Overview of Periodontal Disease, Etiology, Pathogenesis, Diagnosis and Treatment Therapy
Periodontal Disease is the most common chronic inflammatory bacterial disease that dramatically affects tooth loss and consequent adverse effects not only on the patient's aesthetics and self-confidence but also on the general condition of the body. Because of the high expectation of aggressive behaviour of periodontal disease, the ability to diagnosis and treat early may decrease the risk of tooth loss. So a complete understanding of its silent characteristic is the key. Aim: to thoroughly light on the significance of the early diagnosis and treatment of periodontal diseases which will take part in good prognosis and better outcomes on oral and general health. Methodology: A systematic literature review depends on collecting data from an evidence based studies. Searches were made of twenty electronic databases: the Cochrane Oral Health Group’s Trials Register, The Cochrane Central Register of Controlled Trials (CENTRAL), EMBASE, PsycINFO, Scopus and Web of science, MEDLINE (PubMed). Results: There is a statistically significant clinical improvement in all clinical parameter and biochemical analysis following the periodontal therapy treatment which effect on tooth shelf life. Conclusion: The results proved the benefit of periodontal therapy as a promising treatment therapy in improving periodontal parameters. Understanding the etiology of the progression of periodontal diseases is a very essential step to stopping the disease.
Introduction
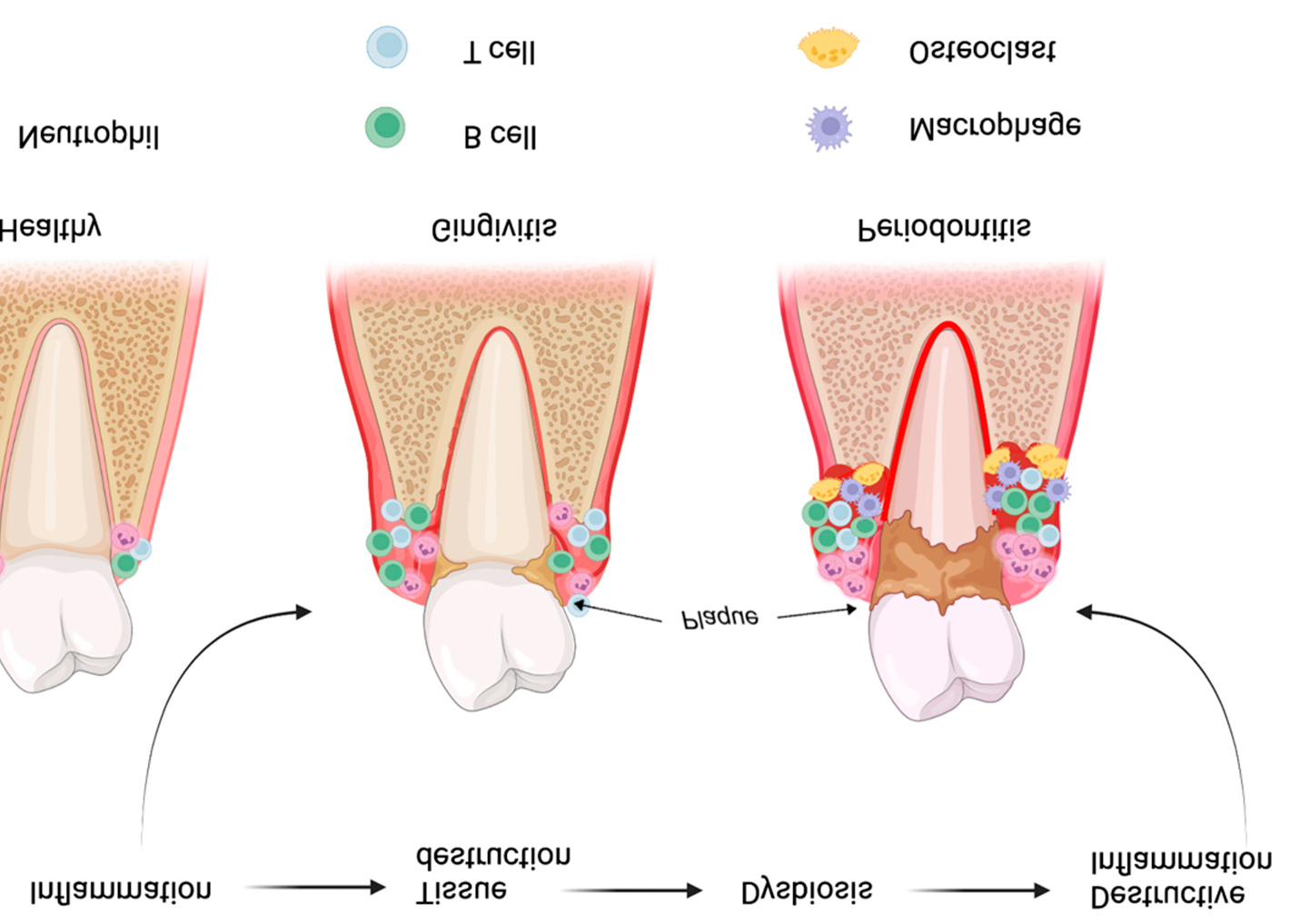
Periodontal disease is a chronic immune inflammatory microbial disease of surrounding supportive structures around the teeth. This disease caused by different micro biomes which already was natural inhabitants in the oral cavity but there is oral dysbiosis occurs due to bad oral hygiene habits which correspond to this state. The most common contributing complex bacterial species are both Gram-negative (Porphyromonas gingivalis, Treponema denticola, Prevotella intermedia, Aggregatibacter actinomycetemcomitans, Campylobacter rectus, etc.) and Gram-positive bacteria (Eubacterium timidum, Parvimonas
micra, etc.). Periodontal disorders are considered asymptomatic in the early stages of the disease ranging from slight inflamed gum and bleeding on probing but later on, the disease becomes more advanced and severe, may reach pocket formation, bone loss, and looseness and at this stage may be difficult to be saved so the time factor is very informative and critical [1, 2].
Plaque biofilm is considered a main etiological factor in periodontal disease which is mineralized into calculus that turns into a niche for precipitating non-calcified plaque, offering ideal places for microorganisms to colonize and metabolize. The tissue damage is based on the interaction between the aggressive microbial factors and the host’s immune reactions. Microbial toxins and enzymes, intensive bacterial growth, and local phagocytic responses lead to odentogingival junctional pathology, chronic inflammation, destruction of the periodontium, and the formation of periodontal pockets. The pathogenicity of microflora to the periodontium is explained by proteolytic enzymes in the bacteria cell wall and the endotoxins that directly stimulate periodontal tissue defence cells to express different inflammatory mediators and cytokines which later result in periodontal tissue destruction. Cytokines are signalling proteins that have the main function of transmitting information between the central nervous system, endocrine system and immune cells. Periodontitis begins with inflammation that extends deep into the tissues and causes the degeneration and destruction of the supporting tissue and alveolar bone. These responses are not only limited to initiating periodontitis but can also have a great impact on triggering systemic conditions such as diabetes, arthritis, and obesity. The idea explained by the chronic inflammation increased macrophage infiltration and proinflammatory cytokines such as TNF-, IL-6 and CRP from the gingival fluid (GCF),serum and saliva [3, 4].
Scientists presented a new classification to categorize periodontal disease conditions according to stages and grades (classification of periodontal and peri-implant diseases and conditions 2018). Stages can be classified according to the severity and extent of tissue loss, and incorporate an assessment regarding the complexity of the long-term management of the patient’s function and aesthetics. Therefore, the severity of the disease and complexity of management are divided into four stages: Stage I: Initial Periodontitis; Stage II: Moderate Periodontitis; Stage III: Severe Periodontitis, with the potential for additional tooth loss; Stage IV: Severe Periodontitis with potential for loss of the dentition.
Grade reflects the risk of disease progression and its effects on systemic health. Grades: is the risk of rapid progression; anticipated response to treatment, Grade A: slow progression, Grade B: moderate progression, Grade C: rapid progression [5, 6].
Periodontal disease considers as destructive irreversible inflammatory disease contributing in gradual bone reabsorption; there are, several enzymes, cytokines, and proteins that lead to these pathogenic process. Clinical periodontal parameters, such as plaque index, probing pocket depth, gingival recession, and tooth mobility were assessed as influential factors for evaluating progress of the diseases. The discovery of the receptor activator of nuclear factor-kB (RANK)/ RANK Ligand (RANKL)/osteoprotegerin (OPG) pathway contributed to the understanding of how bone formation and reabsorption regulated.
RANKL and OPG are members of the tumour necrosis factor (TNF), and binding to receptor activator of NF-kB (RANK) not only regulates osteoclast formation, activation, cell differentiation and survival in normal bone modelling and remodelling but contribute in other pathologic conditions characterized by increased bone turnover. Prognosis of severity of disease can be done by different numerous methods for periodontal diseases diagnostics: bacteriological analysis, the polymerase chain reaction (PCR) method, saliva gas–liquid chromatography and spectrophotometry, pH measurement and proteolytic activity evaluation [7, 8]. Biomarkers Assessment has been commonly used in medical fields to aid the diagnosis, prognosis, and disease monitoring. Moreover it considered a more accurate way to determine the treatment efficacy. RANKL and OPG have been considered as potential critical bone regulator biomarkers of Periodontal Disease. After the initial clinical and radiographic examination, patients were screened, and accordingly, clinical measurements and biomarker evaluations were conducted at baseline, one and three months post-treatment. the sampling sites were isolated, air dried, and isolated with cotton rolls supra-gingival biofilm was gently removed, and then a fine, sterile paper strip was inserted into the pocket until mild resistance was felt and left in place for 30 s. Strips that contaminated with blood or saliva were discarded. The obtained sampled fluid volume in the strip was measured by calculating the resorbed volume per 30 s, and the paper strips were inserted in micro-centrifuge plastic tubes. The obtained samples were stored at 80 _C until being processed for biochemical analysis by enzyme-linked immune sorbent assays (ELISA). Commercially available ELISA kits were used to measure the concentrations of the bone biomarkers: sRANKL and OPG, from the PICF (Biovendor sRANKL (total) Human ELISA (Osteoprotegerin Ligand, OPG (total) Human Osteoprotegerin, Biovendor—Labolatorni medicina a.s— Czech Republic) [9].
Periodontal diseases are a continuous irreversible process which finally ends with loss the tooth and supporting alveolar bone. Every effort should be done to break this cycle to save the tooth and the supportive structure. Proper plaque control is critical for oral health maintenance and to reduce the risk of periodontal diseases development. This need to raise awareness of patient regarding the process of progression of the diseases and how to break it. Several modalities can be used for treatment of periodontal disease such as the non- surgical or surgical treatment of periodontitis. Non-surgical approach involve mechanical debridement of the tooth surface using curettes, ultrasonic devices, or lasers, alone or combined with some sort of chemicals mainly based on local antibiotics or antiseptics such as chlorhexidine [10].
Meticulous oral hygiene of patient should be a routine process and the using of interdental brush and dental flossing in interdental inaccessible area. In the majority of advanced periodontitis lesions, the mechanical non-surgical treatment alone was ineffective, and a surgical approach is suggested in these cases. The most common surgical techniques for surgical treatment are, access flap surgery, the apically positioned flap with or without ostectomy/osteoplasty, and regenerative techniques [11].
The main cornerstone of initial non-surgical periodontal therapy is to remove the supra gingival and sub gingival biofilm and their bacterial products along with calculus elimination to decrease the probing depth and subsequently stop clinical periodontal attachment loss. Sub gingival debridement using hand tools or ultrasound considered an effective in removing bacterial plaque and calculus, decreasing inflammation, and restoring periodontal health. Unfortunately, not all debrided sites show the same satisfactory result, that can be challenged by anatomical factors, accessibility and visibility. Therefore, failure in complete removal of bacterial deposits and calculus after debridement, the more of the depth of the pocket obtained. Evaluation of periodontal therapy through a follow up supportive periodontal program with recall sessions every 3 to 6 months. In case pocket depth less than 6mm, show enhancement in all clinical parameter (such as: probing depth, clinical attachment level, and bleeding on probing) and in bone healing. However the pocket depth that is more than 6mm show defect in bone healing so may need surgical approach for better outcomes. Adjunctive therapy is additional treatment to help increase efficacy of conventional treatment such antimicrobial, and antioxidant treatment [12].
The most common surgical techniques for surgical treatment are, access flap surgery, the apically positioned flap with or without ostectomy/osteoplasty, and regenerative techniques. Each method has specific indications depending on the severity of the situation and the morphology of the bone. Local aesthesia was applied, and each patient used a mouthwash solution of 0.20% chlorhexidine for pre surgical mouth disinfection. Internal bevel incision was done; full thickness flaps were raised to access the osseous defects then removal of granulation tissue and mechanical instrumentation of the root surface.
The instrumentation was followed by thorough cleansing and decontamination of the roots surface using sterilized gauze soaked in chlorhexidine 0.2% solution. After suturing, post-surgical instructions, and analgesics (ibuprofen 400 mg three times a day for four days) were administered to the patients. The sutures were removed about 14 days after surgery, and post-surgical instructions were given to all patients. These included a chlorhexidine 0.12% mouth rinse twice a day for two weeks, and careful tooth brushing with a soft toothbrush so that the sutured area was efficiently cleaned but not traumatized [13].
Surgical periodontal therapy presented a new rational that is based on the application of minimally invasive techniques led to improved outcomes in comparison to conventional surgical techniques. The MIS technique included intramuscular incisions around the involved teeth and a small incision at a distance of 2-3 mm from the top of the interdental papilla buccally, or palatally if it was an aesthetic area. The flap incision was performed with an Orban knife, the size of which was 1/3 or 1/4 of the regular size. Subsequently, the granulation tissue completely removed from the pocket with special rotary instruments, the root surface was smoothened with burs, grafts and membrane were applied and the flap was sutured with vertical mattress sutures. The surgical procedure was performed with 3.5 magnification, the advantages of such techniques, the interdental soft tissues act like a stable “roof”, preventing the loss of volume and contributing to blood fill and clot formation and stabilization, thus preventing the need for additional application of regenerative materials [14].
After complete SRP, scientists Use Scan Electron Microscope examination revealed a consistent finding of the root’s surface cavitation-like defects (also known as lacunar defects). Such defects make a safe area for the development of biofilm, and without complete ablation, these sites will contribute to the infection of the periodontal pockets. EDTA is an antimicrobial and ant biofilm agent. EDTA chelates Ca, Mg, Zn, and Fe and disrupts the cell walls of bacteria, and destabilizes biofilms. EDTA gel has been used as a surface modifier in periodontal root coverage surgeries, e.g., coronal advanced flaps, sub epithelial connective tissue grafts, modified coronal advanced tunnel procedure, etc., to prevent biofilms by inhibiting the adhesion of bacteria and reducing microbial colonization and proliferations. Techniques for using EDTA gel was placed on the scaled root surface for 2 min and then burnished with a sterile cotton pellet. The EDTA was then removed from the root surface by rinsing it with distilled water, will alter the character of smear layer as shown by reductions in the Weight % and Atomic % for N, F, Na, and S and increases in Mg, P, and Ca [15].
Tissue engineering is a regenerative periodontal therapy that is considered a new therapeutic option for, osseous defect or intrabony defect to aid the new tissues grow on a previously diseased root surface. The regeneration of periodontal tissues is considered a promising strategy that promotes immune modulatory potential, proliferation, migration, and multiline age differentiation. Thus, they can be used to repair tissue damage and reduce inflammation, potentially leading to periodontal regeneration. This can be achieved after the surgical implantation of biomaterials that, acting as scaffolds for epithelial cells, create a 3D environment with the biological characteristics that provide cells with an ideal characteristic for proliferation and new fibroblast formation. For scaffold construction, a wide range of materials exist, such as metals, ceramics and polymers. Scaffolds can be of natural or synthetic origin and reabsorb able or non-resorbable based on the nature of their components. In addition to scaffolds, biomolecules are another pillar of tissue engineering. They include cellular adhesion peptides and growth factors that favour cell proliferation such as plasma rich in platelets (PRP), Platelet- Rich Fibrin (PRF) [16].
Patients and Methods
Demographic Characteristics of the Participants
Forty chronic periodontitis patients (15 male and 25 female with age ranged from 23 to 39 years). Clinical measurements of probing depth, plaque index and bleeding on probing were performed at baseline and after periodontal therapy.
- Inclusion Criteria: All patients were free from any systemic diseases.
- Exclusion criteria: Smoker’s patients
Patients Grouping and Interventions
Group I Included 20 chronic periodontitis patients, treated by conventional periodontal therapy (scaling and root planning) combined with intra- pocket application of antioxidant material (Melatonin) as adjunctive therapy to conventional treatment, weekly for one and three months, Group II: included 20 chronic periodontitis patients, treated by SRP combined with the injection of placebo, weekly for one and three months started at the second week after initial therapy. Intra-Pocket Application of 2% Melatonin Gel (Antioxidant Material) The application accomplished by inserting the needle to base of periodontal pocket first and then placing the gel while working the way up until gingival margin. All patients were instructed to avoid eating, drinking and spitting at least 1 hour after application as well as teeth brushing and flossing 4 hour after application. The injections were repeated once weekly for 1 month. Patients were instructed for plaque control regime and oral hygiene instruction were provided every appointment.
Clinical evaluations
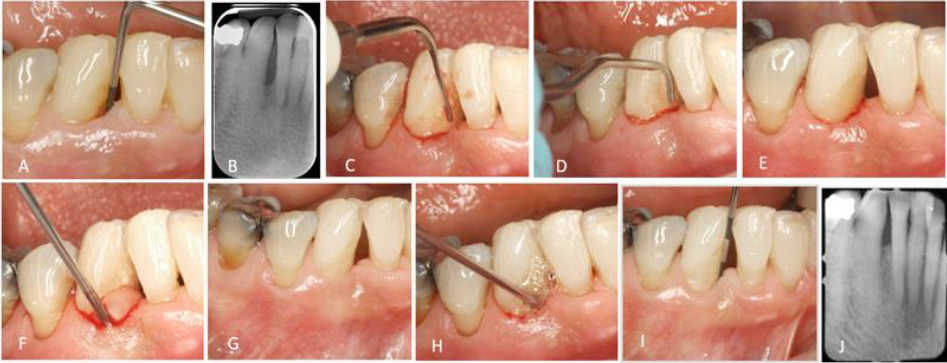
The periodontal status was examined clinically and recorded the diseased sites of each patients (Figure 1) at baseline (at the same day and before initial phase therapy), 1 week, 1 and 3 months using the following clinical parameters:- Plaque Index (PI), Gingival Index (GI), Probing Depth (PD), Clinical Attachment Level (CAL).
Biochemical Evaluation (RANKL levels in Gingival Crevicular Fluid)
The RANKL levels in GCF was assessed using ELISA kits (Sinogeneclon Co., Ltd, China R) at baseline, 1 week, 1and 3 months by sandwich ELISA assay.
Gingival Crevicular Fluid Samples Collection
GCF samples were taken from the deepest periodontal involved sites Figure 1. Prior to sampling supra gingival deposits were removed with sterile cotton pellets without touching the marginal gingival, and the sample sites were isolated with cotton rolls and the reticular site was then dried gently with a syringe. Standardized paper points (META BIOMED Co Ltd, Korea R) size #30 were inserted into the crevice until mild resistance was felt. The paper points were left in pocket for 30 seconds. Paper points which were contaminated with blood and saliva were discarded The collected GCF samples were immediately pooled and diluted in phosphate buffer saline up to 600 μl (PBS; 137 m NaCl, 10 mm Na2HPO4 and 2.7 mm KCl ; pH 7.3) in Eppendorf tube and transported to the lab Figure 2. The samples were frozen at -80°C till they were assayed for RANKL evaluation.
Results
Demographic data, clinical parameters, and RANKL
levels of the patients were summarized in Table 1 at 1 week, 1and 3 months in both groups.
| Group I (Mean ± SD) | Group II (Mean ± SD) | t - test | P - value | |
|---|---|---|---|---|
| GI | ||||
| Baseline | 2.8 ± 0.41 | 2.6 ± 0.5 | 1.378 | 0.109 |
| 1week | 1.6 ± 0.5 | 1 ± 0 | 5.339 | < 0.0001 *** |
| 1month | 0.7± 0.47 | 1.1 ± 0.31 | 3.183 | 0.003 ** |
| 3month | 0.8 ± 0.41 | 1.85 ± 0.37 | 8.536 | < 0.0001 *** |
| PI | ||||
| Baseline | 2.5 ± 0.51 | 2.6 ± 0.5 | 0.623 | 0.205 |
| 1week | 1 ± 0 | 1 ± 0 | 6.332 | < 0.001 ** |
| 1month | 1 ± 0 | 1± 0 | 6.332 | < 0.001 ** |
| 3month | 1 ± 0 | 1.9 ± 0.55 | 7.285 | < 0.0001 * |
| PD | ||||
| Baseline | 4.8 ± 0.41 | 4.9 ± 0.31 | 0.872 | 0.24 |
| 1week | 4.15 ± 0.67 | 4.6 ± 0.5 | 2.401 | 0.01 * |
| 1month | 2.55 ± 0.51 | 3.7± 0.47 | 7.411 | < 0.0001 *** |
| 3 month | 3.25 ± 0.64 | 4.3 ± 0.47 | 5.921 | < 0.0001 *** |
| Attachment level | ||||
| Baseline | 2.8 ± 0.41 | 2.9 ± 0.31 | 0.872 | 0.24 |
| 1week | 2.15 ± 0.67 | 2.6 ± 0.5 | 2.401 | 0.01 * |
| 1month | 0.55 ± 0.51 | 1.7 ± 0.47 | 7.411 | < 0.0001 *** |
| 3months | 1.2 ± 0.7 | 2.3 ± 0.47 | 5.858 | < 0.0001 * *** |
| RANKL | ||||
| Baseline | 13.89 ± 2.13 | 15.43 ± 3.53 | 1.661 | 0.105 |
| 1week | 10.56 ± 1.63 | 12.61 ± 1.96 | 3.593 | 0.001 ** |
| 1month | 10.33 ± 0.82 | 12.81 ± 2.42 | 4.343 | < 0.001 *** |
| 3month | 11.84 ± 1.32 | 13.35 ± 2.05 | 3.1 | 0.004 ** |
Table 1: Means ± SD of Gingival index, Plaque index, Pocket depth, Attachment level, RANKL, paired t- test and P- values in the t
Biomarkers Assessment
The results of ELISA analysis revealed that, both groups I and II showed significant improvement in clinical and biochemical parameters over the study period. But there is a statistically significant positive correlation between PPD,
Diagnosis
Re-Evaluation (Figures 2 & 3)
CAL, and RANKL level at 1-3 months (P < 0.05) especially in group I. This confirm higher RANKL level at baseline refer to periodontal disease activity and lower RANKL level at 1-3 months refer to periodontal healing which was clearly appear with high significant in group I. This result proves the effectiveness of combining LDD as adjuncts to SRP in the healing treatment of chronic periodontitis [17].

Discussion
Periodontal diseases are the most global burden chronic multifactorial diseases caused by plaque biofilm which makes up of multi-complex bacterial species. Periodontitis shares common modifiable risk factors with other major chronic non-communicable diseases such as heart disease, diabetes, and hypertension.
The US Centres for Disease Control and Prevention suggested that it is a pandemic affecting all geographic locations across the globe resulting in loss of teeth with resultant pain and malnutrition, impairment of speech and mastication leading to a poor quality of life for the patient. The pathogenicity of periodontal disease controlled by virulence of pathogen and host immunity state.
There are two mechanisms explain the role of periodontal disease in systemic diseases: Direct Mechanism The endotoxins produced from Gram-negative anaerobic bacteria in the oral cavity directly contribute to systemic disease thorough access periodontal pathogens into the blood circulation so produce collagen degradation, aggregation of platelets and thrombus formation.
Indirect Mechanism
This involves a possible trigger to periodontal pathogens producing inflammatory mediators in the body such as C-reactive protein (CRP), tumour necrosis factor (TNF)-, interleukin (IL)-1, IL-1, IL-6, prostaglandin E2 (PGE2) and matrix metalloproteinase (MMP) causing an autoimmune reaction [18]. Biomarkers have been widely used in several medical fields to aid the diagnosis, treatment outcomes. The RANKL/OPG system has been recognized as a critical bone metabolism regulator. RANKL is the primary factor responsible for osteoclast cell differentiation. The levels of RANKL in GCF were measured by using ELIZA test and high levels of RANKL were reported at baseline in both study groups.
The levels of RANKL showed marked reductions following treatment in both groups. Poor oral hygiene state considered a contributing factor in systemic diseases so there is a strong association between oral health state and systemic. Therefore, good oral hygiene measure and the total removal of bacterial deposits and calculus are the main target for getting appropriate periodontal therapy. There are two rational for periodontal therapy, first the non-surgical therapy by supra gingival and sub gingival debridement to all calculus for the pocket depth not exceed 6 mm. If the periodontal response to this phase is good but residual inflammation and residual deepened periodontal lesions (≥5 mm) are still present, the patient can enter an adjunctive surgical phase. Second Surgical periodontal therapy, thorough open minimal flaps for accessibility, visibility and complete removal of hidden areas which habitant for bacterial microorganism. After periodontal therapy, the patient needs to follow up by supportive therapy for evaluating the outcomes. It was obvious that the clinical parameters measurements show improvement in plaque index, pocket probing depth (PPD), bleeding on probing (BOP), and clinical insertion level (CAL) or bone level (BL). Local Delivery Drug act as adjunctive therapy to initial periodontal therapy which considered as the most effective method than initial therapy alone in treatment of chronic periodontitis.
Adjunctive therapy with periodontal treatment show improvement in regenerative healing capacity which can be appear clearly in improvement of clinical parameter. It was clear that non-surgical therapy is a precursor to surgical treatment. Novel surgical approaches use open flap debridement. The flap incision was performed with an Orban knife, the size of which was 1/3 or 1/4 of the regular size.
Subsequently, the granulation tissue was completely removed from the pocket with special rotary instruments, the root surface was smoothened with burs, grafts and membrane were applied and the flap was sutured with vertical mattress sutures. Regenerative therapy applied in osseous defect repair utilizing components based on tissue engineering. Scaling and root planning alone can leave some microbial and calculus remnant that act as reservoir to collect more and more bacterial biofilm so advisable to use SRP with root conditioning material like EDTA which act to remove the microbes found in sub gingival biofilms. EDTA also alters the character of the smear layer and remaining calculus and so enhance the regenerative capacity of periodontal tissue to heal [19]. Most important points should be consider in regenerative therapy in intrabony defect, level of patients oral hygiene and smoking habits, as both of them have negative results on the treatment outcomes. Regenerative periodontal therapies were used as adjunctive to surgical procedures. Today, the interest of researchers has been focused on regenerative materials and products, mainly three different concepts: barrier membranes, bone grafts, biologic factors, and their combinations. Bone grafts in the treatment of intrabony defects demonstrated an additional CAL gain. Guided Tissue Regeneration (GTR) with the usage of restorable or non-resorbable membranes seemed to enhance the results of the surgical treatment. Also result CAL gain. Koop et al. in a meta-analysis calculated a mean increase in CAL of regenerative treatment protocols, in comparison to gain without regenerative factors [20, 21].
Conclusion
The Relationship between the periodontal state in health and diseases is always changing as the oral cavity has a dynamic environment. Therefore, knowledge of proper oral hygiene is mandatory for preventing bacterial infections. Periodontal therapy is more effective in the treatment of periodontitis. Scaling and root planning are effective nonsurgical procedures that remove hardened plaque deposits and bacteria beneath the gum tissue that are difficult to reach with regular brushing and flossing. Local delivery drugs used as adjunctive method to the conventional scaling and root planning to increase chance of regeneration and healing capacity of periodontal tissues. The RANKL level can be used as effective biochemical marker for diagnosis and treatment of chronic periodontitis. Dentists must present educational messages to their patients regarding learning patient hygiene measures. Regular visits to your periodontics are essential, especially if you have additional health issues such as heart disease or diabetes.
References
-
Herrera D, Meyle J, Renvert S, Jin L (2018) White Paper on Prevention and Management of Periodontal Diseases for Oral Health and General Health. FDI World Dent 20: 1-20.
-
Kinane DF, Stathopoulou PG, Papapanou PN (2017) Periodontal diseases. Nat Rev Dis Prim 3: 17038.
-
Kononen E, Gursoy M, Gursoy U (2019) Periodontitis: A Multifaceted Disease of Tooth-Supporting Tissues. J Clin Med 8(8): 1135.
-
Srivastava MC, Srivastava R, Verma PK, Gautam A (2019) Metabolic syndrome and periodontal disease: An overview for physicians. J Fam Med Prim Care 8(11): 3492-3495.
-
Puetate JCS, Garcia-De Carvalho G, Spin JR (2018) New Classification of Periodontal and Peri-implant Diseases and Conditions: A Brief Review. Dentistry J Clin Periodontol Suppl 20: 1-8.
-
Zeron A (2021) New classification of periodontal diseases. BDJ Open 7.
-
Sakellari D, Menti S, Konstantinidis A (2008) Free soluble receptor activator of nuclear factor-_b ligand in gingival crevicular fluid correlates with distinct pathogens in periodontitis patients. J Clin Periodontol 35(11): 938- 943.
-
Grudyanov A, Zorina O (2009) Methods for Diagnosing Inflammatory Periodontal Diseases: A Guide for Physicians; MIA: Moscow Russia, pp: 112.
-
Petkovic AB, Matic SM, Stamatovic NV, Vojvodic DV, Todorovic TM, et al. (2010) Proinflammatory cytokines (IL-1_ and TNF-_) and chemokines (IL-8 and MIP-1) as markers of peri-implant tissue condition. Int J Oral Maxillofac Surg 39(5): 478-485.
-
Renvert S, Polyzois I (2018) Treatment of pathologic peri-implant pockets. Periodontology 76(1): 180-190.
-
Supranoto S, Slot D, Addy M, Weijden VDG. (2015) The Effect of Chlorhexidine Dentifrice or Gel versus ChlorhexidineMouthwash on Plaque, Gingivitis, Bleeding and Tooth Discoloration: A Systematic Review. Int J Dent Hyg 13(2): 83-92.
-
Ardila CM, Bedoya-García JA (2022) Clinical and Microbiological Efficacy of Adjunctive Systemic Quinolones to Mechanical Therapy in Periodontitis: A Systematic Review of the Literature. Int J Dent pp: 1-6.
-
Renvert S, Polyzois I, Claffey N (2012) Surgical therapy for the control of peri-implantitis. Clin Oral Implant Res 23(6): 84-94.
-
Nibali L, Sultan D, Arena C, Pelekos G, Lin GH, et al. (2021) Periodontal infrabony defects: Systematic review of healing by defect morphology following regenerative surgery. J Clin Periodontal 48(1): 100-114.
-
Gorski B, Szerszen M, Kaczynski T (2022) Effect of 24% EDTA root conditioning on the outcome of modified coronally advanced tunnel technique with subepithelial connective tissue graft for the treatment of multiple gingival recessions: A randomized clinical trial. Clin Oral Investig 26(2): 1761-1772.
-
Miron RJ, Zucchelli G, Pikos MA, Salama M, Lee S, et al. (2017) Use of platelet-rich fibrin in regenerative dentistry: A systematic review. Clin Oral Investig 21(16): 1913-1927.
-
Kotb S, Abo Zaid F, Salama R (2022) Evaluation of The Efficacy of Topically Applied Melatonin Gel as Adjunctive Therapy in Chronic Periodontitis; Randomized Control Trail. Al-Azhar Assiut Dental Journal 5(2): 2561-2568.
-
Nagpal R, Yamashiro Y, Izumi Y (2015) The two-way association of periodontal infection with systemic disorders: An overview. Mediat Inflamm.
-
Harrel SK, Valderrama P, Barnes JB, Blackwell EL (2016) Frequency of root surface microgrooves associated with periodontal destruction. Int J Periodontics Restor Dent 36(6): 841-846.
-
Nibali L, Koidou VP, Nieri M, Barbato L, Pagliaro U, et al. (2020) Regenerative surgery versus access flap for the treatment of intra-bony periodontal defects: A systematic review and meta-analysis. J Clin Periodontol 47(22): 320-351.
-
Koop R, Merheb J, Quirynen M (2012) Periodontal Regeneration With Enamel Matrix Derivative in Reconstructive Periodontal Therapy: A Systematic Review. J Periodontol 83(6): 707-720.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells