Evaluation of Exhaled Carbon Monoxide Levels in Smokers and Non-Smokers-A Comparative Study
Background: Cigarette smoke causes both acute and chronic changes of the immune system. Carbon monoxide (CO) exhaled through breath of an individual is an easiest, immediate and non-invasive method to assess smoking status. Aim: The aim of the study is to compare the exhaled CO levels in smokers and non-smokers using portable CO monitor. Material & Methods: The exhaled CO levels were measured in 100 subjects (50 smokers, 50 non-smokers) who were examined during the OPD. Exhaled CO concentration was measured using the Micro+ Smokerlyser. Results: The mean carbon monoxide in the smokers was 6.34 PPM and the mean carbon monoxide in non-smokers was 1.26 PPM. There was statistically very highly significant difference of mean CO among smokers and non-smokers (P<0.001). Conclusion: The exhaled CO levels successfully distinguished smokers from nonsmokers and it provides an easy and non-invasive mode of assessing a subject's smoking status. This will be beneficial for healthcare providers to examine the effectiveness of tobacco cessation and prevention programs.
Introduction
Tobacco in the form of smoking is associated with a wide spectrum of many diseases including diabetes, hypertension, stroke, coronary artery disease, peripheral artery disease, gastric ulcer, and cancers of oral cavity, larynx, oesophagus, pancreas and bladder that leads to increase risk for morbidity and mortality worldwide. It is also causes major diseases like chronic obstructive pulmonary disease (COPD) and a risk factor for low-birth-weight babies. Annual mortality totals 8 million people, with 7 million of these fatalities directly attributable to tobacco usage [1, 2].
Smoking is a well-established risk factor for the development of a range of diseases [3, 4] including major cardiovascular diseases (CVD) [5, 6], chronic obstructive pulmonary disease [7, 8] and some cancers [9, 10]. Tobacco smoke contains a variety of chemicals which are known to be harmful to human health.
Free radicals, nicotine, and carbon monoxide (CO) are believed to be the most important for pharmacological actions [11]. Smoking boosts the level of CO in the blood, which may lead to several cardiovascular diseases. The measurement of exhaled CO level is an immediate, non- invasive or easiest method of assessing smoking status, although other sources of pollution including exhausts gases which causes elevations in the fractional concentrations of CO in expired air [12, 13].
Therefore, the aim or objective of this study is to compare the exhaled CO levels in established smokers and non- smokers and to investigate factors that may affect breath CO levels or exhaled CO levels.
Method
In the light of above literature present study was undertaken to compare smokers and non-smokers. Study consisted of 100 subjects who visited Al Badar Dental College and Hospital during OPD hours. The subjects were informed of the purpose of the Smokerlyser and were reassured that the results were confidential in order to encourage accurate reporting of smoking habits. Background information about their health, age, gender, smoking habits, frequency of smoking. The subjects who have minimal respiratory symptoms included. The subjects were detected only by means of clinical questioning, and were commonly considered to be normal among smokers. All subjects were asked to provide one breath into Smokerlyser.
Exhaled CO concentration was measured using the the Micro+ Smokerlyser. Micro+ Smokerlyser is reported to correlate closely with blood carboxyhaemoglobin concentration in smokers and in non-smokers, and it is an inexpensive, portable CO monitor [9, 12]. The subjects are asked to exhale completely, inhale fully, and then hold their breath for 15 s before exhaling rapidly into disposable mouthpiece which help to standardize the breath analysed by smokerlyzer. The subjects who have minimal respiratory symptoms included which were detected only by means of clinical questioning, and were commonly considered to be normal among smokers. Finally, all subjects were asked to provide one breath into Smokerlyser.
Statistical Data Analysis
Statistical analyses were done by IBM SPSS 20.0 version software. Collected data were spread on excel sheet and prepared master chart. Through the master chart tables and graphs/diagrams were constructed. For quantitative data analysis t-test was applied for statistical significance. If P-value is less than 0.05 considered as significant.
Results
Exhaled CO was detectable in all subjects. Ambient air concentrations of CO were at 0–18 ppm level during the measurements. Breath CO levels were assessed in a total of 100 subject; 50 of them were smokers 9), 50 of them was non-smokers.
For the smokers, the mean daily consumption of cigarettes was 19.79±9.04 cigarettes/d and all of them reported that they had smoked on the day of testing.
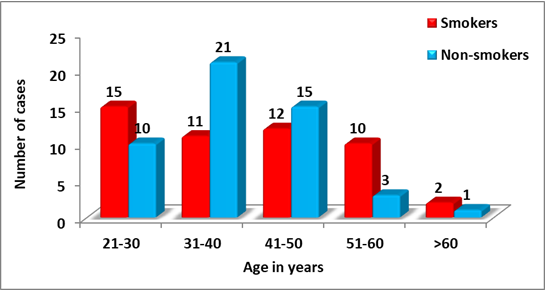
The mean age of all smokers and non-smokers is 38.83 years, the mean age of smokers is 39.56 years and mean age of non-smokers is 38.10 years. There was no statistical significant difference of mean age of smokers and non- smokers (P>0.05). In smokers all cases 50 (100.0%) cases are males and in non-smokers 26 (52.0%) cases are males and 24 (48.0%) cases are females as shown in Table 1 & Figure 1.
| Age in years | Smokers | Non-smokers | Total | |||
|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | |
| 21-30 | 15 | 30 | 10 | 20 | 25 | 25 |
| 31-40 | 11 | 22 | 21 | 42 | 32 | 32 |
| 41-50 | 12 | 24 | 15 | 30 | 27 | 27 |
| 51-60 | 10 | 20 | 3 | 6 | 13 | 13 |
| >60 | 2 | 4 | 1 | 2 | 3 | 3 |
| Total | 50 | 100 | 50 | 100 | 200 | 100 |
| Mean ± SD | 39.56 ± 12.51 | 38.10 ± 8.91 | 38.83 ± 10.71 | |||
| t-test value and P-value | t = 0.672 P = 0.503 NS |
Table 1: Age wise distribution of smokers and non-smokers.
NS= not significant, S=significant, HS=highly significant, VHS=very highly significant Table 1: Age wise distribution of smokers and non-smokers.
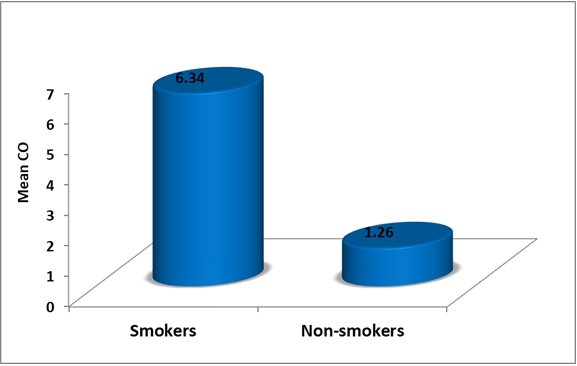
The mean carbon monoxide in the smokers was 6.34 PPM and the mean carbon monoxide in non-smokers was 1.26 PPM. There was statistically very highly significant difference Smokers 6.34 PPM 4.89 t = 7.161 P = 0.000 Non-smokers 1.26 PPM 1.08 VHS
- VHS=very highly significant
Table 2: Comparison of CO among smokers and non-smokers.
Discussion
There are various methods of assessing smoking status. Nicotine, cotinine, or thiocyanate levels in the plasma or of mean CO among smokers and non-smokers (P<0.001). The mean CO in smokers had observed significantly high as compare to non-smokers. As shown in Table 2 & Figure 2.
Groups Carbon Monoxide in PPM t-test value P-value and significance Mean Standard Deviation P-value urine may be used to asses smoking status. However, the blood tests are invasive and neither the blood nor the urine test provide an immediate assessment. The measurement of breath CO level is an immediate, non-invasive or easiest method of assessing smoking status [12].
This study supports that measuring breath CO levels provides an immediate, non-invasive, simple, and effective way of confirming a patient’s smoking status. Exhaled CO levels were higher in smokers than in non-smokers [12, 14]. Also in our study, the exhaled CO level with the Smokerlyser was significantly higher in smokers than non-smokers and the values of exhaled CO in smoking and non-smoking subjects were similar to those of previous study [1, 14]. There is direct relationship between the smoking status of a given individual and the concentration of carboxyhaemoglobin (COHb) in their blood [15, 16, 17].
Our results shown that exhaled CO levels may be used to distinguish smokers from non-smokers as same as the others. Our results shown that the optimal cut-off was 6.34
ppm, giving 90% sensitivity and 83% specificity. Similarly, Middleton and Morice [12] reported that the optimal cutoff was 6 ppm (selectivity 96%, sensitivity 94%). Jarvis, et al. [6] reported that the optimal cutoff was 8 ppm. Jarvis, et al. [6] shown that the second breath CO level was significantly higher than the first. In contrast Middleton and Morice [12] reported that the first breath CO level was significantly higher than the second and they recommended that a single Smokerlyser assessment should usually be sufficient, provided that there is adequate technique.
For this reason in present study exhaled CO levels were assessment with the first measurement. In a previous study it was stated that exhaled CO may be affected by ambient CO. In contrast, Zetterquist, et al. [13] study shown that ambient air did not affect the exhaled CO levels when subjects held their breath for 10s. Since there seems to be no contribution of CO from the conducting airways it must have its origin from the alveoli. Our results shown that there was a direct relationship between daily consumption of cigarettes and CO levels, and between duration of smoking and CO levels in smokers. The increase in CO concentrations after breath- hold also supports this view.
A standardized time of breath-hold of 15 s was used in all the experiments which should have been sufficient for equilibrium to take place [13]. Since we also ask to the subjects to hold their breath for 15s we did not consider the impact of ambient air.
In normal day to day life exposure of carbon monoxide occurs due to environmental pollution, occupational exposure, passive smoking but the common cause and higher levels of exposure due to smoking.
In clinical practice, it would be important to ensure the Smokerlyser was calibrated regularly. This was not a problem in this study because of the measurements were done in 5 days at the open air near the student healthy club desk after the Smokerlyser calibrated. Moreover, we think that exhaled CO level likely is not affected the ambient air because of the measurements were done at the open air.
Conclusion
Exhaled CO measurements may provide a non-invasive, sensitive, and immediate way of assessing a patient’s smoking status. CO measurement will replace at some stage the usual question regarding the number of cigarettes consumed. Moreover, exhaled CO level is recommended for evaluating the exposure of passive smoking. Determining of exhaled CO level more than 6.5 ppm strongly suggests that subject is a smoker.
References
-
World Health Organization, Pan American Health Organization. Tobacco control.
-
Oyapero A, Olatosi OO, Olagundoye O (2021) Are Nigerian oral health workers overlooking opportunities to promote interventions for tobacco smoking cessation? Popul Med 3(6): 1-7.
-
Malenica M, Prnjavorac B, Bego T, Dujic T, Semiz S, et al. (2017) Effect of Cigarette Smoking on Haematological Parameters in Healthy Population. Med Arch 71(2): 132- 136.
-
Caponnetto P, Maglia M, Prosperini G, Busà B, Polosa R (2018) Carbon monoxide levels after inhalation from new generation heated tobacco products. Respir Res 19(1): 164.
-
Selya AS, Hesse ND (2017) Time to first cigarette and serum cholesterol levels. Soc Sci Med 174: 213-219.
-
Jarvis MJ, Russell MA, Saloojee Y (1980) Expired air carbon monoxide: a simple breath test of tobacco smoke intake. Br Med J 281(6238): 484-485.
-
Goodwin RD, Lavoie KL, Lemeshow AR, Jenkins E, Brown ES, et al. (2012) Depression, anxiety, and COPD: the unexamined role of nicotine dependence. Nicotine Tob Res 14(2): 176-183.
-
Selya AS, Oancea SC, Thapa S (2016) Time to First Cigarette, a Proxy of Nicotine Dependence, Increases the Risk of Pulmonary Impairment, Independently of Current and Lifetime Smoking Behavior. Nicotine Tob Res 18(6): 1431-1439.
-
Doll R, Peto R, Boreham J, Sutherland I (2005) Mortality from cancer in relation to smoking: 50 years observations on British doctors. Br J Cancer 92(3): 426-429.
-
Hecht SS (1999) Tobacco smoke carcinogens and lung cancer. J Natl Cancer Inst 91(14): 1194-1210.
-
Acik DY, Suyani E, Aygun B, Bankir M (2020) The Effect of Smoking on Hematological Parameters. Ulutas Med J 6(1): 9-14.
-
Middleton ET, Morice AH (2000) Breath carbon monoxide as an indication of smoking habit. Chest 117(3): 758-763.
-
Zetterquist W, Marteus H, Johannesson M, Nordval SL, Ihre E, et al. (2002) Exhaled carbon monoxide is not elevated in patients with asthma or cystic fibrosis. Eur Respir J 20(1): 92-99.
-
Montuschi P, Kharitonov SA, Barnes PJ (2001) Exhaled carbon monoxide and nitric oxide in COPD. Chest 120(2): 496-501.
-
Jones RH, Ellicott MF, Cadigan JB, Gaensler EA (1958) The relationship between alveolar and blood carbon monoxide concentrations during breathholding. J Lab Clin Med 51(4): 553-564.
-
Ringold A, Goldsmith JR, Helwig HI, Finn R, Schoutte F (1962) Estimating recent carbon monoxide exposures. Arch Environ Health 5(4): 308-318.
-
Antuni JD, Kharitonov SA, Hughes D, Hodson ME, Barnes PJ (2000) Increase in exhaled carbon monoxide during exacerbations of cystic fibrosis. Thorax 55(2): 138-142.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells