Endowment for Implantology: Lasers
With dentistry in this high tech and changing era, we are fortunate to have many technological innovations to enhance and ameliorate the various treatment modalities. The archetypal of the term high tech is LASER which is an acronym and stands for Light Amplification by Stimulated Emission of Radiation. Its introduction to the prosthodontics and dental implantology has replaced many conventional surgical and technical procedures once thought only possible with the conventional dental drill or scalpel. This review article aims at describing the types, the expanding application and indications of the dental lasers in the field of dental implantology which provide the patient with the rigorous treatment that may minimize pain and recovery time.
Introduction
In this modern era of implant dentistry, surgeons are offered many sophisticated products to improve the quality of the treatment rendered to the patients. One of these evolutions is LASER, which is an acronym and stands for Light Amplification by Stimulated Emission of Radiation. It has begun to revolutionise dentistry and has become its inseparable part. The coextension of implant dentistry and lasers is quite apparent and as they are being put to use the prognosis of the implant treatment is improving. Several advantages of using lasers in implant dentistry have been documented like simpler treatment, truncated complications and patient & clinician friendly clinical procedures without compromising the safety, effectivity and precision of the treatment and its prognosis. The objective of this article is to enlighten the properties, types and the current and possible future clinical applications of lasers in Implant dentistry.
Historical Development
The conceptual basis for production of lasers i.e. stimulated emission of radiation was postulated by Albert Einstein in 1917. Later, in 1957 the term laser was coined by Gordon Gould [1]. The first laser was introduced by Theodore Maimen, in which ruby was used as the active medium, on 16th May 1960 at the Hughes Research Laboratory in Malibu, California [2]. In 1961, Javan, et al. described the first gas and continuously operating laser [3]. The CO2 (Carbon-dioxide) laser has been used in oral and maxillofacial surgery for both hard and soft tissues, since its development in 1964. In the same year Nd: YAG (Neodymium-doped yttrium aluminum garnet) was developed by Geusic for medical use, like ophthalmology [4]. This ophthalmic Nd: YAG laser was then modified by Drs William and Terry Myers and the first dental laser was designed in 1989 [5, 6]. Then, in 1997 an all tissue Erbium family laser consisting of Er: YAG (Erbium-
dopedyttrium aluminium garnet) & Er, Cr: YSGG (Erbium Chromium doped Yttrium Scandium Gallium Garnet) was introduced that can be used both for the hard and soft tissues [7]. Since, then the use of lasers for various clinical procedures has increased rapidly.
Basic Components of Laser and its Production
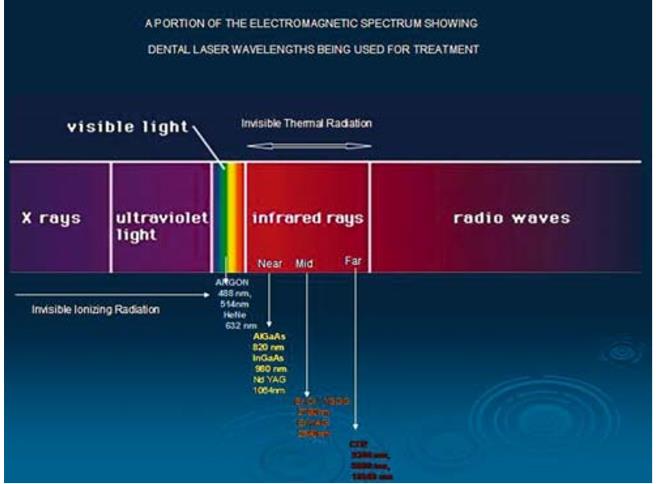
Laser light is a form of an electromagnetic energy [8] which is formed by stimulating the medium from an external energy source that leads to the emission of the photons. Also, it can be described as a man-made single photon wavelength [9]. Laser has 3 basic components (Figure 1): a) Active/ Laser medium: can be solid, liquid, gas or a crystal. It determines the wavelength as well as the nomenclature of the laser [8, 10]. b) Laser cavity/ Optical cavity/ Housing tube: It is an internally polished tube, with co-axially arranged mirrors at both the ends [8]. One of the two mirrors is fully reflective and the other one is partially reflective [10]. c) Pumping mechanism / external energising unit: is a man-made source of primary energy that pumps the atoms of the active medium to higher energy levels. It can either be a flashlight, arc-light or an electromagnetic coil [8, 10]. When atoms of the active medium are bombarded with photons from external energy source, the incident light energy is absorbed by the target atom resulting in the movement of electron to the higher energy level and making it unstable. This unstable state results in the emission of photonic energy (Spontaneous emission). When this already unstable or energised atom is bombarded with a second photon, emission of two coherent photons of identical wavelength takes place and this phenomenon was termed as “Stimulated emission”. These coherent photons energize more atoms, which emit additional identical photons stimulating more surrounding atoms. To maintain this excitation process a constant supply of energy is required [8].
![Figure 1: Typical components of a LASER [10].](/fulltextimages/1808/fig_1.jpeg)
Unique Characteristics of Lasers
a) Monochromaticity: All the waves of the emitted laser have same frequency and wavelength and therefore, a specific colour [8, 10]. b) Collimation: Emitted beam have specific spatial boundaries ensuring a constant parallelism between all the waves, thereby lowering the divergence of the emitted beam [8, 10]. c) Coherency: Light waves are all in phase with one another and have identical peaks and valleys [8].
Classification of Lasers
Based on the type of tissue they penetrate [8]
| Soft tissue lasers | Argon, Nd:YAG, He-Ne, GaAs, Diode |
|---|---|
| Hard tissue lasers | Er:YAG, Er,Cr:YSGG |
Based on type of medium [4].
| Gas lasers | Argon, CO 2 |
|---|---|
| Liquid | Dyes |
| Solid | Nd:YAG, Er:YAG, Diode |
| Semiconductor | Hybrid silicon laser |
| Excimers | Ar-F, Kr-F, Xe-F |
| UV light | 100-400nm | Not used in dentistry |
|---|---|---|
| Visible light | 400-750nm | Most commonly used in dentistry |
| Infrared light | 750- 1000nm | Most dental lasers are in this spectrum |
According to ANSI and OHSA standards Lasers are Classified as [11]
a) Class I- These are low powered lasers that are safe to use. e.g. Laser beam pointer b) Class II- Low powered visible lasers that are hazardous only when viewed directly for longer than 1000 seconds, e.g. He-Ne lasers c) Class II b- Low powered visible lasers that are hazardous when viewed for more than 0.25 seconds. d) Class III a- Medium powered lasers that are normally hazardous if viewed for less than 0.25 seconds without magnifying optics.
e) Class III b- Medium powered lasers that can be hazardous if viewed directly. f) Class IV - These are high powered lasers (> 0.5 W) that produce ocular skin and fire hazards.
Based upon Duration of Laser Emission [12]
a) Continuous wave (CW) b) Single pulsed (normal mode) lasers c) Single pulsed q-switched lasers d) Repetitively pulsed or scanning lasers e) Mode locked lasers
Based on Emission Mode [8]
a) Continuous wave mode b) Gated pulse mode c) Free-running pulse mode (“True-pulsed”)
Based on the Method of Use [8]
a) Contact mode: Diode b) Non-contact mode: Er:YAG; Er,Cr:YSGG
Advantages of Using Lasers in Implantology
The advantages of using lasers in implantology are similar to the other soft tissue dental procedure and these include increased hemostasis (which further enhances the visibility during surgical procedure), minimal damage to the surrounding tissues, reduced inflammation, reduced infection and pain postoperatively and superior as well as rapid healing. The hard tissue ablation capability of erbium lasers has made it possible to use erbium lasers for osteotomy and decontamination of infected and ailing implant bodies [6].
Different Types of Lasers Used in Implantology
Argon Lasers
Uses argon gas as the active medium. They operate at 2 emission wavelengths used in dentistry: 488 nm and 514 nm and falls in blue-green visible spectrum. It is fiberoptically delivered in the wave and gated pulsed modes. The 488nm blue light is used mainly for curing composite resin whereas 514 nm blue-green light has its peak absorption in hemoglobin, hemosiderin and melanin; thus, it is mainly used for the soft tissue procedures like gingivectomy and coagulation [3, 8].
Diode Lasers
Nowadays, types of diodes available for dental use are Indium-Gallium-Arsenide-Phosphide (InGaAsP Diode); Gallium-Aluminum-Arsenide (GaAlAs Diode); Gallium- Arsenide (GaAs Diode). Its wavelength ranges from 655- 980nm and utilizes flexible quartz fiber. It has more affinity for the pigmented soft tissue; this makes it an excellent haemostatic agent. It is used for soft tissue removal in contact mode and for deeper coagulation in non-contact mode. These systems can also be used as low level laser therapy to biostimulate the osteoblasts around implants. Tissue penetration is less than Nd: YAG, thus have the potential to heat damage of the underlying bone. The depth of soft tissue penetration is approximately 2 ± 1 mm [3, 8].
Nd: YAG Lasers
Nd: YAG laser was first introduced by Geusic in 1964 [3]. It employs neodymium doped yttrium-aluminium- garnet crystal as the active medium and has the wavelength of 1,064nm. It is highly absorbed by melanin, which makes it a very beneficial surgical laser for cutting and coagulating dental soft tissues, with good hemostasis [1]. Nd:YAG has been a popular wavelength used for second stage surgery but a few investigators contended that its use in implantology is contraindicated. This laser energy has the potential to transmit heat to the bone from heated implant surface, effect metal surface of the implant and can lead to pitting, porosity and melting of the implant surface [6, 13, 14, 15].
Carbon Dioxide Lasers
In 1964, CO2 laser was first developed by Patel, et al. [3]. Its active medium is a mixture of CO2, helium and nitrogen in the proportions of 8:7:1 & has 3 emission wavelengths i.e. 9,300nm; 9,600nm and 10,600nm [8]. Development of Hollow wave guide technology has made its use easier in the oral cavity [3]. The light energy, whose wavelength is 10,600 nm, is well absorbed by water (second only to the erbium family) [4, 8] and have excellent haemostatic properties thus, can be used for soft tissue procedures like second stage surgery in implants [6]. Whereas another wavelength of this laser i.e. 9,300 nm can be employed for both the hard and soft tissues [16] and has shallow depth of penetration into tissue ranging from 100-300 µm [8]. The major advantage of this laser is the failure of implants to absorb its energy as it reflects away from the metal surfaces. Though, CO2 laser does not alter the implant surface, it’s not the instrument of choice for osseous procedures as it has the potential to cause thermal changes to bone [6].
Erbium family
Two specific wavelengths that uses erbium are Er,Cr:YSGG lasers that employs a solid crystal of yttrium- scandium-gallium-garnet doped with erbium and chromium as the active medium and has wavelength of 2,780nm and Er:YAG lasers, uses a solid crystal of erbium doped yttrium-aluminium-garnet as an active medium and has the wavelength of 2,940nm [8]. These wavelengths have high empathy for hydroxyapatite and water [8] therefore, it is the laser of choice for hard tissues [3] and as our oral mucosa has approximately 90% of water hence, it can also be used for the soft tissue procedures. Thus, making it an “ALL-TISSUE LASER”. It is used for tissue retraction for uncovering implants. They are similar to CO2 is some respects that there is minimal depth soft tissue penetration and reflection away from the implant surface. These lasers do not have hemostatic capability similar to CO2 and Nd:YAG lasers [6].
Ho: YAG
It is holmium and thulium doped YAG laser having the wavelength of 2,100nm. It is absorbed by water 100 times greater than that of the Nd: YAG laser and does not react with haemoglobin or other tissue pigments. Hence, it is employed for ablating hard calcified tissues at high peak powers and for TMJ arthroscopy in oral surgery [8]. In addition to Nd: YAG laser, they are also contraindicated for decontamination of ailing implants surfaces at any power output [6].
Application of Lasers in Implantology
Removal of Granulation Tissue
Removal of granulation tissue and disinfection of the surgical site after extraction is one of the most important uses of lasers in implantology. The perfect tool for this can be Erbium lasers as it does not cause mechanical or thermal trauma to the bone and the procedure can be performed with the greater comfort to the patient while disinfecting the surface , since no force is applied, unlike with curettes. Following, this a diode or Nd: YAG lasers can also be used for deep disinfection. The penetration of these laser energies in hydroxyapatite and absorption by bacterial pigments are advantageous thus, can have a Biomodulation or Low level laser therapy effect, that aids in healing and causes less oedema and pain to the patient [17, 18].
Peri-implantitis
Peri-implantitis is characterized as a rapidly progressive failure of osseointegration. The success rate of an implant is determined by many factors, out of which one of the most important is the maintenance of the peri- implant area. With objective in mind of avoiding deleterious alteration on the implant surface during routine maintenance procedures or in the treatment of ailing implants, the Nd:YAG laser was a possible modality for detoxifying, debriding and sterilizing the surface of the implant but it has been found that when Nd:YAG laser is used at 0.3, 2.0 or 3.0 watts it results in surface melting, porosity and other alteration of the implant surfaces including physical changes in the crystalline structure of the hydroxyl apatite coating. Thereby, contraindicating its use for treatment of peri-implantitis & hyperplasia of surrounding gingival tissues [14]. The laser systems that can be effectively used for decontamination of the implant surface are diode lasers alone or with toludine O dye, CO2 lasers (Figure 3) and Er:YAG lasers, because of their bactericidal effect and technical simplicity [14]. Debridement of implant abutment surface with lasers can effectively decontaminate the surfaces, reduce the bacterial count (Photodynamic therapy) and improve the success rate of ailing implants. It has been documented that even at low energy densities, the Er: YAG laser had a high bactericidal potential on common implant surfaces. Thus, can be a novel technical modality for the debridement of implant abutment surface [19, 20].
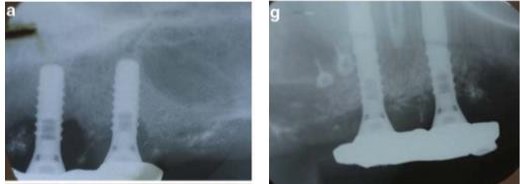
Figure 3a): Radiograph showing crestal bone loss around the two implants.
Figure 3b): Radiological examination 8 months after peri-implantitis therapy using CO2 laser, shows the new bone formation around the failing implants and the stable result [21].
Second – Stage Recovery of Implants
According to the laser tissue characteristics, all laser wavelengths can be employed for the second stage recovery of implants, provided care is exercised to avoid contact with the implant body. Using lasers for tissue ablation leads to precise and predictable healing with minimal shrinkage of the tissue so that the impressions can be taken immediately after the procedure without delay [18, 22]. Laser systems those can be used for this procedure are Diode, Erbium group & CO2 at the suggested energy levels of 1-2W, 200-250mJ/10 pps & 1- 2 W respectively. The prime advantages of using laser for this procedure are haemostasis, superior accessibility, and production of the protective coagulum as an aid to healing and patient comfort [22]. Though Nd: YAG can be used for uncovering the implants but the issue of concern is the transmission of the heat to the bone from the heated implant surface and its ability to alter the implant surface [6] (Figure 4).
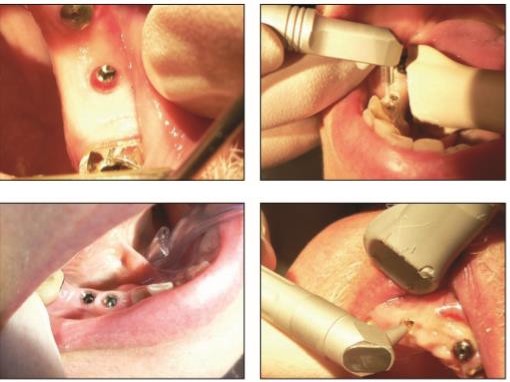
Figure 4a: Soft tissue healing at 10 days. Figure 4b: Implants uncovered using Er: YAG (2,940 nm) laser without water spray. Figure 4c: Healing at one week. Figure 4d: Second stage recovery using CO2 laser (10,600 nm) [22].
Sinus Lift Procedure with Implant Placement
Sinus lift elevation using bone grafts is a popular and scientifically documented method of bone augmentation and is performed in cases with reduced bone height followed by implant placement. It is relatively an extensive surgical procedure and is associated with adequate postoperative morbidity of the patient especially in the cases performed using conventional scalpel technique [23]. The procedure can be carried out by making the lateral osteotomy with a decreased incidence of sinus membrane perforation & Er, Cr: YSGG is the optimum choice for this. Also, it has been demonstrated that bone grafts done using lasers decrease the amount of bone necrosis from the donor site and the osteotomy cuts are narrower, resulting in less postoperative pain and edema [24]. Er, Cr: YSGG is a valuable tool in open sinus lift surgery when used at recommended parameters [23].
Laser Assisted Osteotomy
The use of conventional drills for osteotomy have several disadvantages like anxiety and discomfort to patient, undue pressure application on the bone, difficulty in getting the coolant between the drill and the bone and excessive bleeding during the procedure. This can increase the risk for developing postoperative complications. Hence, these can be overcomed with the use of lasers, as no pressure is exerted on bone while performing osteotomy with them. Er:YAG is a safe option for use in osteotomy procedures and when compared with CO2 laser (9.6 µm) and conventional drill, Er:YAG lasers require lower power and causes a smaller temperature rise than mechanical tools [5]. Laser assisted osteotomy is also beneficial for patients with potential bleeding problems, to provide essentially bloodless surgery in the bone [1, 2].
Laser as a Hemostatic Tool
A large proportion of the patients is aware about implants and desires their placement. These patients include those are on long term anticoagulant therapy or other systemic medical problems and could benefit from a quick and effective hemostasis; therefore, the use of laser in this aspect is being evaluated especially for better blood clot stabilization in the surgical site. According to the laser-tissue interactions the best hemostatic effect of the lasers is associated primarily with the Nd: YAG (deep soft tissue penetration) and diode lasers followed by CO2 and erbium lasers. The use of Nd: YAG laser with a hand piece has been deemed effective in bringing about hemostasis. In addition to this when bare laser technique followed by a pulsed laser is used, the thermal effects are reduced and intra-alveolar application of pulsed Nd: YAG laser energy is considered safe [5].
Intraoral Welding
The most peculiar of the osseointegration technique is a passive fit of the prosthesis on the implants when it has to be placed on multiple implants. The conventional casting techniques can lead to the expansion or contraction of the metal thereby jeopardising the passive fit of the prosthesis. For this purpose, Nd:YAG lasers are the tool of choice as they have the ability to alter the metallic surfaces and weld dental alloys [6]. Several advantages of laser welding include strong laser-welded joints; localized heat production, thus avoiding expansion and distortion; eliminates the need to fabricate a refractory cast and welding can be performed in close proximity with acrylic resin or ceramics [25]. Hence, the laser-welded framework exhibits a more precise fit than the onepiece casting [26].
Laser Microtextured Implant Collars
Nowadays, laser microtexturing of the implants is being carried out to improve and maintain the integration at the bone implant interface as it helps in controlling cell attachment proliferation and differentiation [27].
Risks Associated With Laser Use
Laser Beam Risks
These risks are posed when non-target tissues are exposed to laser beams and because of the high intensity and ability of lasers to produce very high concentrations of optical power at considerable distances, serious injuries to the eyes and skin can be caused.
Ocular Injuries
Most of them are caused due to operator error. Two groups of wavelengths that can adversely affect the eye are: 400–1,400 nm (visible and near infrared): passes through the transparent structures in front of the eye and causes retinal injuries, selectively destroys red or green cones, resulting in color blindness. 2,780–10,600 nm (mid-to far infrared): causes corneal injuries as they mainly effects the non-pigmented structures towards the front of the eye. Retinal injuries are more damaging than the corneal injuries and are not noticed at the initial stages due to lack of pain receptors thus, have a little scope of repair. The focusing ability of the eye lens makes 1 mW laser beam to pass at the back of the eye resulting in the retinal irradiance of more than 300 W/cm2 that is well above the ablation threshold. Potential injury to the eye can occur either by direct emission from the laser or by reflection from a specular (mirror like) surface or highly polished, convex curvature instruments. To avoid this, use of carbonized and non-reflective instruments has been recommended. All persons within the controlled area must wear appropriate eye protection glasses, which must have an optical density of 4, during laser emission. The selected eyewear should be free of any scratches or damage and constructed with side protection/shields to protect the eyes from reflective laser energy [8].
Tissue Injuries
Thermal interaction of radiant energy with tissue proteins results in Laser - induced damage to skin and others non-target tissues. Temperature elevation of 21°C above normal body temp (37°C) can produce cell destruction by denaturation of cellular enzymes and structural proteins. Tissue damage can also occur due to cumulative effects of radiant exposure. These type of tissue damages are termed as photodisruption and photoplasmolysis [28].
Non Beam Risks Include
Respiratory problems: The potential inhalation of the airborne biohazardous materials released by vaporisation of the cellular components due to the rapid heating of the water content of the tissues, involves the another class of hazards. During ablation or incision extremely small fragments of carbonized, partially carbonized, and relatively intact tissue elements are violently projected into the area, leading to the formation of airborne contaminants that are observed clinically as smoke and is known as LASER PLUME. The effect of plume inhalation can be serious and cause nausea, breathing difficulties and distant inoculation of bacteria. A particle of approx. 5nm in size is filtered out by the standard surgical masks, whereas the size of the particles in laser plume may be as small as 0.3nm therefore, use of suitable fine mesh face masks and evacuation of the laser plume is indicated [28]. Fire and explosion: The use of flame resistant material is highly recommended within the clinical settings as flammable solids, liquids and gases can easily be ignited if exposed to laser beam (eg. Ignition of tubing, anaesthetic gases or chemicals including alcoholic disinfectants) [28]. Electrical hazards: These hazards include Electrical shock hazards & Electrical fire or explosion hazards and can occur due to the moveable components of a laser, electrical shock and mains supplies (pressurized air, water) [28].
Limitations of Lasers
a) Requires special training and education for various clinical applications and types of lasers. b) Requires high cost required to purchase equipment and implement technology c) More than one laser may be needed as different wavelengths are required for various procedures [4].
Conclusion
From this wide range of laser applications, it is evident that the use of laser technology is well documented and promising in implant dentistry when correct laser wavelength and power settings for soft and hard tissue are being applied. There is no doubt, that thorough knowledge of the laser physics in association with laser tissue interactions and training should be a prerequisite to use lasers efficiently in daily practice. Having this knowledge about laser wavelengths, the lasers may be used to treat peri-implantitis, to manage periimplant inflammatory reactions leading to progressive bone loss with implant failures and possibly to improve osseointegration. As Aaron rose says ‘In right light at right time everything is extraordinary’.
References
-
Durrani S (2015) Laser and its Application in Prosthetic Dentistry. Int J Dent Med Res 1(6): 183- 188.
-
Nachrani P, Srivastava R, Palekar U, Choukse V (2014) Lasers in Prosthodontics- A Review. Nat J Dent Sci and Res 1(2): 74-77.
-
Mishra MB, Mishra S (2011) Lasers and its Clinical Applications in Dentistry. Int J Dent Clin 3(4): 35-38.
-
David CM, Gupta P (2015) Lasers in Dentistry: A Review. International Journal of Advanced Health Sciences 2(8): 7-13.
-
Romanos GE, Gupta B, Yunker M, Romanos EB, Malmstrom H (2013) Lasers Use in Dental Implantology. Implant Dent 22(3): 282-288.
-
Martin E (2004) Lasers in dental implantology. Dent Clin N Am 48: 999-1015.
-
Spitz SD Lasers in Prosthodontics: Clinical realities of a Dental Laser in a Prosthodontic practice. Alpha Omegan 101(4): 188-194.
-
Bhat AM (2010) Lasers in Prosthodontics - An Overview Part 1: Fundamentals of Dental Lasers. J Indian Prosthodontic Society 10: 13-26.
-
Mohammadi Z, Jafarzadeh H, Shalavi S, Kinoshita JI, Giardino L (2017) Lasers in Apicoectomy: A Brief Review. J Contemp Dent Pract 18(2): 170-173.
-
Jyoti N, Pankaj M, Tulika G, Shelly A (2010) Dental Lasers - A Boon To Prosthodontics- A Review. IntJ Dent Clin 2(2): 13-21.
-
Bali SK, Naqash TA, Abdullah S, Mir S, Nazir S, et al. (2012) Application of Lasers in Prosthodontics. Int J Clin Dent Sci 3(2): 66-70.
-
Oregon state university Laser types and classification. Ehs.oregonstate.edu.
-
Walsh LJ (1992) The use of lasers in implantology: an overview. J Oral Implantology 18(4): 335-340.
-
Block CM, Mayo JA, Evans GH (1992) Effects of the Nd:YAG dental laser on plasma-sprayed and hydroxyapatite-coated titanium dental implants: surface alteration and attempted sterilization. Int J Oral Maxillofac Implants 7(4): 441-449.
-
Chu RT, Watanabe L, White JM, Marshal GW, Marshal SJ, et al. Temperature rises and surface modification of lased titanium cylinders. J Dent Res 71(Spec Iss): 144.
-
Sawisch TJ, Strauss RA (2016) Uses of lasers for minor oral surgery in general practice. Principles and Practice of Laser Dentistry 2nd (Edn.).
-
Maden I, Kazak Z Lasers in implantology.
-
Maden I, Kazak Z (2012) Lasers in oral implantology pp: 34-36.
-
Kreisler M, Kohnen W, Marinello C, Götz H, Duschner H, et al. (2002) Bactericidal Effect of the Er:YAG Laser on Dental Implant Surfaces: An In Vitro Study. J Periodontol 73(11): 1292-1298.
-
Matsuyama T, Aoki A, Oda S, Yoneyama T, Ishikawa I (2003) Effects of the Er:YAG Laser Irradiation on Titanium Implant Materials and Contaminated Implant Abutment Surfaces. J Clin Laser Med Surg 21(1):7-17.
-
Romanos GE, Gutknecht N, Dieter S, Sculean A (2009) Laser wavelengths and oral implantology. Lasers Med Sci 24(6): 961-970.
-
Parker S (2007) Surgical laser use in implantology and endodontics. Br Dent J 202(7): 377-386.
-
Titsinides S, Markopoulos G (2016) Er,Cr:YSGG Laser- Assisted Sinus Lift Surgery and Implant Placement. A Case Report. J Dent Health Oral Disord Ther 4(3): 00111.
-
Lukram A, Sachdeva N, Sahu K, Yadav A (2014) Application of Laser in Prosthetic Dentistry: A Review. Int J Dent Med Res 1(4): 99-102.
-
Forniani C, Merigo E, Cernavin I, Castro Lòpez de G, Vescovi P (2012) Intraoral Laser Welding (ILW) in Implant Prosthetic Dentistry: Case Report. Case reports in dentistry 2012: 839141.
-
Reidy SJ, Lang BR, Lang BE (1997) Fit of implant frameworks fabricated by different techniques. J Prosthet Dent 78(6): 596-604.
-
Weiner S, Simon J, Ehrenberg DS, Zweig B, Ricci JL (2008) The effects of laser microtextured collars upon crestal bone levels of dental implants. Implant Dent 17(2): 217-228.
-
Kaura S, Wangoo A, Singh R, Kaur S (2015) Lasers in prosthodontics. Saint Int Dent J 1(1): 11-15.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells