimicrobial agent is known to decrease the incidence of post-operative infection [10]. However, the incidence of sinus infections can be around 3%, despite administration of antibiotics [11]. The post-operative radiographic evaluation after 6 months revealed a well osseo- integrated implant. Clinically the implant was stable. Major concerns of the ibid procedure are the initial stabilization of the bone graft; its impact on the implant stability and membrane perforation. The rate of membrane perforation which is one of the most common complication was reported to range from 10% to 56%. It has been reported that the use of piezosurgery along with bioabsorbable membranes, sealants and oxidized regenerated cellulose minimises the complications. Sinus lining perforation may deter the clinician to continue the implant placement. The major problem following membrane perforation is the loss of graft particles into the air chamber of the sinus [9]. Therefore the membrane elevation must be carefully executed to avoid the membrane perforation so that in case if it occurs it is still possible to continue the procedure safely after repair [11].
Conclusion
The main advantage of simultaneous implant placement with sinus floor augmentation is its ability to provide initial stability for the implant and the grafting material without the need for autogenous bone harvesting. Further clinical and histologic studies are required before it can be recommended for routine use in sinus augmentation procedures with simultaneous implant placement in posterior atrophic maxillary ridges with height of less than 6mm.
References
-
Wallace SS, Froum SJ (2003) Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann Periodontol 8(1): 328-343.
-
Del Fabbro M, Testori T, Francetti L, Weinstein R (2004) Systematic review of survival rates for implants placed in the grafted maxillary sinus. Int J Periodontics Restorative Dent 24(6): 565-577.
-
Nkenke E, Stelzle F (2009) Clinical outcomes of sinus floor augmentation for implant placement using autogenous bone or bone substitutes: a systematic review. Clin Oral Implants Res 20: 124-133.
-
Smiler DG, Johnson PW, Lozada JL, Misch C, Rosenlicht JL, et al. (1992) Sinus lift grafts and endosseous implants. Treatment of the atrophic posterior maxilla. Dent Clin North Am 36(1): 151- 186.
-
Peleg M, Mazor Z, Chaushu G, Garg A (1998) Sinus floor augmentation with simultaneous implant placement in the severely atrophic maxilla. J Periodontol 69(12): 1397-1403.
-
Achong RM, Block MS (2006) Sinus floor augmentation: Simultaneous versus delayed implant placement In: Jensen OT, (Eds.), The Sinus Bone Graft. Carol Stream, IL: Quintessence Publishing, 2006: 60- 65.
-
Khoury F (1999) Augmentation of the sinus floor with mandibular bone block and simultaneous implantation: a 6-year clinical investigation. Int J Oral Maxillofac Implants 14(4): 557-564.
-
Peleg M, Garg AK, Mazor Z (2006) Predictability of simultaneous implant placement in the severely atrophic posterior maxilla. A 9-year longitudinal experience study of 2,132 implants placed into 731 human sinus grafts. Int J Oral Maxillofac Implants 21(1): 94-102.
-
Gavriel C, Ofer M, Shlomo C, Joseph N (2009) The use of cancellous block allograft for sinus floor augmentation with simultaneous implant placement in the posterior atrophic maxilla. J Periodontol 80(3): 422-428.
-
Rath SK, Singh M (2013) Comparative clinical and microbiological efficacy of mouthwashes containing 0.2% and 0.12% chlorhexidine. Dent Res J (Isfahan) 10(3): 364-369.
-
Schwartz-Arad D, Herzberg R, Dolev E (2004) The prevalence of surgical complications of the sinus graft procedure and their impact on implant survival. J Periodontol 75(4): 511-516.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells