Osteonecrosis of the Jaws due to Drugs: Series of Clinical Cases
Osteonecrosis of the jaw is a rare but severe condition manifested as necrotic bone lesion, it has been linked to the use of potent antiresorptive agents and antiangiogenic medication, in the absence of prior radiation treatment. Staging the pathology once installed, helps us to continue with the protocol guide and is essential to be able to apply the indicated therapy in each case. Clinical Relevance: The contribution of this work is for general dentist, in the observation and clinical management of patients at risk or with development of osteonecrosis of the jaw due to medication, through their staging
Introduction
Osteonecrosis of the jaw is a rare condition in which bone cells die due to various causes. It is classified into drug-induced osteonecrosis of the jaw, osteoradionecrosis, traumatic, non-traumatic, and spontaneous osteonecrosis.
Even though the vascularization of the jawbone is rich, the vessels have a terminal course, and this feature makes it fragile to traumatic and inflammatory injuries [1].
The medication-related osteonecrosis of the jaw (MRONJ) is an “adverse drug reaction described as the progressive destruction and death of bone that affects the mandible and maxilla of patients exposed to the treatment with medications known to increase the risk of disease, in the absence of a previous radiation treatment” [2].
Exposed bone, purulence, swelling, fistula, inflammation, and trismus were the most commonly reported clinical signs at diagnosis [3].
Some potential risk factors, including periodontal diseases, tooth extraction or dental implantation, and chemotherapy were reported to be associated with the occurrence of MRONJ [4].
Evidence has shown that immunity dysfunction is highly involved in the development of MRONJ, BP and risk factors that impact the mucosal immune system, coupled with bacterial infection contribute to the development of MRONJ. The results showed that the imbalance in oral flora may be a prerequisite for MRONJ and biological barriers are of great necessity to prevent the occurrence of MRONJ [5], previous studies have shown increased bacterial infiltration and inflammation at the necrotic site [6], BPs, on the one hand, can induce an immunosuppressive condition by suppressing immune cell activation, on the other hand, it can render an imbalance between anti-inflammatory and pro-inflammatory cytokines, thereby resulting in intense inflammation and tissue damage [7]. In addition to the direct toxic effect, BPs
also exert an inhibitory effect on wound healing by altering immune cytokines [8].
The type of BP used may affect the risk of MRONJ development. MRONJ incidence is considerably higher with IV BPs compared to oral BPs, largely because oral BPs are mostly used for benign diseases whereas IV BPs are used for malignancies, in much higher and more frequently administered doses [9].
Denosumab, is a receptor activator of nuclear factor kappa-B ligand (RANK-L), is an antiresorptive agent that exists as a fully humanized antibody against RANK ligand and inhibits osteoclast function and associated bone resorption. Among patients exposed to Denosumab, the risk for MRONJ was reported to be 0.3 percent, higher than for BPs [10].
To estimate the risk for medications associated with MRONJ, the primary parameter to be considered is the therapeutic indication for treatment (malignancy or osteoporosis/osteopenia). The data suggest that antiresorptive medications (BPs and DMB) are associated with an increased risk for developing MRONJ. The risk of MRONJ is considerably higher in the malignancy group (<5%) than in the osteoporosis group (<0.05%) [11].
In postmenopausal women with osteoporosis previously treated with oral bisphosphonates, denosumab was associated with greater bone mineral density increases at all measured skeletal sites and greater inhibition of bone remodeling compared with BPs [12].
We are not going to refer in this article to other types of osteonecrosis of the jaws, such as osteoradionecrosis.
Patients and Method
The position papers developed by American Association of Oral and Maxilofacial Surgeons (AAOMS) committee provide the strategies for management of patients with, or at risk for, medication-related osteonecrosis of the jaw (MRONJ) in 2007, 2009, and 2014. In 2022, an update was made and a new position on this entity [11].
The case definition help to differentiate MRONJ from other diseases that present with bone exposures and delays in the healing of alveolar processes. Patients must meet the following 3 characteristics: a) Current or previous treatment with antiresorptive therapy alone or in combination with immune modulators or antiangiogenic medications. b) Exposed bone or bone that can be probed through an intraoral or extraoral fistula(e) in the maxillofacial region that has persisted for more than 8 weeks. c) No history of radiation therapy to the jaws or metastatic disease to the jaws.
Staging
A staging system for MRONJ was introduced in the 2009 AAOMS position paper and then modified in the 2014 position paper to characterize more accurately all aspects of the clinical presentation of MRONJ. The AAOMS system is a useful and widely implemented assessment tool guiding clinicians involved in the care of MRONJ patients.
Patients at-risk
No apparent necrotic bone in asymptomatic patients who have been treated with intravenous or oral antiresorptive therapy.

Stage 0: Male patient 75 years old. With a history of prostate cancer. Consumption of Ibandronate 150 mg/ every 30 days, for 1 year. Necrotic bone exposed post extraction for 18 months. Clinical evidence of a scar with receding gums.
Stage 0 (Non-exposed Bone Variant) Patients with no clinical evidence of necrotic bone but who present with nonspecific symptoms or clinical and radiographic findings. These nonspecific findings, which characterize this variant of MRONJ without bone exposure, may occur in patients with a prior history of Stage 1, 2 or 3 disease who have been healed and have no clinical evidence of exposed bone.
Figure 1 Exposed and necrotic bone or fistulae that probes to the bone in patients who are asymptomatic and have no evidence of infection/inflammation.

Stage 2 Exposed and necrotic bone, or fistula that probes to the bone, with evidence of infection/inflammation. These patients are symptomatic.

Stage 3: Exposed and necrotic bone or fistulae that probes to the bone, with evidence of infection, and one or more of the following:
• Exposed necrotic bone extending beyond the region of alveolar bone (i.e., inferior border and ramus in the mandible, maxillary sinus and zygoma in the maxilla).
- Pathologic fracture.
- Extraoral fistula.
- Oral antral/oral-nasal communication.
• Osteolysis extending to the inferior border of the mandible or sinus floor.
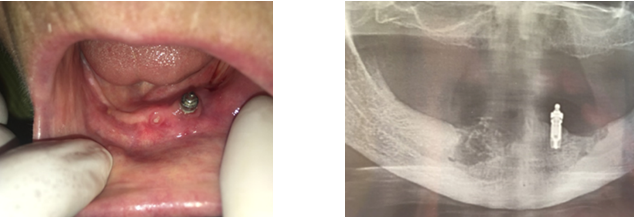
Denosumab (IV every 6 months) for 3 years. Spontaneous implant loss, and suppuration.
| Drug consumed | Consumption Time | Systemic Diagnosis | Previous Dental Treatment | Stage AAOMS | |
|---|---|---|---|---|---|
| F/75 | Denosumab | 3 years | osteoporosis | Implant | 3 |
| F/63 | Ibandronate | 12 months | osteoporosis | Dental Surgery | 2 |
| F/60 | Risedronate | 13 months | osteoporosis | Dental Surgery | |
| F/65 | Denosumab | 3 years | breast cancer/ bone metastasis | Complete Denture | 1 |
| M/80 | Denosumab | 12 months | osteoporosis | Implant | 1 |
| M/68 | Zoledronate | 18 months | kidney cancer | Dental Surgery | 3 |
| M/68 | Zoledronate | 18 months | bone metastasis | Dental Surgery | 3 |
| M/82 | Ibandronate | 20 months | lung cancer/ bone metastasis | Dental Surgery | 2 |
| M/63 | Zoledronate | 18 months | prostate cancer / bone metastasis | Dental Surgery | 0 |
| F/63 | Ibandronate | 3 years | osteoporosis | Complete Denture | 3 |
| F/55 | Ibandronate | 2 years | osteoporosis | Periodontal Disease | Patient at risk |
| M/56 | Bevacizumab/ 5 fluoracilo | 2 years | colon cancer/ bone metastasis | Periodontal Disease | patient at risk |
| F/34 | Zoledronate | 12 months | breast cancer/ bone metastasis | Dental Surgery | 2 |
| M/58 | Zoledronate | 9 months | lung cancer | Periodontal Disease | 2 |
| M/58 | Zoledronate | 9 months | lung cancer | Dental Surgery | 2 |
| F/75 | Everolimus | 18 moths | Breast cancer | Complete Denture | 2 |
| F/75 | Ibandronate | 6 years | osteoporosis | Complete Denture | 1 |
| F/68 | Ibandronate | 10 years | osteoporosis | Dental Surgery | 1 |
| F/62 | Ibandronate | 61 | osteoporosis | Prótesis | 3 |
| F/71 | Ibandronato | 72 | osteoporosis | Protesis/ spontaneous loss of tooth | 2 |
Table 1: Series of clinical cases.
Discussion
The first reports (2003) of the MRONJ were related only to the use of BP (BRONJ=Bisphosphonate-Related Osteonecrosis of the Jaw). The entity’s nomenclature in the literature was modified as cases associated with new therapies were reported [13]. Thus, in 2014, the American Association of Oral and Maxillofacial Surgeons (AAOMS) determined that, in addition to bisphosphonates, Denosumab and antiangiogenic drugs can also cause osteonecrosis of the jaw [14].
MRONJ is a rare but serious disease of the soft and hard tissues induced by several types of drugs. Antiresorptive or antiangiogenic drugs cause drug-induced osteonecrosis. The combination of drugs, microbial contamination, and local trauma induces this condition.
The most common anti-resorptive drugs associated with MRONJ are bisphosphonates, denosumab, and romosozumab.
Bisphosphonates (BP) are a group of drugs used for the prevention and treatment of diseases with bone resorption, such as osteoporosis and cancer with bone metastases, either with or without hypercalcemia, associated with breast and prostate cancer.
Oral bisphosphonates, indicated for postmenopausal osteoporosis, osteopenia, are Alendronate, Clodronate, Etidronate, Risedronate, Tiludronate, Ibandronate, and have less potency than those for intravenous use. The incidence of complications is lower, the estimated risk of developing MRONJ is 0.04 -0.07%, the latency time until the onset of adverse effects is longer (3 years), the evolutionary course of the lesions is less aggressive [15].
Intravenous bisphosphonates are used for the treatment of Paget’s disease, hypercalcemia of tumor origin, osteolytic metastases of solid tumors, multiple myeloma [16]. For example, Ibandronate, Pamidronate, Zoledronate. They are more powerful and have a higher concentration in bone. The incidence of complications is high, the estimated risk of developing osteonecrosis is 0.8 - 12%, the lesions generally appear earlier (6 months), and are much more aggressive and complicated to resolve [17].
Denosumab is a human monoclonal antibody (IgG2) that inhibits the formation, function and survival of osteoclasts, causing a decrease in bone resorption in cortical and trabecular bone with inhibition of osteoclastogenesis and a rapid decrease in bone turnover, which combined to macrophage tissue damage, could trigger the development of MRONJ [18].
RANKL, is one of the important molecules, links bone metabolism and immune response, in several reports, it was shown that RANKL could induce the differentiation of osteoclast precursors by binding to RANK. Nisio, et al. found the increased expression of RANK, RANKL in BPs induced necrotic bone lesions, suggesting that colonizing bacteria that produced lipopolysaccharide could trigger the RANK/RANKL signaling pathway and enhance osteoclast differentiation and activation. It was suggested that osteoclast activation was a protective strategy from the host bone tissue to eliminate the necrotic area and infection. In contrast to BP, RANK-L inhibitors like Denosumab, do not bind to bone, and their effects on bone remodeling are mostly diminished within 6 months of treatment cessation.
Romosozumab is a new monoclonal antibody used for fracture prevention in osteoporotic women. Romosozumab binds to and inhibits sclerostin, and increases bone formation, and decreases bone resorption [19]. In postmenopausal women with osteoporosis who were at high risk for fracture, romosozumab treatment for 12 months followed by alendronate resulted in a significantly lower risk of fracture than alendronate alone [20].
Angiogenesis inhibitors are cancer-fighting substances, they block the growth of blood vessels that support the growth of tumors rather than block the growth of the tumor cells themselves. Anti-angiogenic inhibitors can be divided into three categories, anti-VEGF monoclonal antibody (bevacizumab), VEGF decoy receptors or VEGF- Trap (aflibercept), and small molecule tyrosine kinase inhibitors (TKI) that block the VEGF receptors downstream signaling pathways (sunitinib, cabozantinib, and sorafenib [21]. Fibroblasts are the main cellular components of gum tissue that have an important role in mucosal wound healing. Fibroblasts mainly migrate from the nearby tissues to the wound in response to cytokines and growth factors produced by platelets and macrophages in the wounds [22]. Anti-angiogenic drugs have been reported to inhibit platelet function, affecting the blood clot formation that is used as a scaffold for the migration of different cell players [23].
Anti-resorptive exposure has been associated with gingival fibroblast death and delayed wound healing, which could be attributed to an elevated inflammatory response and immune dysfunction [24]. Anti-angiogenic drugs combined with anti-bone resorption drugs could seriously affect the proliferation and migration of fibroblasts, which may be the cause of unsatisfactory granulation tissue formation, eventually affecting alveolar bone healing [25].
There are local risk factors that contribute to the development of MRONJ, such as the anatomy of the maxillary bones: exostosis, maxillary or mandibular torus, knife-edge edges, acute mylohyoid line. Dental treatments such as tooth extractions or surgeries, implant rehabilitation (placement, bone augmentation, peri-implantitis, extraction), periodontal surgery, endodontic treatment (especially apicoectomy). Dental prostheses, fixed prostheses, ill-fitting dental prostheses that generate areas of mechanical irritation. Other oral conditions like excessive bite force poor oral hygiene and hiposyalia [26].
Systemic risk factors that increase the risk of developing MRONJ are also described, cancer patients, diabetes [27], rheumatoid arthritis, cardiovascular disease (hypertension, hyperlipidemia and angina), Sjögren’s Syndrome, sarcoidosis, hypocalcemia, hypoparathyroidism, osteomalacia, vitamin D deficiency, renal dialysis [28], anemia, Paget’s disease of bone [29].
There are other factors described in the literature such as age, alcohol consumption, tobacco, obesity and advanced age [30].
It has been suggested that polymorphisms in the genes for farnesyl pyrophosphate synthase 185 or cytochrome P450, CYP2C8, could predispose some people to developing MRONJ.
During the development of osteonecrosis, necrotic bone damages local immune function, which leads to uncontrolled inflammation that creates a chronic inflammatory microenvironment, hindering bone regeneration and repair [31].
We can affirm that MRONJ lesions negatively affect the quality of life of patients, especially oncologic patients. Painful lesions affecting the oral cavity negatively influence feeding and the diet.
Conclusion
Dentists should perform appropriate dental treatment to prevent MRONJ in patients before or when receiving medications like antiresorptive drugs or antiangiogenic drugs. In addition, there are treatment strategies for MRONJ at each stage that oral surgeons could follow. It is very useful to carry out the staging of patients who present pathology or at risk of presenting it, thus applying the corresponding treatment protocols. Practitioners prescribing BP, DNS, Romosozumab and antiangiogenic drugs should advise patients about regular dental visits and monitor for symptoms of MRONJ. Dental consultation is mandatory.
Conflicts of Interest: The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
-
Bernardi S, Bianchi S, Continenza MA, Macchiarelli G (2017) Frequency and anatomical features of the mandibular lingual foramina: systematic review and meta-analysis. Surg Radiol Anat 39(12): 1349-1357.
-
Campisi G, Mauceri R, Bertoldo F, Bettini G, Biasotto M, et al. (2020) Medication-Related Osteonecrosis of Jaws (MRONJ) Prevention and Diagnosis: Italian Consensus Update 2020. Int J Environ Res Public Health 17(16): 5998.
-
Nicolatou Galitis O, Kouri M, Papadopoulou E, Vardas E, Galiti D, et al. (2018) Osteonecrosis of the jaw related to non-antiresorptive medications: a systematic review. Support Care Cancer 27(2): 383-394.
-
Giovannacci I, Meleti M, Manfredi M, Mortellaro C, Greco Lucchina A, et al. (2016) Medication-related osteonecrosis of the jaw around dental implants: implant surgery-triggered or implant presence-triggered osteonecrosis? J Craniofac Surg 27(3): 697-701.
-
Zadik Y (2018) Clarithromycin as the empiric antibiotic therapy for medication-related osteonecrosis of the jaw in multiple myeloma patients. Oral Oncol 84: 104-105.
-
Sedghizadeh PP, Kumar SKS, Gorur A, Schaudinn C, Shuler CF, et al. (2009) Microbial biofilms in osteomyelitis of the jaw and osteonecrosis of the jaw secondary to bisphosphonate therapy. J Am Dent Assoc 140(10): 1259-1265.
-
Zhang W, Gao L, Ren W, Li S, Zheng J, et al. (2021) The Role of the Immune Response in the Development of Medication-Related Osteonecrosis of the Jaw. Front Immunol 12: 606043.
-
Saito T, Izumi K, Shiomi A, Uenoyama A, Ohnuki H, et al. (2014) Zoledronic acid impairs re-epithelialization through downregulation of integrin alpha v beta 6 and transforming growth factor beta signalling in a three- dimensional in vitro wound healing model. Int J Oral Maxillofac Surg 43(3): 373-380.
-
King AE, Umland EM (2008) Osteonecrosis of the jaw in patients receiving intravenous or oral bisphosphonates. Pharmacotherapy 28(5): 667-677.
-
Bone HG, Wagman RB, Brandi ML, Brown JP, Chapurlat R, et al. (2017) 10 years of denosumab treatment in postmenopausal women with osteoporosis: results from the phase 3 randomised FREEDOM trial and open-label extension. Lancet Diabetes Endocrinol 5(7): 513-523.
-
Ruggiero SL, Dodson TB, Aghaloo T, Carlson ER, Ward BB, et al. (2022) American Association of Oral and Maxillofacial Surgeons’ Position Paper on Medication- Related Osteonecrosis of the Jaws-2022 Update. J Oral Maxillofac Surg 80(5): 920-943.
-
Miller PD, Pannacciulli N, Brown JP, Czerwinski E, Nedergaard BS, et al. (2016) Denosumab or Zoledronic Acid in Postmenopausal Women with Osteoporosis Previously Treated with Oral Bisphosphonates. J Clin Endocrinol Metab 101(8): 3163-3170.
-
Ruggiero SL, Dodson TB, Fantasia J, Goodday R, Aghaloo T, et al. (2014) American Association of Oral and Maxillofacial Surgeons position paper on medication- related osteonecrosis of the jaw - 2014 update. J Oral Maxillofac Surg 72(10): 1938-1956.
-
Guelman R, Larroudé MS, Mansur JL, Sanchez A, Vega E, et al. (2020) Osteonecrosis De Los Maxilares Asociada A Medicamentos (Onmm). Actual Osteol 16(3): 232-252.
-
Ruggiero SL, Dodson TB, Assael LA, Landesberg R, Marx RE, et al. (2009) American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws-2009 update. J Oral Maxillofac Surg 67(5): 2-12.
-
Caggiano M, Di Spirito F, Acerra A, Galdi M, Sisalli L (2023) Multiple-Drugs-Related Osteonecrosis of the Jaw in a Patient Affected by Multiple Myeloma: A Case Report. Dent J (Basel) 11(4): 104.
-
Ciobanu GA, Mogoantă L, Camen A, Ionescu M, Vlad D, et al. (2023) Clinical and Histopathological Aspects of MRONJ in Cancer Patients. J Clin Med 12(10): 3383.
-
Scott LJ (2014) Denosumab: a review of its use in postmenopausal women with osteoporosis. Drugs Aging 31(7): 555-576.
-
Saag KG, Petersen J, Brandi ML, Karaplis AC, Lorentzono M, et al. (2017) Romosozumab or alendronate for fracture prevention in women with osteoporosis. N Engl J Med 377(15): 1417.
-
Lau EMC, Dinavahi R, Woo YC, Wu CH, Guan J, et al. (2020) Romosozumab or alendronate for fracture prevention in East Asian patients: a subanalysis of the phase III, randomized ARCH study. Osteoporos Int 31(4): 677-685.
-
Zhao N, Li QX, Wang YF, Qiao Q, Huang HY, et al. (2023) Anti-angiogenic drug aggravates the degree of anti- resorptive drug-based medication-related osteonecrosis of the jaw by impairing the proliferation and migration function of gingival fibroblasts. BMC Oral Health 23(1): 330.
-
Barker TH (2011) The role of ECM proteins and protein fragments in guiding cell behavior in regenerative medicine. Biomaterials 32(18): 4211-4214.
-
Landén NX, Li D, Ståhle M (2016) Transition from inflammation to proliferation: a critical step during wound healing. Cell Mol Life Sci 73(20): 3861-3885.
-
Yuan A, Munz A, Reinert S, Hoefert S (2019) Gingival fibroblasts and medication-related osteonecrosis of the jaw: Results by real-time and wound healing in vitro assays. J Craniomaxillofac Surg 47(9): 1464-1474.
-
Zhao N, Li QX, Wang YF, Qiao Q, Huang HY, et al. (2023) Anti-angiogenic drug aggravates the degree of anti- resorptive drug-based medication-related osteonecrosis of the jaw by impairing the proliferation and migration function of gingival fibroblasts. BMC Oral Health 23(1): 330.
-
Kawahara M, Kuroshima S, Sawase T (2021) Clinical considerations for medication-related osteonecrosis of the jaw: a comprehensive literature review. Int J Implant Dent 7(1): 47.
-
Kammerhofer G, Vegh D, Bányai D, Végh Á, Joob-Fancsaly A, et al. (2023) Association between Hyperglycemia and Medication-Related Osteonecrosis of the Jaw (MRONJ). J Clin Med 12(8): 2976.
-
Yoshizawa K, Moroi A, Iguchi R, Takayama A, Goto J, et al. (2021) An unusual case of bone regeneration of a necrotic mandible with pathologic fracture in an elderly hemodialysis patient with medication-related osteonecrosis of the jaw: a case report and review of the literature. J Med Case Rep 15(1): 608.
-
Shimizu R, Sukegawa S, Sukegawa Y, Hasegawa K, Ono S, et al. (2022) Incidence and Risk of Anti-Resorptive Agent-Related Osteonecrosis of the Jaw after Tooth Extraction: A Retrospective Study. Healthcare (Basel) 10(7): 1332.
-
Khan AA, Morrison A, Hanley DA, Felsenberg D, McCauley LK, et al. (2015) Diagnosis and management of osteonecrosis of the jaw: a systematic review and international consensus. J Bone Miner Res 30(1): 3-23.
-
Zheng J, Yao Z, Xue L, Wang D, Tan Z (2022) The role of immune cells in modulating chronic inflammation and osteonecrosis. Front Immunol 13: 1064245.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells