Clinical Outcome of Root Coverage Following the Treatment of Multiple Gingival Recession Defects Treated with Vista in Combination with PRF and Zucchelli’s Technique: A Case Series
Background: Mucogingival treatment for gingival recession coverage is very specific and is more predictable when done with a specific technique. Different surgical approaches should be focused more on the basis of their effectiveness, efficacy and efficiency meeting the needs of patient’s aesthetic and functional demand. Aim: The purpose of this case series is to combine the biological properties of PRF and compare both the techniques VISTA and Zucchelli’s to predict the clinical outcome of gingival recession coverage. The case series describe the treatment of gingival recession with bilateral Miller’s class I and II recession (RT1 and RT2) defects extend from canine to premolars by using Vestibular incision sub periosteal tunnel access (VISTA) technique and Zucchelli’s technique with PRF. Clinically gingival recession and width of keratinized gingiva was assessed at the follow up time interval 1 month and 3 months. Based on the clinical outcome, both VISTA and Zucchelli’s technique are reliable for the treatment of multiple gingival recession defect. It also improves the root coverage, and gingival phenotype. The use of PRF with Zucchelli’s and VISTA technique is a substitute in terms of regeneration and enhanced wound healing process.
Introduction
According to the Glossary of Periodontology, gingival recession refers to the exposure of the root surface by an apical shift in the position of the gingiva in relation to the cementoenamel junction [1]. By definition, gingival recession is correlated with clinical attachment loss [2]. Gingival recessions can be localized or generalized, affecting one tooth or multiple teeth in the same patient, and associated with one or more surfaces in the same tooth.
In health, free gingival margin, is located about 1-2 mm coronal to the CEJ, and the level of the epithelial attachment is usually at or slightly coronal to the level of the CEJ [3]. In case of gingival recession, an osseous dehiscence is present and the soft tissues around the tooth (free gingiva, attached gingiva and alveolar mucosa) moved in an apical direction to the CEJ, exposing the root surface to external environment [4]. Histologic studies have shown that in buccal-lingual cross-sections of teeth affected by gingival recession is characterized by a keratinized epithelium, which tends to move apically with an increasing recession depth, whereas the position of the mucogingival junction (MGJ) and the alveolar mucosa tends to remain unaltered [5]. These findings confirm that with the increase of the recession depth, the width of keratinized tissue tends to decrease, which leads to the partial or complete loss of the attached gingiva.
Although numerous factors have been implicated in the etiology of gingival recession in both cross-sectional and longitudinal studies [6]. AAP-EFP World Workshop 2017 concluded that the etiology of gingival recession remains unclear [2]. Several predisposing factors have been suggested: mechanical trauma, plaque accumulation, periodontal phenotype and attached gingiva, cervical restorative margins, dental malposition, high frenum attachment and shallow vestibular depth, orthodontic treatment. Miller classified gingival recession in to four classes namely Class I, Class II, Class III and Class IV. Miller’s classified gingival recessions based on the relation of gingival margin to the mucogingival junction, interdental bone level adjacent to defect area and the height of interproximal papillae. The need for gingival recession management is to prevent the accumulation of etiological factors (plaque and calculus), to prevent tooth abrasion, root caries, to avoid hypersensitivity and the most important is the aesthetic concern of the patients.
Root coverage is a successful and predictable procedure in periodontics [7]. Different surgical strategies in the literature have been proposed for the correction and management of gingival recession’s defects, which include free gingival graft, connective tissue grafts, pedicle flaps, guided tissue regeneration with resorbable or non-resorb able membrane. Recent systematic reviews and consensus reports have concluded that connective tissue grafting seems to be the most effective method of root coverage and is the most extensively documented technique [8]. Surgical procedures used in the treatment of gingival recessions can involve the use of pedicle flaps, free soft tissue grafts, additional adjuncts (e.g. PRP, PRF) and combination of the above-mentioned techniques. There were various modifications in the Coronally Advance Flaps given by Allen, Miller, and Zucchelli & De Sanctis. Coronally advanced flap (CAF) is the most frequent approach for treating gingival recessions and it can be combined with a connective tissue graft (CTG) which is accepted as a gold standard therapy [9].
Raetze in 1985 was the first to use an envelope flap technique for covering isolated gingival recession defects.
He created a partial-thickness envelope that allowed for the insertion of a connective tissue graft. Later, a modification was proposed by AL Allen, et al. [10] for the treatment of multiple adjacent recession defects. Further investigated this approach and coined this technique the “tunnel” approach. The “coronally advanced modified tunnel technique” proposed by Aroca S, et al. [11] and comprises a full thickness flap elevation that carefully separates the entire interproximal papillae from bone and places sutures suspended from composite stops at teeth contact points to prevent the flap from collapsing during healing. The positive aesthetic outcomes are attributable to flap elevation that does not dissect the interdental papillae or does not require any vertical releasing incision. A recent systematic review comparing tunnel techniques and CAF showed that CAF seemed to be associated with higher percentage of complete root coverage than was tunnel when the same grafts (connective tissue or a cellular dermal matrix) were used in both techniques [12].
Periodontal tissue loss is typically treated with various regeneration modalities such as bone grafts, Guided Tissue Regeneration and Growth Factors. Growth Factors are large family of polypeptide growth molecules which enhances the healing by modulating the cell responses such as cell attachment, adhesion, survival, proliferation, chemo taxis and differentiation [13]. The Growth Factors are obtained from autogenous source or by Recombinant technology. Recombinant growth factors have positive effect on experimental studies but clinically less effective due to complex application procedures and high cost. Platelets serve as a major resource of autogenous growth factors because they are the first cells to reach the wound site initiating the haemostasis and healing process [14]. Platelet Rich Fibrin (PRF) was the evaluation of PRP which was used in periodontal regeneration. PRF has the same properties as PRP but it is advantageous over PRP in Osteogenicity, Method of preparation and Lack of thrombus and anticoagulants [15]. The minimal invasive techniques for gingival recession coverage when combined with growth factors it provides unique, satisfactory and more advantageous results in terms of predictable clinical and histological outcome.
Therefore, a clinical trial was tried in the form of case series to combine the biological properties of PRF and compare both the techniques VISTA and Zucchelli’s to predict the clinical outcome of gingival recession coverage.
Case Description
Case 1: Zucchelli’s Technique with PRF
A 33-year-old patient reported to the department of periodontics with a chief complaint of tooth elongation with respect to maxillary right teeth. There was no significant medical or family history and patient had no habits. Clinical examination revealed Millers class I and class II gingival recession (RT1 and RT2) in multiple teeth from 13 to 15. The recession width and depth was measured with UNC-15 probe. There was presence of adequate keratinized gingiva, thin gingival phenotype and good vestibular depth. The gingival thickness was measured with the help of endodontic file and a rubber stopper. The patient was diagnosed with Stage I periodontitis with grade B rate of progression. The first visit of the patient involved phase 1 therapy i.e., scaling and root planning. Oral hygiene instructions were given post procedure, along with 0.12% chlorhexidine mouthwash was prescribed twice daily for 15 days and then patient was recalled after 21 days for the recession coverage technique (Figures 1-5).


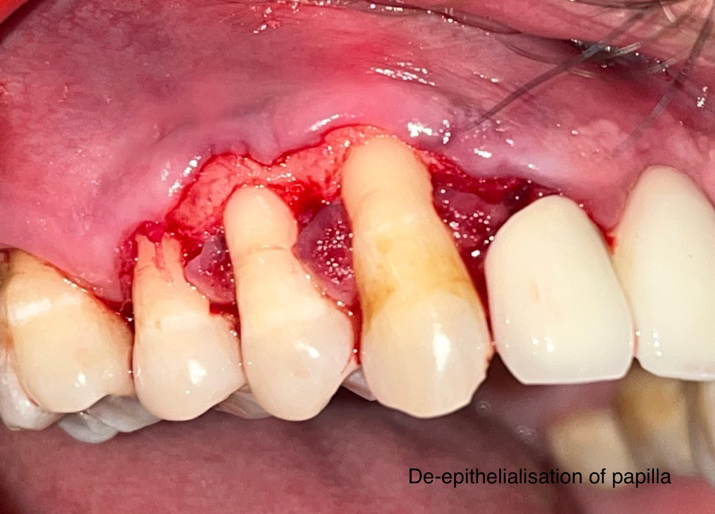

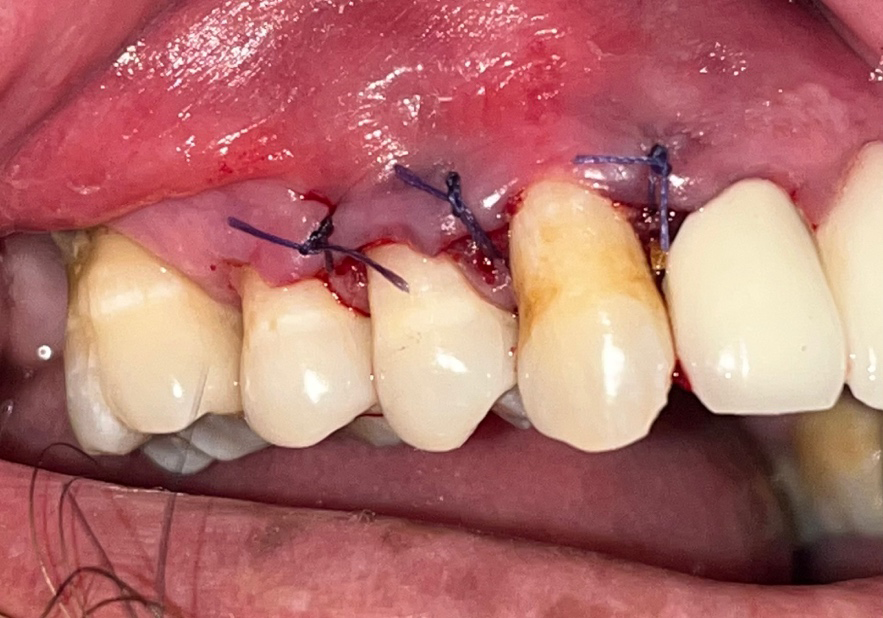
After the administration of local anaesthesia (Lignocaine HCl with 2 % epinephrine 1: 80,000), oblique horizontal incisions were given with a scalpel to modified the form of the flap and connecting the CEJ of one tooth to the gingival margin of the adjacent tooth in order to facilitate the coronal repositioning of the flap tissue over the exposed root surfaces. A split full split thickness envelope flap was reflected in coronal-apical direction till the root exposure and further apically a full thickness flap was raised. Gingival tissue apical to the exposure was raised in a full-thickness manner to provide that portion of the flap critical for root coverage with more thickness. Anatomic interdental papilla was completely deepithelialised with scalpel to expose the underlying connective tissue and to eliminate the epithelium that might interfere with healing. After flap reflection the root surface was examined for presence of any remnant of calculus and thorough scaling and root planning was done. Root conditioning was done with tetracycline. While advancing the flap coronally, surgical papillae were rotated towards the ends of the flap and were displaced on the prepared connective tissue beds of the anatomical papillae. PRF membrane was freshly prepared by drawing 5 ml of blood from anti-cubital vein and was transferred in the test tube and centrifuge was done at 2700 rpm for 12 minutes. The PRF membrane was trimmed and placed underneath the envelope flap to cover the recession defect and for the enhancement of gingival phenotype. The flap was secured in place with 5-0 triclosan coated absorbable interrupted sutures. After the precise adaptation of the flap, the surgical site was then covered with periodontal dressing (Coe pak).
The patient was instructed not to remove the pack or disturb the surgical site. The patient was instructed to avoid tooth brushing in the surgical area. Patient was advised to take antibiotics (Amoxicillin 500mg tds) and analgesic (Ketorol DT10 mg) for 3 days postoperatively. Use of 0.12% chlorhexidine mouthwash twice a day for 15 days was also advised. The patient was recalled after 7 days for removal of periodontal dressing and the area was thoroughly irrigated with normal saline. The surgical site was examined for uneventful healing. The patient was instructed to use soft toothbrush for mechanical plaque control in surgical area. After the follow up of 1 month and 3 months, recession depth recession width and root coverage was assessed.
Case 2: VISTA Technique with PRF
A 38-year-old patient reported to the department of periodontics with a chief complaint of tooth elongation with respect to maxillary left teeth. There was no significant medical or family history and no symptom of sensitivity was reported. Clinical examination revealed Millers class I and class II gingival recession (RT1 and RT2) in 23 and 24. The recession width and height was measured with UNC- 15 probe. There was an adequate keratinized gingiva, thin gingival phenotype and good vestibular depth. The gingival thickness was measured with the help of endodontic file and a rubber stopper. The patient was diagnosed with Stage I periodontitis with grade B rate of progression. The first visit of the patient involved phase 1 therapy i.e., scaling and root planning. Oral hygiene instructions were given post procedure, along with 0.12% chlorhexidine mouthwash was prescribed twice daily for 15 days and then patient was recalled after 21 days for the recession coverage technique (Figures 5-10).


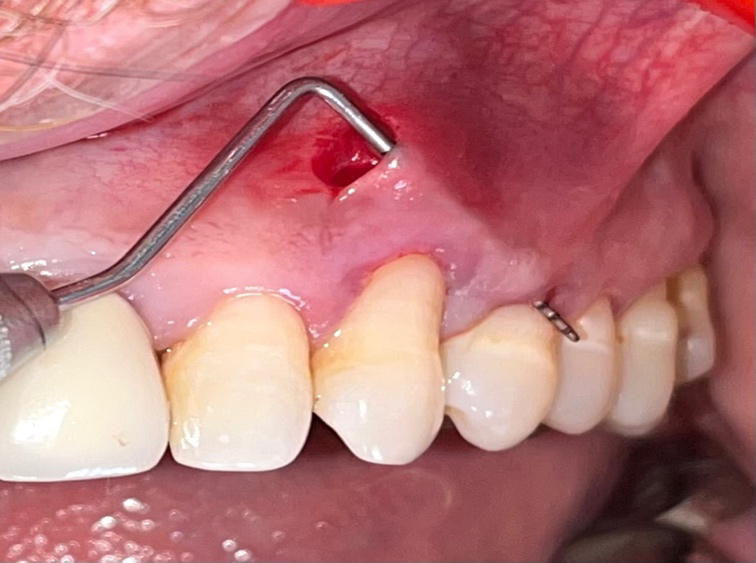
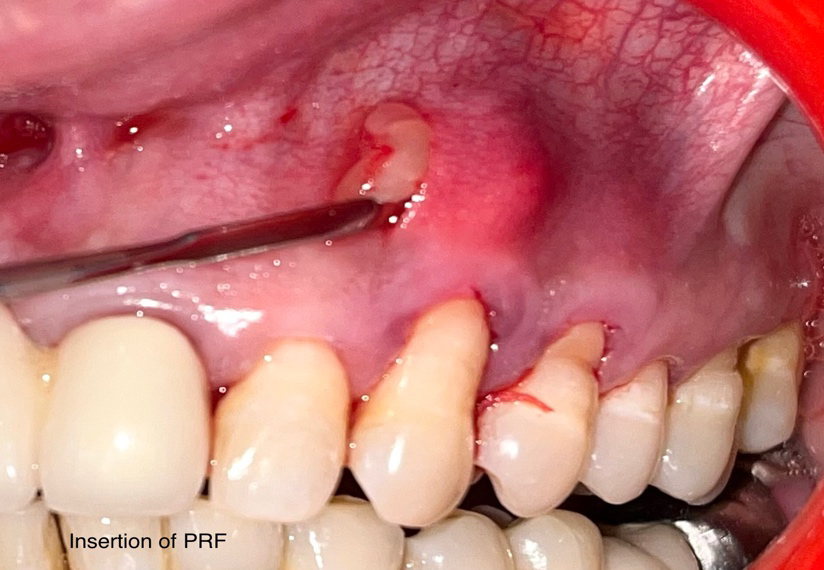
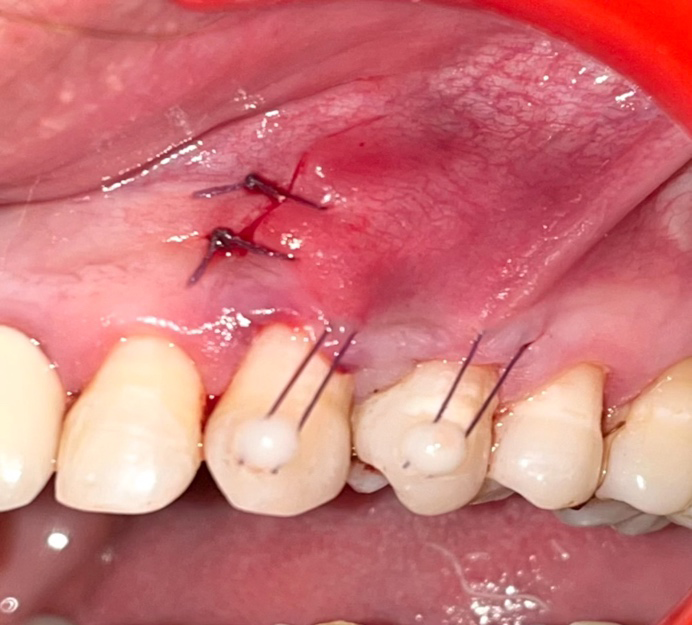
After the administration of local anaesthesia (Lignocaine HCl with 2 % epinephrine 1: 80,000), vestibular incisions were given with a scalpel through the periosteum to create the sub periosteal tunnel, exposing the facial osseous plate and root dehiscence. This tunnel was extended at least one or two teeth beyond the teeth requiring root coverage so as to mobilize gingival margins and facilitate coronal repositioning. The sub periosteal tunnel was extended inter- proximally under each papilla as far as the embrasure space permits, without making any surface incisions through the papilla. The tunnel was extended beyond the mucogingival junction as well as through gingival sulci to allow in order to achieve the low-tension coronal repositioning of the gingiva, once coronal advancement of the gingival margin was established, PRF membrane was freshly prepared by drawing 5 ml of blood from anti-cubital vein and was transferred in the test tube and centrifuge was done at 2700 rpm for 12 minutes. The PRF membrane was trimmed and placed beneath the tunnel and repositioning was done below the gingival margin of each tooth. The membrane and mucogingival complex were then advanced coronally and stabilized in the new position with a coronally anchored suturing using 5-0 triclosan coated absorbable interrupted sutures. Sutures were tied, and the knots positioned at the mid coronal point of each tooth and stabilized at that position by placing composite stops. After the precise adaptation of the flap, the surgical site was then covered with periodontal dressing (Coe pak).
Same instructions were given to the patient as in Case 1. Patient was advised to take antibiotics (Amoxicillin 500mg tds) and analgesic (Ketorol DT10 mg) for 3 days postoperatively. Use of 0.12% chlorhexidine mouthwash twice a day for 15 days was also advised. The patient was recalled after 7 days for removal of periodontal dressing and suture removal along with composite stops and the area was thoroughly irrigated with normal saline. The surgical site was examined for uneventful healing. After the follow up of 1 month and 3 months, recession depth recession width and root coverage was assessed.
Discussion
Root coverage procedure is becoming an important issue in clinical periodontics because of increasing demand for cosmetic treatment. Aesthetics is the main indication for Perio-plastic procedures. The patient exposes the most coronal aspect of the recession while smiling which is considered as the main aesthetic problem. Different techniques have been developed in the literature to cover the denuded roots, with the ultimate goal is complete root coverage, and many attempts have been made to increase the predictability and success rate. While planning and designing for any root coverage procedure, the clinicians must address many aspects of clinical problems such as correction of etiological factors, root preparation, discomfort and healing of donor site wound, vestibular depth and anatomic contour of the recipient sites.
Dental literature has given many treatment modalities for achieving root coverage such as Coronally Advanced Flap, Lateral Pedicle graft, free gingival and Connective tissue graft. A systemic review conducted by Cairo F, et al. [16] has concluded that Coronally Advanced Flap is predictable and safe approach for recession management. Coronally advanced flap is one of the very effective in treatment of recession defects having the advantages for the patient in terms of aesthetics and morbidity. To obtain the highly successful root coverage, modification of the coronally advanced flap procedures is introduced in which there will not be any vertical releasing incision because it might damage the vascular supply to the flap resulting in unesthetic appearance of the affected site with visible white scar. Therefore, this modified approach provides increased probability of achieving complete root coverage and increase in keratinized tissue height.
The present case series demonstrated the effectiveness of the minimally invasive VISTA technique with PRF and Zucchelli’s technique with PRF for the management of gingival recession defects in the aesthetic zone. There was a significant improvement in the root coverage 3 months post operatively. Patient did not report any discomfort during the healing phase and it was an uneventful. Also, patients were overall satisfied with the clinical outcome. Recent studies have shown that the use of growth factors along with VISTA and Zucchelli’s techniques can be an effective tool in the management of multiple gingival recession defects in the aesthetic zone. The recombinant growth factors have proven good results in the experimental and in animal studies. The presence of the Growth Factors in Platelets was first described by Naik B, et al. [17]. Growth Factors which are released from local application enables better tissue regeneration by having a critical role in cell proliferation, survival, migration and angiogenesis [18]. The platelet derived growth factor (PDGF) acts as a power mitogen in the connective tissue cells, stimulation of osteoprogenitor cell is mediated by transformation growth factor -β (TGF-β). The late-stage differentiation of the osteoblasts is promoted by Insulin like Growth factor and Endothelial migration and proliferation is initiated by Vascular Endothelial Growth Factor (VGEF) thus promoting angiogenesis. Luo H, et al. [19] did a systematic review stating the positive effect along with their additional use of Platelet Concentrates in the treatment of Gingival Recessions and wound healing. Placements of PRF membrane in recession defects have been shown with a positive clinical outcome to repair gingival defects, re- establish the continuity and integrity of the keratinized gingiva and increasing the gingival phenotype.
The recession depth and recession width are the two important clinical parameters for gingival recession treatment. Reduction in the recession depth and recession width will result into root coverage and restoration of aesthetics. In the present case series, both the techniques are effective in reduction of recession depth and recession width and shown a significant positive outcome with a follow up time interval of 3 months. Root coverage is the expected and desirable outcome of mucogingival therapy. Clinically, the amount of root coverage is measured as the distance between the CEJ to the gingival margin. In the present case series, using a PRF along with both the technique provide a successful coverage and better aesthetics.
The minimally invasive VISTA technique, combined with PRF, has a number of advantages for the successful treatment of multiple recession defects. Most importantly maintenance of blood supply in the coronally advanced techniques which involve vertical incision is quite compromised. Moreover, the drawback of creation of a palatal donor site after harvesting of autologous soft tissue graft can be overcome by the use of appropriate biomaterial or growth factor such as PRF. PRF is autogenous in origin with evidence for soft tissue healing and can be a promising biomaterial for periodontal therapy. Although large sample and longer follow time period is required to reach the conclusion and for effective evaluation of VISTA technique with PRF and Zucchelli’s technique with PRF. Both the cases documented in this case series are done in the maxillary arch. There is a need of demonstration of these techniques in managing gingival recession in mandibular teeth also. Future research needs to be directed towards the design of randomized controlled clinical trials (RCTs) aimed at evaluating and comparing different mucogingival procedures in the treatment of buccal gingival recessions on maxillary and mandibular anterior teeth. Therefore, more comparative studies and randomized controlled trials are needed in this regard.
Conclusion
The result of both VISTA and Zucchelli’s technique with PRF are effective in treating the multiple gingival recession defect. Multiple gingival recessions are a great challenge to the clinician especially with large defects. Both VISTA and Zucchelli’s technique are reliable techniques for treatment of multiple recession defects. Both techniques require a high level of surgical clinical skill and expertise. Careful patient selection, treatment planning and precise execution are important for achieving optimal results.
References
-
Pini-Prato G, Baldi C, Pagliaro U, Nieri M, Saletta D, Rotundo R, Cortellini P (1999) Coronally Advanced Flap Procedure for Root Coverage. Treatment of Root Surface: Root Planning Versus Polishing. J Periodontol 70(9): 1064-1076.
-
Cortellini P, Bissada NF (2018) Mucogingival Conditions in the Natural Dentition: Narrative Review, Case Definitions, and Diagnostic Considerations. J Clin Periodontol 89(S1): 204-213.
-
Stahl SS (1985) Periodontal Attachment in Health and Disease. J West Soc Periodontol Periodontal Abstr 33(4): 147-157.
-
Stern IB (1981) Current Concepts of the Dentogingival Junction: The Epithelial and Connective Tissue Attachments to the Tooth. J Periodontol 52(9): 465-476.
-
Pini-Prato G (2011) The Miller Classification of Gingival Recession: Limits and Drawbacks. J Clin Periodontol 38(3): 243-245.
-
Kassab MM, Cohen RE (2003) The Etiology and Prevalence Oof Gingival Recession. J Am Dent Assoc 134(2): 220-225.
-
Tatakis DN, Chambrone L, Allen EP, Langer B, McGuire MK, et al. (2015) Periodontal Soft Tissue Root Coverage Procedures: A Consensus Report from the AAP Regeneration Workshop. J Periodontol 86(S2): 52-55.
-
Greenwell H, Fiorellini J, Giannobile W, Offenbacher S, Salkin L, et al. (2005) Oral Reconstructive and Corrective Considerations in Periodontal Therapy. J Periodontol 76(9): 1588-1600.
-
Graziani F, Gennai S, Roldan S, Discepoli N, Buti J, et al. (2014) Efficacy of Periodontal Plastic Procedures in the Treatment of Multiple Gingival Recessions. J Clin Periodontol 41(S15): 63-76.
-
Allen AL (1994) Use of the Supraperiosteal Envelope in Soft Tissue Grafting for Root Coverage. I. Rationale and Technique. Int J Periodontics Restorative Dent 14(3): 216-227.
-
Aroca S, Molnar B, Windisch P, Gera I, Salvi GE, et al. (2013) Treatment of Multiple Adjacent Miller Class I and II Gingival Recessions with a Modified Coronally Advanced Tunnel (MCAT) Technique and a Collagen Matrix or Palatal Connective Tissue Graft: A Randomized, Controlled Clinical Trial. J Clin Periodontol 40(7): 713- 720.
-
Tavelli L, Barootchi S, Nguyen TVN, Tattan M, Ravida A, et al. (2018) Efficacy of Tunnel Technique in the Treatment of Localized and Multiple Gingival Recessions: A Systematic Review and Meta-Analysis. J Periodontol 89(9): 1075-1090.
-
Smith PC, Martínez C, Cáceres M, Martínez J (2015) Research on Growth Factors in Periodontology. Periodontology 2000. 67(1): 234-250.
-
Borzini P, Mazzucco L (2005) Platelet Gels and Releasates. Curr Opin Hematol 12(6): 473-479.
-
Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJJ, et al. (2006) Platelet-Rich Fibrin (PRF): A Second- Generation Platelet Concentrate. Part I: Technological Concepts and Evolution. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101(3): e37-e44.
-
Cairo F, Pagliaro U, Nieri M (2008) Treatment of Gingival Recession with Coronally Advanced Flap Procedures: A Systematic Review. J clin periodontol 35(S8): 136-162.
-
Naik B, Karunakar P, Jayadev M, Marshal RV (2013) Role of Platelet Rich Fibrin in Wound Healing: A Critical Review. J Conserv Dent 16(4): 284-293.
-
Clark RA (2001) Fibrin and Wound Healing. Ann N Y Acad Sci 936: 355-367.
-
Luo H, Li RM, Wang CL, Peng L, Ye L (2015) The Adjunctive Use of Platelet Concentrates in the Therapy of Gingival Recessions: A Systematic Review and Meta-Analysis. J Oral Rehabil 42(7): 552-561.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells