Predictable 3D Bone Reconstruction and Implant Restoration with Full Digital Workflow in Aesthetic Zone
Implant restoration in anterior maxilla often present a challenging dilemma to both surgeons as well as restorative dentists. Several factors influence the outcome of the case such as available residual bone, soft tissue type, restorative space, smile line, and implant position. Careful implant planning and placement play a critical role for successful implant therapy. The presence of good bone support is often scarce in the anterior maxilla Bone resorption due to peri-apical or periodontal infections and in case of delayed implantation, there is often the need for bone augmentation procedures especially in the aesthetic zone. Bone augmentation procedures advocated in literature demonstrate a variable success rate in achieving predictable bone volume. This case report of a 30-year-old male presents an endodontically failing central incisor, with inadequate surrounding bone (Seibert class 3) demonstrating both horizontal and vertical bone defect. Rehabilitation was carried-out by bone augmentation using autogenous cortical bone harvested from the ramus in combination with Xeno bone particles. On maturation this is followed by guided implant insertion and immediate Cad-cam restoration, following a full digital workflow. Final Restoration was given after 6 weeks. Conclusion: Bone augmentation using a thin autogenous bone plate stimulates revascularization and accelerates graft regeneration. The Xeno particles help in maintaining the volume during the remodelling stage. Complete digital workflow with guided implant placement and immediate prefabricated restoration provides accuracy for an aesthetic outcome besides reducing overall treatment time and patient acceptance. The customized BioHpp one-time abutment provides softer loading of the implant and maintains 3-dimensional bone volume and provides good soft tissue stability. The author advocates the described treatment workflow for such complex cases as it demonstrates reliable and predictable treatment outcome.
Introduction
Implant restorations have become the preferred choice of treatment for restoring a single or multiple teeth as compared to fixed partial dentures [1]. Loss of teeth due to trauma or pathology is accompanied by significant bone loss within the first three years and can be aggravated in presence of pre-existing endodontic or periodontal infection. Bone resorption is a biological phenomenon and cannot be prevented by the immediate implant placement [2, 3] alone. These clinical situations require additional bone augmentation to create bone volume to be able to place dental implants in an ideal position for an esthetic outcome. The most described techniques in the dental literature are: Guided Bone Regeneration (GBR), Distraction osteogenesis, Ridge splitting and inter-positional inlay grafting technique [4, 5, 6]. GBR which is a commonly advised procedure, entails the use of a barrier membrane to isolate bone defects and thus allows bone regeneration without interference from surrounding tissues. However, the uncertain resorption rate of collagen membrane often leads to a compromised clinical result [7, 8, 9, 10]. Khoury [11] in 2007 advocated a technique for grafting the alveolar ridge using thin cortical plates harvested from the ramus. Although this method has shown great success, the technique has disadvantages due to the need for a second surgical site, donor site morbidity, and being technique sensitive [11, 12, 13, 14, 15]. In the present case report a failing maxillary central incisor, with endodontic pathology, is rehabilitated with GBR- (a combination of the autogenous bone plate with Xeno bone particles & barrier membrane), followed by a full digital implant restoration workflow.
Case Presentation
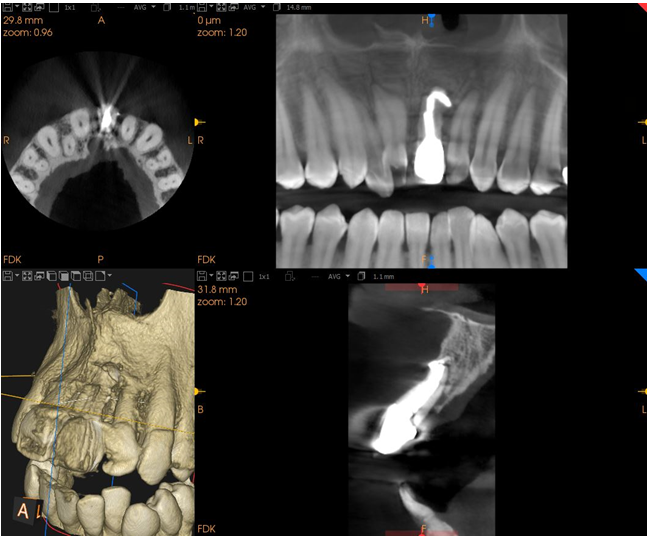
A 30-year-old young male presented with pain and mobility in a root canal treated maxillary left central incisor. Patient was unhappy with the re-cession of the anterior gingiva and presented a concern about it and wanted to explore the possibilities of fixed restoration using a dental implant. His medical history revealed no known drug allergies nor any medical health conditions. His expectations were reasonable, social history indicated that he was a non-smoker. Esthetic risk analysis revealed overall high- risk profile [16]. CBCT scan exhibited periapical pathology with inadequate bone availability for implant placement in the desired position (Figure 1). These findings suggested poor prognosis of the tooth and extraction was advised. Rehabilitation with implant supported prosthesis was agreed upon. Pre-implant surgery to augment the area with ramus cortical bone plate in combination with Xeno- bone particles and membrane was planned as phase 1of treatment. Tooth supported bonded provisional restoration was planned during this phase [15, 16, 17]. After 4-6 months of healing period guided implant placement and immediate CAD-CAM provisional was planned [18, 19, 20].
Preoperative CBCT of the mandible revealed inferior alveolar nerve canal at 7-10 mm from the buccal cortex indicating safe site for harvesting a bone plate from ramus. The surgical procedure was carried out under local anaesthesia (lignocaine with Adrenaline1:80,000) and antibiotic cover (amoxicillin plus clavulanic acid 625 mg) starting 1 hour before surgery. A mucoperiosteal flap exposing the underlying bone was raised by making sulcular incision from Right central incisor to left lateral incisor, followed by two vertical releasing incisions preserving the adjacent papilla (Figure 2a). The vertical and horizontal bone defect demonstrated Seibert class 3 situation (Figure 2b) [21].

Figure 2a: Sulcular incision design with vertical release on adjacent teeth.

Figure 2b: Full thickness flap elevation showing Siebert class 3 bone defect.
Donor Site
Cortical bone plate was harvested from right ramus area. A muco-periosteal flap was raised through an extension of the commonly used envelope flap from the mandibular body, exposing the third molar area and the buccal plate of the ramus and 1mm of trapezoidal osteotomy was performed along the external oblique ridge of the ramus using a saw PIEZOTOME™Cube, (Aceteon, India). A gentle tap with a chisel parallel to the length of osteotomy harvested the thin segment of cortical bone plate (Figure 3). The donor site was packed with an absorbable gelatin sponge (Hemocollagene, Septodont, UK) and the flap was repositioned with interrupted sutures using 4-0 vicryl suture (Ethicon, Johnson, and Johnson Pvt Ltd, India).

Recipient Site
The maxillary central incisor was extracted, and the site carefully curetted and disinfected using Photodynamic therapy-PDT (Helbo, Bredent medical, Gmbh) [22]. This involves the use of a low wavelength diode laser exposed to a photosensitive dye (methylene blue containing methylthioninium hydrochloride, 3,7-bis phenothiazine-5- ium chloride) for its activation which promotes the killing of periodontal pathogens. The harvested cortical plate was trimmed to fit the recipient site and anchored using a long fixation titanium screw (stoma®, Germany) and layered with Xeno bone particles (Geistlich Bio-Oss®) slow resorbing, to compensate for bone resorption during remodelling stage (Figure 4). A barrier membrane 13x25mm (Geistlich Bio-Gide®) was used to cover the site and stabilized under the labial and palatal tissue. The mucoperiosteal flap was mobilized by a sulcular periosteal cut and tension free closure achieved using vertical mattress and interrupted 4-0 vicryl sutures (Ethicon, Johnson, and Johnson Pvt Ltd, India).

CAD-CAM PMMA provisional crown with an ovate design was digitally designed using the pre-operative intra-oral scan (CS 3600, carestream, India, LLC) for a good emergence profile and bonded to the adjacent teeth (Figure 5). 17 CBCT scan after 4 months demonstrated the regeneration of the alveolar ridge along with adequate bone density (Figure 5).

Guided Implant Placement
After 4 months of healing, digital implant planning for 4x16 mm blueSKY implant (bredent medical, GmbH) and guide designing was done using coDiagnostix software (Dental wings, GmbH, Chemnitz, Germany). A 3D printed surgical guide was fabricated. Guided Implant placement was performed using bredent pro-guide system and a placement Torque of > 45Ncm was achieved with implant stability quotient (ISQ) of 65 (Penguin RFA, Sweden) (Figures 6a, 6b). Immediate implant restoration was done with one-time abutment protocol, BioHPP SKY elegance 15 degree (bredent medical, GmbH) and prefabricated CAD- CAM provisional crown (BreCAM Multicom, bredent medical GmbH) for softer implant loading (Figures 7a, 7b) [23, 24, 25].
Figure 6a: Static guided surgical implant placement.
Final abutment torqued to 25 Ncm and provisional crown luted using light cure temporary resin cement (tempo- link clear, Detax©). Soft tissue conditioning with proximal contacts was done to allow adequate papillae formation using Tarnow’s principle [26].
Figure 6b: Bredent blue sky implant In-situ, flapless surgery.
Figure 7a: Ceramic modified PEEK (Bio-Hpp abutment, Bredent Sky Elegance).
Figure 7b: Implant supported CAD PMMA prosthesis in situ- Papillae contouring.
Final Restoration
8 weeks later, an abutment level intra-oral scan (IOS) was made using CS 3600 scanner (Carestream Dental LLC, India). The emergence profile of the provisional crown, the contoured peri-implant mucosa, adjacent teeth on the maxilla, corresponding opposite arch, and the bite registration was all captured. Based on the STL file from the IOS, a full-contoured cement-retained E-max crown was designed and CAD/CAM milled without any physical models. Inter-proximal and occlusal contacts were defined virtually according to the threshold settings of the dental design software and superimposition of the customized pro-visional crown. This Emax crown was bonded over the ceramic modified PEEK abutment (Sky elegance Bio-Hpp abutment, bredent medical, GmbH) using Visio link primer & combolign resin cement (bredent medical, GmbH) (Figures 8a & 8b).

Figure 8a: Cement Retained Definitive Emax crown.
Figure 8b: Final Restoration.
Follow-up
Recall appointments were made at 6 months intervals, the implant remained stable, and the peri-implant gingiva was pink and healthy without bleeding on probing. CBCT scan was made for the assessment of marginal bone levels on the mesial and distal sides of the implant, which exhibited stable bone levels without any peri-implant radiolucency during the 1year follow-up period (Figure 8).
Discussion
Guided Bone Regeneration (GBR) is a method of enhancing bone growth by preventing soft-tissue ingress using a resorbable or non-resorbable barrier membrane thereby achieving bone regeneration. Several techniques have been advocated in literature, however many of them remain unpredictable especially for larger and vertical bone defects [8, 9, 10, 11]. Vertical augmentation procedures are challenging in the aspect of 3D reconstruction of the defect and securing the transplant for stable integration. Non-resorbable membrane in combination with bone substitute material is a commonly described procedure in literature, however a common complication is the exposure of membrane and the need for its removal which has a detrimental effect on the outcome [9]. Alternatively Autogenous bone plates with fixation screws provided good stability of the transplant ensuring integration and lesser tissue irritation compared to GBR techniques using membrane [11, 14]. The augmentation technique used in the case report may be easily altered according to the morphological bone defect. Clinical study by Khoury Fouad and Thomas H demonstrated that 97.89% of patients presented with low or moderate pain perception with low complication rate during the process of bone harvesting suggesting higher reproducibility and predictability of the procedure [15].
Guided implant surgery allows a minimal invasive procedure without the necessity to elevate a flap, thereby maintaining vascularization over the grafted bone. This allows soft tissue to be in immediate contact with its natural surface thereby assisting faster healing and a stable reattachment of the tissue with the underlying surface [18].
Furthermore, frequent removal and insertion of the healing abutment is associated with increased crestal bone loss [19, 24]. Romanos, et al. suggested placement of the final abutment immediately after the surgical implant placement (“one-abutment at one-time” protocol) to significantly reduce crestal bone loss [20]. José Eduardo Maté also reported that the use of Bio-HPP abutment in combination with guided surgery and immediate restoration provides softer loading of the implant resulting in stable crestal bone and peri- implant tissue [23, 24, 25]. In clinical comparison to the results perceived in the present case report for three-dimensional reconstruction and implant rehabilitation in the esthetic zone, a similar result could be achieved with various other techniques described in the literature, However, the proposed protocol seems to be associated with fewer complications such as marginal bone loss, dehiscence, infection and allows a significant reduction in treatment time.
Summary
This retrospective case observation exhibited predictable results for the management of challenging implant restorative cases with horizontal and vertical bone defects in esthetic zones while maintaining healthy peri-implant tissue. Autogenous bone augmentation and a full digital implant workflow aided in overall reduction of treatment time, improved esthetic and stable peri-implant tissue; thus the author advocates the treatment workflow for management of such complex cases in esthetic zone.
References
-
Alzahrani KM (2020) Implant bio-mechanics for successful implant therapy: A systematic review. J Int Soc Prev Community Dent 10(6): 700.
-
Araújo MG, Sukekava F, Wennström JL, Lindhe J (2006) Tissue modeling following implant placement in fresh extrac-tion sockets. Clin Oral Implants Res 17(6): 615- 624.
-
Duncan JM, Westwood RM (1997) Ridge widening for the thin maxilla: a clinical report. Int J Oral Maxillofac Implants 12(2): 224-227.
-
Elian N, Jalbout Z, Ehrlich B, Classi A, Cho SC, et al. (2008) A two-stage full-arch ridge expansion technique: review of the literature and clinical guidelines. Implant Dent 17(1): 16-23.
-
Guirado JLC, Yuguero MRS, del Valle MRC, Zamora GP (2005) A maxillary ridge-splitting technique followed by immediate placement of implants: a case report. Implant Dent 14(1): 14-20.
-
Hämmerle CHF, Jung RE, Feloutzis A (2002) A systematic review of the survival of implants in bone sites augmented with barrier membranes (guided bone regeneration) in partially edentulous patients. J Clin Periodontol 29: 226- 231.
-
Buser D, Brägger U, Lang NP, Nyman S (1990) Regeneration and enlargement of jawbone using guided tissue regeneration. Clin Oral Implants Res 1(1): 22-32.
-
Dahlin C, Linde A, Gottlow J, Nyman S (1988) Healing of bone defects by guided tissue regeneration. Plastic Reconstr Surg 81(5): 672-676.
-
Von Arx T, Broggini N, Jensen SS, Bornstein MM, Schenk RK, et al. (2005) Membrane durability and tissue response of different bioresorbable barrier membranes: a histologic study in the rabbit calvarium. Int J Oral Maxillofac Implants 20(6): 843-853.
-
Zakhary IE, El Mekkawi HA, Elsalanty ME (2012) Alveolar ridge augmentation for implant fixation: status review. Oral Surg Oral Med Oral Pathol Oral Radiol 114(5): 179- 189.
-
Fouad K, Khoury C (2007) Mandibular bone block grafts: diagnosis, instrumentation, harvesting techniques and surgical procedures. Bone Augmentation in Oral Implantology Berlin: Quintessence.
-
Marco E, Grusovin MG, Felice P, Karatzopoulos G, Worthington HV, et al. (2010) The efficacy of horizontal and vertical bone augmentation procedures for dental implants: a Cochrane systematic review. Evidence-based practice: Toward optimizing clinical outcomes pp: 195- 218.
-
Marco E, Grusovin MG, Felice P, Karatzopoulos G, Worthington HV, et al. (2009) Interventions for replacing missing teeth: horizontal and vertical bone augmentation techniques for dental implant treatment. Cochrane Database Syst Rev 4: CD003607.
-
Peck MT (2015) Alveolar ridge augmentation using the allograft bone shell technique. J Contemp Dent Pract 16(9): 768-773.
-
Fouad K, Hanser T (2015) Mandibular bone block harvesting from the retromolar region: a 10-year prospective clinical study. Int J Oral Maxillofac Implants 30(3): 688-697.
-
Martin WC (2006) Diagnostic factors for esthetic risk assessment. Implant Therapy in the Esthetic Zone- Single-Tooth Replacements pp: 11-20.
-
Wang WCW, Hafez TH, Almufleh AS, Ochoa DD, Manasse M (2015) A Guideline on provisional restorations for patients undergoing implant treatment. J Oral Bio 2(2): 7.
-
Nadine B (2009) Flapless surgery and its effect on dental implant outcomes. Int J Oral Maxillofac Implants 24: 118-125.
-
Ana M, Sánchez IS, Martín C, Blanco J, Sanz M (2017) The effect of one‐time abutment placement on interproximal bone levels and peri‐implant soft tissues: A prospective randomized clinical trial. Clin Oral Implants Res 28(4): 443-452.
-
Romanos GE, Traini T, Johansson CB, Piattelli A (2010) Biologic width and morphologic characteristics of soft tissues around immediately loaded implants: studies performed on human autopsy specimens. J Periodontol 81(1): 70-78.
-
Seibert JS (1983) Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts, Part I. Technique and wound healing. Compend Contin Educ Dent 4(5): 437-453.
-
Umberto R, Nardi GM, Libotte F, Sabatini S, Palaia G, et al. (2016) The antimicrobial photodynamic therapy in the treatment of peri-implantitis. Int J Dent 2016: 7692387.
-
Atef YA, Korsel AM, Tokhey E, Mohamed H, Ali KM, et al. (2020) The effect of different implant abutment materials on the stress distribution to the bone implant contact. Egyptian Dent J 66(2): 1289-1294.
-
Marco D, Nardi D, Piattelli A (2011) One abutment at one time: non‐removal of an immediate abutment and its effect on bone healing around subcrestal tapered implants. Clin Oral Implants Res 2(11): 1303-1307.
-
de val JEMS (2019) A safe and predictable long-term treatment protocol. EDI Journal 2: 60.
-
Tarnow DP, Magner AW, Fletcher P (1992) The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. J Periodontol 63(12): 995-996.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells